
Abstract
Abstract
Background:
Compared to volume/circumference measurements to diagnose lymphedema, thickening and disturbance of echogenicity of cutis and subcutis associated with the development of lymphedema is measured directly by ultrasonography. The aim of the present study was to investigate the evolution of thickness and echogenicity of cutis and subcutis of the lower and upper arm after axillary dissection for breast cancer and compare patients with and without arm lymphedema.
Methods and results:
Immediately after the surgery and at 6 and 12 months post-surgery, 42 patients received an ultrasonography of both arms, at the wrist, ventral and dorsal side of the lower arm, and biceps and triceps side of the upper arm. Thickness and echogenicity of cutis and subcutis were determined. Lymphedema was defined as 5.0% or more increase compare to the preoperative value. Eighteen patients had developed lymphedema of the lower arm, and 24 patients of the upper arm. Thickness of the cutis decreased significantly during the postoperative period on the healthy and affected side as well. The difference of cutis thickness between affected and healthy side increased postoperatively in patients with lymphedema and decreased in patients without lymphedema at the wrist and dorsal side of the lower arm. Patients with lymphedema had more frequent disturbance of echogenicity of the cutis at all measurement points. In exception of the triceps, thickness and echogenicity of the subcutis is less obvious disturbed. Sensitivity to detect arm lymphedema by ultrasonography was acceptable for increased subcutis thickness at the ventral lower arm and triceps and disturbed cutis echogenicity at the wrist (67%–100%). Sensitivity for the other measurements was bad. Specificity was for all measurements acceptable (59%–100%).
Conclusion:
Ultrasonography may be useful to diagnose lymphedema developing after axillary dissection for breast cancer. However, it cannot be used as a separate diagnostic test for lymphedema.
Introduction
B
The diagnosis of lymphedema occurs clinically by physical examination of the skin and volume/circumference measurements. Additional investigations may be performed by ultrasonography.7,8 High-frequency ultrasonography is a noninvasive reliable and valid method to measure cutis and subcutis thickness and echogenicity.9–12 In patients with chronic lymphedema, thickness of cutis and subcutis is larger on the affected side than on the healthy side.13–17 The echogenicity of the dermis on the affected side is lower than on the healthy side, indicating intradermal edema.15,17–19 Different patterns of structural changes may be visualized within the subcutis: 1) a uniform hypoechoic subcutis due to diffuse spread of water through the subcutis, 2) hyperechoic areas surrounded by hypoechoic streaks corresponding to adipose tissue surrounded by fluid embedded in fibrous tissue, and 3) homogeneous hyperechoic subcutis due to overgrowth of adipose tissue with a minimal amount of water. 6 Compared to volume/circumference measurements to diagnose lymphedema, thickening of cutis and subcutis associated with the development of lymphedema is measured directly by ultrasonography. Consequently, changes in volume/ circumferences caused by muscular atrophy or hypertrophy are excluded.14,17
To our knowledge, a study about the evolution of thickness and echogenicity of cutis and subcutis up to one year after the axillary dissection for breast cancer and the relation to the development of arm lymphedema is missing.
The aim of the present study was to investigate the evolution of thickness and echogenicity of cutis and subcutis with ultrasonography until one year after axillary dissection for breast cancer, and to compare patients with and without objective lymphedema.
Materials and Methods
Subjects
Forty-five patients with unilateral axillary dissection for primary breast cancer participated in the present study. All patients were recruited in the Multidisciplinary Breast Clinic of the University Hospitals Leuven between September 2008 and February 2009. Patients were excluded if they were physically or mentally not able to participate, had a sentinel node biopsy, or had axillary surgery on the contralateral side. This study had approval from the Ethical Committee of the University Hospitals Leuven (B-number: 32220072574, S-number: 50682). All patients signed informed consent.
Arm circumferences
In all patients, circumferences of both arms were measured before and 1, 6, and 12 months after the surgery. The circumferences were measured at the olecranon and 4, 8, 12, 16, and 20 cm below and above the olecranon with a reliable measurement device. 20 Volume of one segment (between two consecutive circumferences) was estimated by the formula of the truncated cone, V=h(c 2 +cC+C2)/12π, where h is the height and c and C are the circumferences of the segment. 21 The volume of the lower arm was determined by summing all segments from the olecranon up to 20 cm below the olecranon. The volume of the upper arm was determined by summing all segments from the olecranon up to 20 cm above the olecranon. The relative increase of the arm volume on the affected side was calculated as follows: [(VA postop×VH preop)+(VH postop×VH preop)] −1, where VA is the arm volume on the affected side and VH is the arm volume on the healthy side. 22 Since the aim was to detect mild lymphedema, lymphedema was defined as 5.0% or more increase of the arm volume on the affected side. 22
Ultrasonography
The ultrasonographic evaluations of both arms were performed immediately and 6 and 12 months after the axillary surgery. An ultrasound device (Siemens Acuson Antares Premium, Erlangen, Germany) with high-frequency linear probe of 13 MHz was used. An experienced assessor (SP) performed all ultrasonographic measurements and was blinded for the side of axillary surgery. The ultrasonographic measurements were made at the ventral side of the wrist, ventral and dorsal side of the lower arm, and biceps and triceps side of the upper arm. At each measurement site, a sagittal and transversal image was made. The marked reference point was located in the middle of the probe, where a minimal amount of pressure was given. Putting the reference points and performing the measurements is further described in Figure 1.
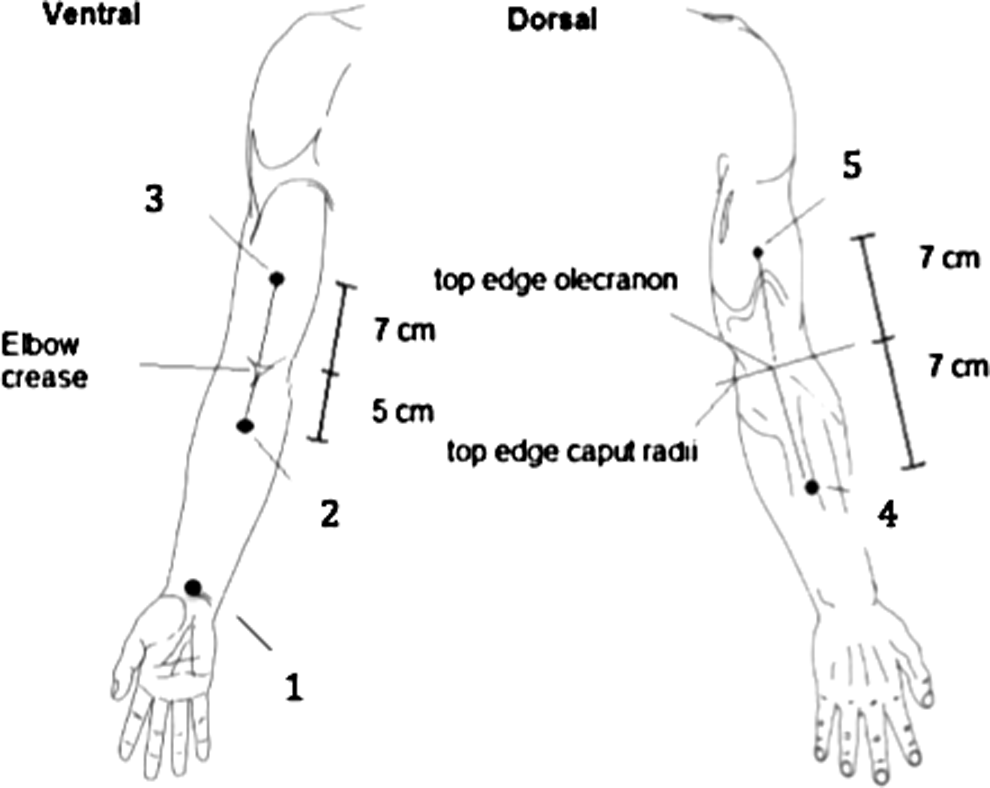
Reference points and sequence of measuring by ultrasonography. 1: wrist, 2: ventral side lower arm, 3: biceps side upper arm, 4: dorsal side lower arm, and 5: triceps side upper arm. Subject in sitting position: for points 1, 2, and 3, arm on table with supination of the elbow; for point 4, pronation of lower arm; for point 5, arm against belly with elbow 90° flexed and supinated.
Analyses
One assessor (SP) performed all analyses of the ultrasonographic images at once (after finishing all measurements) by using Picture Archiving and Communication System (PACS) screens. As during the ultrasonographic measurements, the assessor was blinded for the side of axillary surgery.
Thickness of cutis and subcutis at the different measurement sites was determined objectively on the transversal image, with an accuracy of 0.1 mm. The sagittal image was considered if the border between cutis and subcutis was not obvious. Thickness of cutis was considered as increased when the difference of thickness between affected and healthy side was more than 0.3 mm. Thickness of subcutis was considered as increased when the difference of thickness was more than 20%. In the literature, cut-off values for changed thickness of cutis and subcutis are missing.
Thereafter, echogenicity of cutis and subcutis at the different measurement sites was determined subjectively. The sagittal and transversal images were considered. The assessor rated the images as disturbed or not disturbed.
Statistics
Statistical analyses were performed with SPSS 20.0. A 5% level of significance was applied. To describe the study group, mean and standard deviations for continuous data and number and proportions for discontinuous data were determined.
The evolution of thickness of cutis and subcutis from postoperatively to 6 and 12 months post-surgery was analyzed using ANOVA for repeated measures. Post-hoc analyses were performed with the paired t test. To test the difference in evolution of cutis and subcutis thickness between patients with and without lymphedema, two-way ANOVA for repeated measures was used. Lymphedema had to be present at 6 or 12 months post-surgery, or both. The difference in cutis/subcutis thickness between patients with and without lymphedema was analyzed using independent t test. The difference in cutis/subcutis thickness between affected and healthy side was analyzed using the paired t test.
For the different measurement sites, the proportion of patients with disturbed echogenicity of cutis and subcutis at 1, 6 and 12 months post-surgery was determined. The difference in proportion between patients with and without lymphedema was determined with the Chi2- test.
Sensitivity and specificity were determined to detect lymphedema by ultrasonography. Sensitivity=number of patients with lymphedema and disturbed ultrasonographic image/all patients with lymphedema. A disturbed ultrasonographic image is defined as increased thickness of cutis/ subcutis (see analyses) or disturbed echogenicity of cutis/ subcutis. Specificity=number of patients without lymphedema and non-disturbed ultrasonographic image/all patients without lymphedema.
Results
Of 45 included patients, three patients dropped out. One patient was not interested to continue the study, and the other two patients did not receive an ultrasonography immediately post-surgery. Table 1 gives an overview of the characteristics of the included patients and makes a comparison between patients with and without lymphedema of the lower or upper arm.
Mean and standard deviation for continuous date; frequency and percentage for discontinuous data.
Not normal distributed: median and interquartile range; bIMC, intra-mammary chain.
Cutis—Thickness
Table 2 gives an overview of the evolution of cutis thickness at the different measurement sites from postoperatively to 6 and 12 months post-axillary dissection. A comparison was made between patients with and without lymphedema (developed during the 12 months post-surgery) and between the affected and healthy side.
A, affected side; D, absolute difference between affected and healthy side; H, healthy side.
ANOVA for repeated measures; **Independent t test; ***Two-way ANOVA for repeated measures.
For wrist, ventral and dorsal lower arm: patients with lymphedema of lower arm (N = 18) versus patients without lymphedema (N = 24); For biceps and triceps: patients with lymphedema of upper arm (N = 26) versus patients without lymphedema (N = 16); bSignificant difference between affected and healthy side, p < 0.05.
Postoperative evolution
The thickness of the cutis decreased significantly during the postoperative period at the following measurement sites: ventral part of the lower arm at the affected side and wrist, dorsal part of the lower arm, and biceps and triceps part of the upper arm at the healthy side. There was a significant increase from postoperatively to 12 months of the difference between affected and healthy side at the dorsal part of the lower arm and a borderline significant increase at the triceps.
With versus without lymphedema
Patients with and without lymphedema had a significantly different evolution of the cutis thickness from postoperatively to 12 months post-surgery at the following measurement sites: at the wrist and dorsal part of the lower arm at the affected side. Cutis thickness of patients with lymphedema increased during the postoperative period, whereas cutis thickness of patients without lymphedema decreased during the postoperative period. The difference in cutis thickness between affected and healthy side also increased in patients with lymphedema and decreased in patients without lymphedema at the wrist and dorsal part of the lower arm.
Affected versus healthy side
At the wrist and triceps, thickness of cutis was significantly larger on the affected side than on the healthy side at 6 and 12 months post-surgery. This was also the case in the subgroup of patients with lymphedema, and was not the case in the subgroup of patients without lymphedema. At the ventral and dorsal part of the lower arm, thickness of cutis was also significantly larger on the affected side than on the healthy side and this was also the case in the subgroup of patients with lymphedema, but at certain time intervals also in the subgroup of patients without lymphedema.
Cutis—echogenicity
Table 3 gives an overview of the proportion of patients with disturbance of the echogenicity of the cutis postoperatively and at 6 and 12 months post-surgery. A comparison was made between patients with and without lymphedema.
For wrist, ventral, and dorsal lower arm: patients with lymphedema of lower arm (N = 18) versus patients without lymphedema (N = 24); For biceps and triceps: patients with lymphedema of upper arm (N = 26) versus patients without lymphedema (N = 16); *Chi2-test.
Postoperative evolution
The proportion of patients with disturbed echogenicity of the cutis was similar at the different time intervals post-surgery.
With versus without lymphedema
At 12 and sometimes at 6 months post-surgery, the echogenicity of the cutis was more frequently disturbed in patients with lymphedema (6%–33%) than in patients without lymphedema (0%–13%). Significant difference between patients with and without lymphedema was found at the wrist and dorsal side of the lower arm. Clinically relevant differences were found at the triceps.
Affected versus healthy side
On the affected side, depending on the measurement site, echogenicity of the cutis was in 1 to 7 patients disturbed. On the healthy side, echogenicity of the cutis was disturbed in 1 patient (at each measurement site).
Subcutis—Thickness
Postoperative evolution
With the exception of one measurement site, thickness of the subcutis did not change significantly from postoperatively to 6 and 12 months post-surgery. Only thickness of subcutis on the ventral lower arm at the healthy side decreased significantly from 5.87±2.56 mm postoperatively to 5.79±2.70 mm at 6 months and 5.56±2.79 mm at 12 months (p=0.01) (data not shown).
With versus without lymphedema
With the exception of the triceps, patients with and without lymphedema showed a comparable postoperative evolution of subcutis thickness and also a comparable evolution of the difference of subcutis thickness between affected and healthy side. On the affected side, thickness of triceps increased form 11.4±4.3 mm postoperatively to 12.4±5.0 mm at 6 months and 12.3±4.9 mm in patients with lymphedema of the upper arm, and decreased from 11.4±7.1 mm postoperatively to 11.2±7.4 cm at 6 months and 10.9±7.6 cm in patients without lymphedema (p=0.06). On the healthy side, there was no difference in evolution at all (p=1.00). Consequently, the evolution of the thickness difference between affected and healthy side was different between patients with and without lymphedema of the upper arm (p=0.08).
Affected versus healthy side
For most measurement sites, thickness of subcutis was comparable between affected and healthy side. Only at the triceps, thickness of subcutis was significantly larger on the affected side than on the healthy side 11.42 versus 9.75 mm postoperatively, 11.91 versus 10.26 mm at 6 months, and 11.76 versus 9.95 mm at 12 months; p<0.01. This difference was present in the subgroup of patients with lymphedema and not in the subgroup without lymphedema.
Subcutis—Echogenicity
Postoperative evolution
For each measurement site, the proportion of patients with disturbed echogenicity of subcutis was similar at all time intervals post-surgery.
With versus without lymphedema
The proportion of disturbed echogenicity of subcutis was nonsignificantly higher in patients with lymphedema (11%–39%) than in patients without lymphedema (4%–19%).
Affected versus healthy side
On the affected side, depending on the measurement site, echogenicity of subcutis was disturbed in 3 to 14 patients. Most disturbances were seen at the triceps. On the healthy side, echogenicity of subcutis was disturbed in 0 to 5 patients.
Sensitivity and specificity
At 12 months post-surgery, 15 patients had lymphedema of the lower arm and 21 patients had lymphedema of the upper arm (defined as 5.0% or more increase). Table 4 gives an overview of sensitivity and specificity to detect lymphedema by ultrasonography. For most ultrasonographic measurements, sensitivity was low and ranged between 10% and 43%. Only for disturbed echogenicity of the cutis at the wrist and increased thickness of the subcutis at the ventral lower arm and triceps, sensitivity was higher (100%, 67%, and 67%, respectively). Specificity was remarkably higher and ranged between 59% and 100%.
Discussion
This is the first study investigating the postoperative evolution of thickness and echogenicity of cutis and subcutis up to 12 months after the axillary dissection for breast cancer and making a comparison between patients with and without objective arm lymphedema.
In the present study, thickness of the cutis decreased significantly during the postoperative period on the healthy side and affected side as well. This finding cannot be compared with other studies. Since there is a decrease of thickness of cutis on both sides, it may be induced by the adjuvant treatment. In many pre-menopausal breast cancer patients, chemotherapy contributes to the onset of the menopause. 23 After the menopause, a relative hypoestrogenism exists and leads to a decrease of the thickness of the cutis. 24 This hypoestrogenism is also induced by use of tamoxifen and aromatase inhibitors. In the present study, all patients, except one, received chemotherapy and/ or endocrine treatment as part of the adjuvant treatment. The decrease is not a methodological error caused by the pressure by the transducer. The same, experienced radiologist performed all ultrasonographic measurements. In addition, each ultrasonographic measurement was performed with minimal pressure of the transducer on the skin.
Postoperative decrease of cutis thickness was significantly larger on the healthy side than on the affected side, leading to a postoperative increase of the difference of cutis thickness between affected and healthy side. This increase is probably related to the development of lymphedema, since slight changes in the water distribution of the body influence the thickness of cutis. 18 In the present study, patients with and without arm lymphedema had a significantly different postoperative evolution of cutis thickness difference between affected and healthy sides at the wrist and dorsal lower arm. In patients with lymphedema, cutis thickness difference increased postoperatively, whereas in patients without lymphedema, thickness difference decreased postoperatively. To our knowledge, no other studies compared the postoperative evolution of skin thickness between patients with and without arm lymphedema.
At 6 and/ or 12 months post-surgery, in patients with lymphedema, cutis thickness on the affected side is larger than on the healthy side, at the wrist, dorsal and ventral lower arm and at the triceps. This finding is confirmed by other studies that also found a larger thickness of the cutis in the arm with lymphedema than in the opposite arm.13–17 As expected, in patients without lymphedema, at none of the measurement sites, cutis thickness on the affected side was clinically relevant larger than on the healthy side. Other studies did not perform ultrasonographic evaluations of the skin in patients without lymphedema.
Depending on the measurement site, the echogenicity of the cutis on the affected side was disturbed in 2%–17% of the patients. At 12 months (and sometimes 6 months) post-surgery, the prevalence of disturbed echogenicity of the cutis on the affected side was at the wrist, dorsal lower arm, and biceps and triceps higher in patients with arm lymphedema (8%–33%), than in patients without arm lymphedema (0%–6%). Other studies also found a hypoechoic cutis in the arm with lymphedema compared to the arm on the healthy side.15,17–19 Within the cutis, water is bound to hyaluronic acid, glycosaminoglycan, and proteoglycan. Increase of water content (as in lymphedema development) disarranges and separates collagen bundles resulting in a drop of echogenicity. 15 A negligible number of patients without lymphedema had anyway a disturbed echogenicity of the cutis of the affected arm. The echogenicity of cutis on the healthy side was for each measurement site maximally disturbed in one patient. This is probably caused by a deep venous thrombosis after implantation of a central venous catheter for chemotherapy, that causes venous edema of the healthy arm. 25
In the present study, with exception of the triceps, thickness of the subcutis did not change clinically relevant during the postoperative period and the evolution was comparable between patients with and without arm lymphedema. In addition, thickness of the subcutis of the affected arm was at each measurement site comparable to the healthy arm. In other studies, subcutis thickness of patients with lymphedema was at each measurement site significantly larger on the affected side than on the healthy side.13–15,17 They included patients with severe and chronic lymphedema, whereas the major part of the patients in the present study had mild and recent lymphedema. Mellor et al. mentioned that, in contrast to the cutis, the subcutis is not uniformly increased around the arm. The largest increase in subcutis thickness is at the dorsal aspect of the arm. 14 This was confirmed by the results of our study. We also found in patients with lymphedema, increase of subcutis thickness at the triceps side of the upper arm.
In our study, echogenicity of the subcutis was more frequently disturbed on the affected side (in 7%–33% of the patients) than on the healthy side (0%–19%). The prevalence of disturbed echogenicity of the subcutis on the affected arm was (nonsignificant) clinical relevant different between patients with and without lymphedema at the wrist, dorsal lower arm and biceps and triceps.
From the present study, it seemed that, increased subcutis thickness of the ventral lower arm and of the triceps and changed echogenicity of the cutis at the wrist are good indicators to identify a patient with lymphedema (sensitivity=67%–100%). The other ultrasonographic measurements are poor indicators to identify a patient with lymphedema (sensitivity=10%–43%). Absence of increased thickness of cutis/subcutis and changed echogenicity of cutis/subcutis are good indicators to identify a patient without lymphedema (specificity=59%–100%).
The present study had several strengths. Patients were assessed at fixed time intervals post-surgery. One experienced radiologist made all ultrasonographic images and performed all analyses and was blinded for the side of axillary surgery. Experienced physical therapists performed the circumference measurements with a reliable measurement device. 20 Lymphedema was defined in a relative way and accounted for the preoperative arm volume difference and the postoperative change of arm volume (due to weight change, for example). The present study did not only report the change of cutis and subcutis in lymphedema patients as others did,13–15,17 but also made a comparison between patients with and without lymphedema. A weakness of our study was that the participants did not receive an ultrasonography of cutis and subcutis before the axillary surgery. However, the interval between the axillary surgery and ultrasonography was only 5 days on average.
In the future, the use of ultrasonography to detect the development of breast cancer-related arm and breast lymphedema has to be examined further. The postoperative change of thickness and echogenicity of cutis/subcutis has to be compared with the extracellular fluid content in the arm, for example, by performing bioelectrical impedance analyses.26,27 In clinical trials about the effect of physical therapy on the prevention and treatment of lymphedema, it is besides assessment of lymphedema volume and quality of life, also interesting to evaluate the change of cutis/subcutis thickness and echogenicity.
Conclusions
To detect the development of arm lymphedema during the first year post-surgery by evaluating the postoperative increase of cutis thickness of the affected arm, it is also necessary to measure the healthy limb (to correct for the decrease of cutis thickness related to chemotherapy and/ or endocrine treatment). Also for the evaluation of the postoperative change of subcutis thickness, it is necessary to assess both limbs (to correct for the change of subcutaneous fat tissue). Development of lymphedema induces initially an increase of cutis thickness and disturbance of its echogenicity. In the case of chronic and more severe lymphedema, there are also changes of subcutis thickness and its echogenicity. Since sensitivity of ultrasonography to detect lymphedema is not perfect, ultrasonography may be used to confirm the diagnosis of lymphedema and is not a separate diagnostic test. In case of unchanged cutis or subcutis thickness or normal echogenicity, there is a great chance the patient has no lymphedema.
In conclusion, in breast cancer patients, ultrasonography may be useful to diagnose arm lymphedema; however it cannot be used as a separate diagnostic test.
Footnotes
Acknowledgments
This study was funded by the agency for Innovation by Science and Technology (Applied Biomedical Research) (IWT 60519). We thank all patients who participated in our study. Furthermore, we thank Hilde Lemkens and Ine Van Nuland for performing the circumference measurements. Finally, we are grateful to the nurses and medical staff of the Department of Radiology for their cooperation in the study.
Author Disclosure Statement
The authors declare that they have no conflicts of interest.