
Abstract
Abstract
Background:
The aim of this study was to evaluate gall bladder visualization in lymphoscintigraphy of extremities.
Methods and Results:
Thirteen patients who had prediagnoses of lymphedema and were referred for lower extremity lymphoscintigraphy to our department were retrospectively evaluated. Lower extremity lymphoscintigraphy with Tc-99m sulfur colloid was performed on the patients, and planar images of the lower extremity and abdominal region were taken in early phase and late phase (at the 24th hour) routinely. Lymphoscintigraphy results of eight patients were normal regarding lymphatic flow or lymph nodes; however, additional pathologic tracer accumulations in gall bladder were observed, which disappeared at 24th hour images in three patients. Five patients had various pathologies regarding lymph flow or lymph nodes. However, there were no patients with gall bladder activity except those three patients who had casual anamnesis of fasting prior to the exam.
Conclusion:
The fasting state of the patients might be the cause of gall bladder visualization during the lymphoscintigraphy of the extremities with sulfur colloid.
Introduction
The liver can be visualized during normal lymphoscintigraphy at late phase due to flow of the radiopharmaceutical into systemic circulation. 3 Gall bladder visualization has been also reported by Tc-99m human serum albumin (HSA) injection. 4 However, gall bladder visualization by Tc-99m sulfur colloid injection has not been reported to the best of our knowledge. In this study, we report findings of our patients and evaluate possible reasons of gall bladder visualization in lower extremity lymphoscintigraphy with Tc-99m sulfur colloid.
Materials and Methods
Thirteen patients (8 F, 5 M; mean age 30.2 years) in the Department of Nuclear Medicine of Firat (Euphrates) University Medical Faculty were evaluated retrospectively.
All the patients had suspicion of primary lymphedema and were referred to our department for lower extremity lymphoscintigraphy. All patients were injected with 0.5 mCi of Tc-99m sulfur colloid (Amerscan Hepatate II Agent, GE Healthcare Ltd, UK) subcutaneously into the first interdigital space of the dorsum of both feet. The radiopharmaceutical was prepared according to the manufacturer's instructions. Static images were acquired after the injection and approximately at 1, 2, and 24 hours covering whole lower extremities, pelvis, and abdomen (including the liver) for 5 min with a double-head gamma camera (GE Infinia) interfaced with a computer. Blockage of the activity or delay in appearance of the lymph nodes or asymmetrical activity accumulation in lymph nodes or dermal backflow were considered as pathological findings.
Results
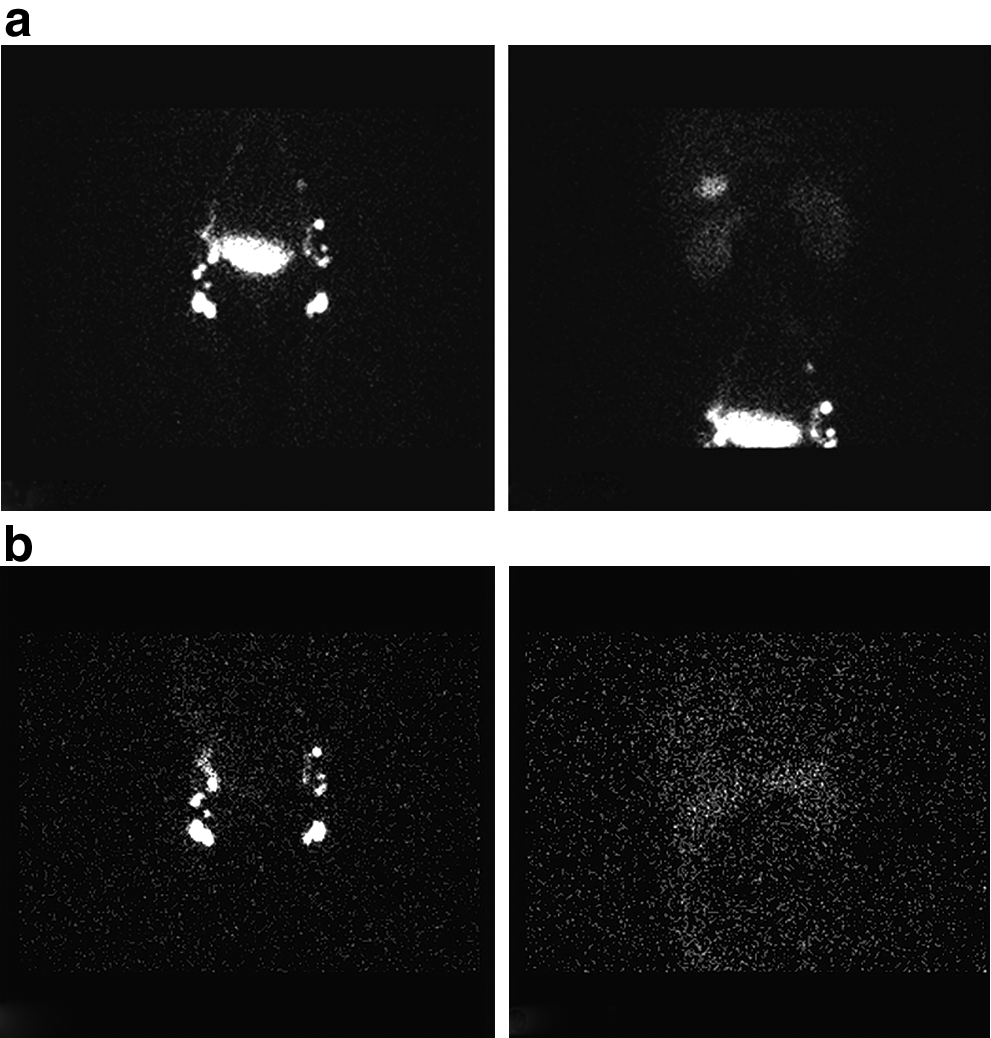
Lower extremity lymphoscintigraphy studies of eight patients were normal; the rest of the patients had some abnormal scintigraphic results related to their clinical condition. Three patients with normal lymphoscintigraphy regarding lymph flow had additional gall bladder visualization on early phase disappearing at next day imaging. Figure 1a (early phase) and 1b (late phase) present images of one of these patients. In the early phase, we can see the gall bladder activity on the second image of upper row and it was disappeared on the next day imaging (second image of the lower row). When we questioned, all of the three patients were in fasting state casually. The other patients who had no gall bladder activity were not fasting.
Discussion
Lymphoscintigraphy has high accuracy in the diagnosis of lymphedema, and dermal backflow and asymmetrical uptake pattern are especially important diagnostic findings. 5 Lymphoscintigraphy is an important diagnostic method if the technique is standardized. 6 Subclinical changes might be identified by lymphoscintigraphy, and also quantification of the images and thus revealing of the pathological process is possible.7,8 Magnetic resonance imaging (MR) was recently introduced in lymphatic imaging. A comparative study with MR showed that scintigraphy is superior in identification of lymph nodes, and MR is superior in discriminating lymph vessel anomalies. 9 However, the diagnostic power of lymphoscintigraphy is extremely high. Besides extremity imaging, sentinel lymph node imaging is another important field in which lymphoscintigraphy is essential. The most important points in radionuclide lymphatic imaging are the particle size and the injection technique. Intradermal injection and smaller particle size provides faster lymphatic clearance; however, larger particle size provides better visualization of the lymph nodes. 10 The best approach in lymphatic imaging would be the selection of method and particle size according to the imaging purpose. Furthermore, there are new agents such as Tc-99m neomannosyl human serum albumin for lymphatic imaging. 11
The liver and gall bladder accumulation of Tc-99m HSA have been previously reported3, 4. The in vivo instability of Tc-99m HSA has been discussed by Jensen et al. 4 Additionally, Jensen et al. have found that the clearance of subcutaneous injection site is slower in Tc-99m HAS. 4
This is the first report to show and explain gall bladder accumulation of Tc-99m sulfur colloid. The three patients with gall bladder accumulation in the lower extremity lymphoscintigraphy were in a fasting state for more than 10 hours before the study. This probably resulted in this unexpected appearance of gall bladder activity. A previous study about gall bladder visualization with Tc-99m methylene diphosphonate concluded that this is a consequence of a minor quality defect of Tc-99m generator because all the quality control results were normal. 12 Intense gallbladder uptake in bone scintigraphy associated with recent chemotherapy administration in three patients has been reported in another study. 13 A previous study addressed the importance of gall bladder activity in Tc-99m mercaptoacetyltriglycine dynamic renal studies and additionally found that gall bladder activity was more prominent in fasting patients than nonfasting patients. 14
Tc-99m labeled colloids may cause hepatic uptake in lymphoscintigraphy, especially at late phase, but gall bladder activity is first described here as far as we know. The liver uptake is a consequence of the leakage of the tracer to the systemic circulation. However, gall bladder uptake may be a consequence of the exceptionally prolonged fasting in these patients. Two of the patients were imaged in the holy month of Ramadan and the other was in fasting state randomly in the course of scintigraphy. A well-known entity called “rim sign” for acute cholecystitis is described for both Tc-99m iminodiacetic acid and Tc-99m colloid hepatic scintigraphy.15–18 Thus, we had suspicion of an inflammatory process in the gall bladder for these patients, although appearance of gall bladder activity was not like the rim sign. However, abdominal ultrasound imaging of the patients was also normal, and visualization of gall bladder in the scintigraphy was transient, so we excluded the inflammation as a cause. We suppose that inhibition of the contraction of the gall bladder because of the fasting state was the reason of the abnormal radiotracer accumulation. We did not have the chance to perform the radiochemical purity measurements. However, we followed the manufacturer's instructions in the preparation of the radiopharmaceutical and we did not observe such an accumulation on the subsequent patients who were imaged on the same day with the same kit. Therefore, probably this coincidence is a result of both the property of radiopharmaceutical (sulfur colloid) and fasting state. A prospective study with patients who have long-length fasting during lymphoscintigraphy is warranted in the identification of this uptake. We believe that this finding is related to in vivo instability of Tc-99m sulfur colloid, especially in the prolonged fasting state. Additionally, although it is very rare, to avoid the incorrect interpretation of the lymphoscintigraphy and not to be in doubt about another gall bladder pathology, we recommend to the patients “to eat something and not to be hungry” before the study. We suggested that this finding has to take part in the relevant gamut.
Footnotes
Acknowledgments
The authors would like to thank Dr. Ayse Murat Aydin from the Radiology Department for performing USG and the Cardiovascular Surgery Department for routinely referring patients with prediagnosed lymphedema for lymphoscintigraphy.
Author Disclosure Statement
No competing financial interests exist.