
Abstract
Abstract
The association between lymphatic malformations and congenital venous ectasia is extremely rare, and the relative rarity of both entities makes it difficult to determine the relationship between the two. Here we present four new cases and review the current literature. We hypothesize that there might be a strong association between mediastinal lymphatic malformations and segmental phlebectasia; furthermore, there is a molecular background that may justify the association between these two entities.
Introduction
L
Material and Methods
Four patients with a mean age of 4.8 years (range, 1.2–8) were evaluated in the context of LM of the mediastinum and were found to have abnormal dilatations of thoracic large veins. We obtained informed consent from the parents, guardian, or conservator of all the patients for their medical data to be used in a study. LM was combined (macro and microcystic) in all patients involving mediastinal organs as well as part of the neck in three patients, and upper limb in two. Lung parenchyma was unnaffected and no pleural effusions were observed. Cardiac function was normal in all patients.
Results
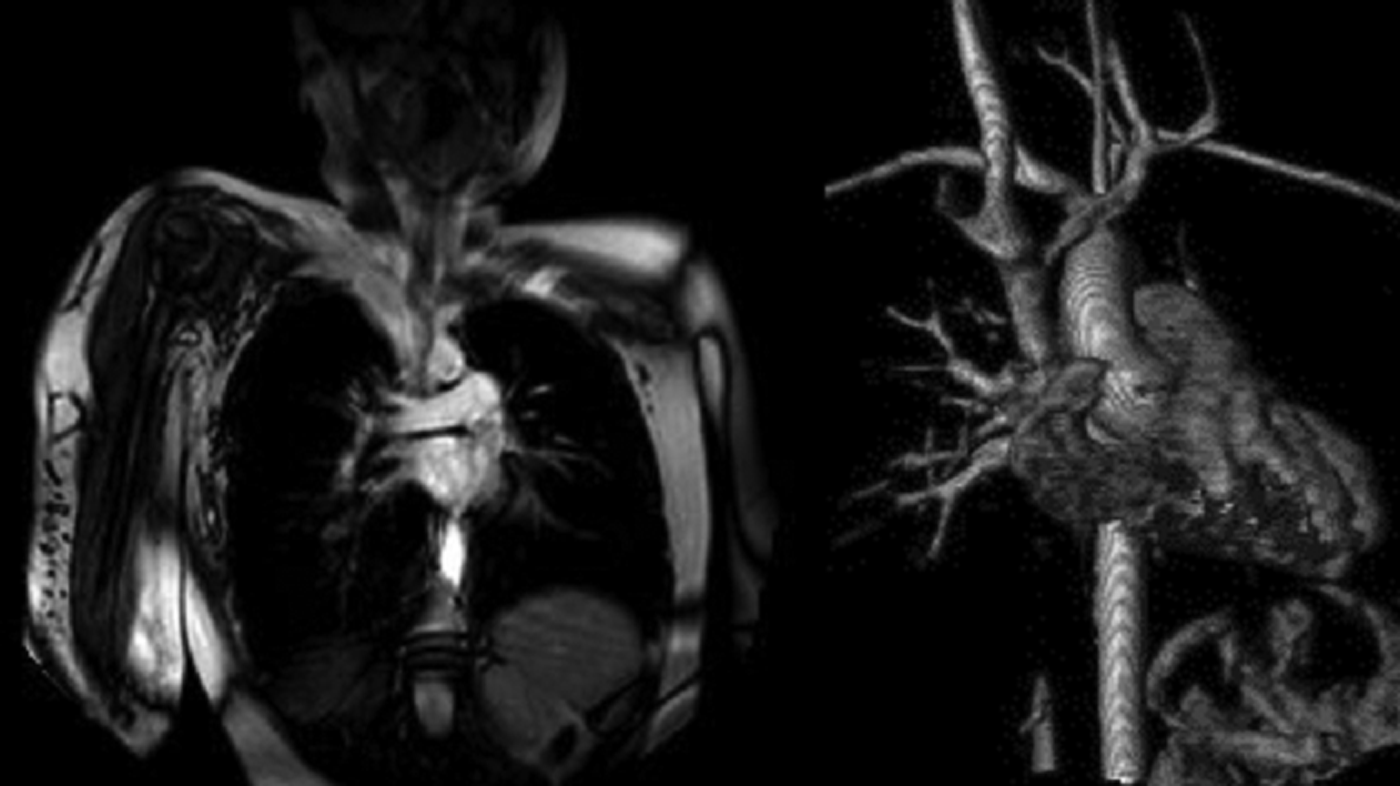
In patient 1, a 4-year-old male, magnetic resonance imaging (MRI) first and angio CT later confirmed a multicystic mediastinal, left supraclavicular and cervical mass and a dilatation of the subclavian vein, internal jugular vein and brachiocephalic vein with a maximum diameter of 36×28 mm (Fig. 1). In patient 2, a 15-month-old female, a multicystic right mediastinal mass with supraclavicular extension and a dilatation of the superior vena cava (SVC) with a maximum diameter of 21 mm was observed (Fig. 2).An upper right limb phlebography in this patient revealed a dilatation of the SVC displaced laterally, without significant relationship with the thoracic mass. Patient 3 was a 6-year-old female with a predominantly macrocystic right paracardiac mass with supraclavicular and vertebral extension and a dilatation of the SVC with a maximum diameter of 20×30 mm and 38 mm of length, presenting a normal diameter at the most distal part of the SVC (Fig. 3).Patient 4 was a preterm girl with a thoracic and right upper limb mass diagnosed by prenatal ultrasound, in association with a right basilic vein enlargement and axilary vein aneurysm (Fig. 4).She underwent surgical exploration at first month of life for intrathoracic mass resection. At 8 years of age, the patient presented with an acute thrombosis of the right cephalic vein, and an acute pulmonary embolism that required hospitalization and long-term anticoagulant therapy. At 18 months follow-up, the patient is asymptomatic, with no evidence of local recurrence and no change in the diameter of the aneurysmatic vein. No extrathoracic aneurysms, dismorphic features, lipomas, syndactily, overgrowth, or syndromic associations were found. Two patients underwent surgical excision of the LM due to airway compression symptoms. Enlarged veins were left untreated without signs of progression in size.

Case 1: Magnetic resonance shows a dilatation of the subclavian vein where it joins with the internal jugular vein to form the brachiocephalic vein.

Case 2: Thoracic CT with 3D reconstruction shows a multicystic right mediastinal mass with supraclavicular extension and a dilatation of the SVC with a maximum diameter of 21 mm, as well as the subclavian and internal jugular veins.
Case 3: Magnetic resonance shows predominantly macrocystic right paracardiac mass and with supraclavicular and vertebral extension and a dilatation of the SVC.
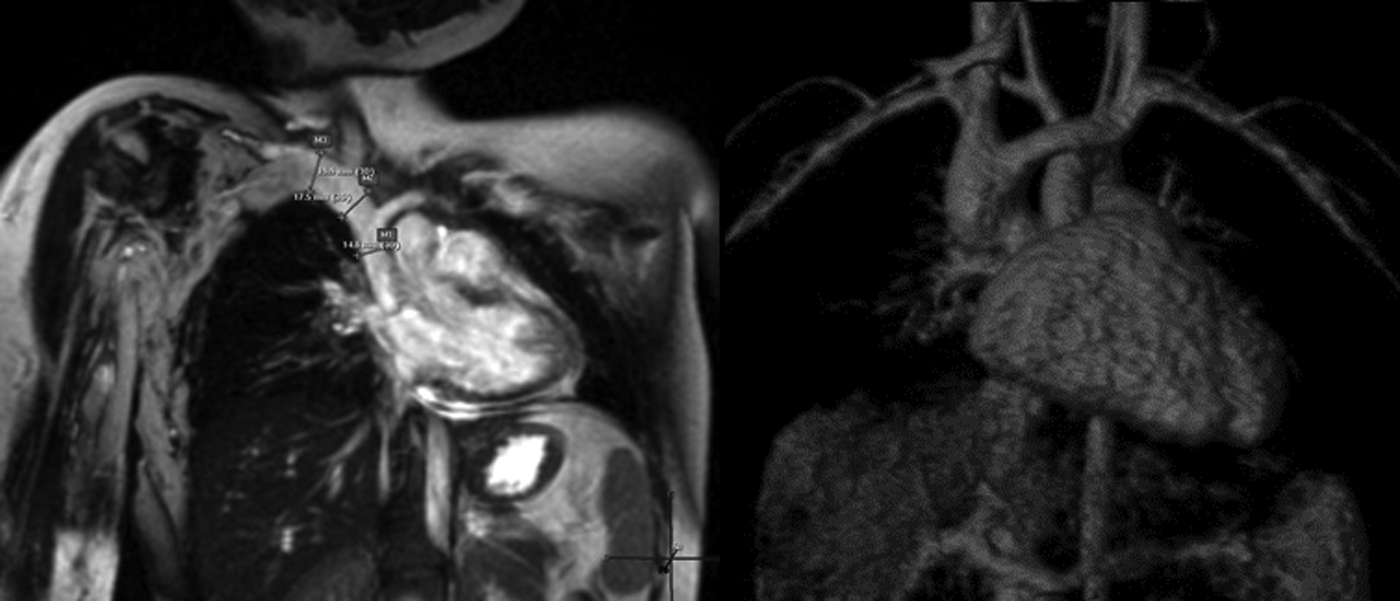
Case 4: Magnetic resonance shows enlargement of the right basilic, axilary and subclavian veins. Lymphatic malformation can be seen on subcutaneous tissue of the right arm and the chest wall.
Discussion
The association between lymphatic malformation and congenital venous ectasia is extremely uncommon, and the relative rarity of both entities makes it difficult to determine the relationship between the two; however, previously reported cases, in conjunction with the present patients, support that the coexistence of mediastinal lymphatic malformations and abnormal venous dilatation may not be just coincidental. For unknown reasons the neck is, by far, the most frequent anatomical location for idiopathic phlebectasia.
Embryologically, the lymphatic system develops in close relation to the venous system and is identified in the embryo as early as the end of the fifth week of gestation. In normal embryos, the main lymphatics develop from different sources including the venous walls, but they subsequently lose their connections with the veins to form a separate lymphatic system, except for the juguloaxillary sacs, which drain the lymph to the venous system, as well as from lymphangioblasts (mesenchymal precursor cells).
The recent advent of molecular markers and methods for analyzing the formation of the lymphatics has permitted a more conclusive re-examination of the origins of lymphatic endothelial cells (LEC) in a number of different developmental model organisms. 2
Although microcystic and macrocystic lesions have different clinical behavior, they have indistinguishable histological features and immunohistochemical staining for markers of lymphatic endothelium. These findings suggest that both microcystic and macrocystic lesions are derived from similar tissue but may behave differently based on their anatomic microenvironment. 3 The cause for the different localization of microcystic and macrocystic lymphatic malformations is still not clarified. 4
The origins of avian lymphatics have been studied using quail-chick embryo chimera grafting experiments. Endothelium of quail (but not chick) blood and lymphatic vessels can be marked using a specific antibody, QH1. Quail somites grafted into the wing level in chick embryo hosts contributed QH1/VEGFR3-positive lymphatic endothelial cells to the wing, suggesting that at least some peripheral lymphatic endothelial cells originate in paraxial/somitic mesoderm. 5 A subsequent study using quail-chick chimeras and DiI-conjugated LDL labeling of blood vascular endothelium suggested that the deeper lymphatics of the jugular sac have a dual origin, arising both from adjacent veins and from lymphangioblasts derived from local mesoderm. 6
LMs arise as a result of abnormal communications between the developmental lymphatic sacs and the venous system. It is therefore quite plausible that a developmental defect might affect both systems. A possible mechanism for increased translucency is dilatation of the jugular lymphatic sacs, because of developmental delay in the connection with the venous system, or a primary abnormal dilatation or proliferation of the lymphatic channels interfering with a normal flow between the lymphatic and venous systems. 7
Lymphatic and blood vasculature are difficult to differentiate when the histologic morphology of the two systems is the only basis on which the distinction is made. Recently, the identification of several markers that show different profiles of expression in blood and lymphatic vasculature has facilitated a detailed analyses of the development and pathologic role of the lymphatic vasculature. Because a variety of growth factors and receptors involved in the angiogenesis process have been identified, the molecular mechanisms that control the development of the vascular system are now being deciphered. In contrast, the mechanisms involved in the development of the lymphatic system are still poorly characterized.8,9
Events effecting genes critical to the correct function of the venous system can occur at any level of the organization of DNA and diffuse segmental ectatic veins have been found to be associated with several congenital disorders (CLOVES syndrome, Klippel Trenaunay syndrome, Bockenheimer disease, or Menkes disease), some of which have a strong hereditary component. 10
Several studies have suggested that venous compliance is highly dependent on genetic composition and an individual carrying the susceptibility loci will have a higher risk of developing a venous disease. Downregulation of desmuslin gene expression has been noted in the smooth muscle cells of incompetent varicose veins. The desmuslin gene is located at chromosome 15q26.3 and encodes the protein desmuslin, which belongs to intermediate filament protein family and is located in the smooth muscle cell cytoplasm.11–13
Interestingly, mutations in the FOXC2 gene cause lymphedema distichiasis syndrome in which 50% of patients have abnormal dilated veins.
Despite molecular evidence of correlation between lymphatic and venous development, the association of aberrant venous wall formation in the thorax and neck when surrounded by a lymphatic malformation remains unexplained. Thirty-five patients treated at our center with generalized lymphatic anomaly (GLA) were reviewed without finding history of vein aneurysms. Fifty-four patients with progressive osteolysis caused by lympathic malformations treated at our hospital were reviewed as well, without history of vein aneurysms. 14 Similar results were found in our group of children with large or giant LM in the abdominal area or lower limbs. Genetic studies including full exome sequencing are currently being performed.
Table 1 gives an overview of the existing literature regarding mediastinal lymphatic malformations associated with venous ectasia.
SVC, superior vena cava.
Surprisingly, 8 patients of the 13 published in the literature had both mediastinal and neck LM in association with venous ectasias. From our series, patient 1 had neck, left upper limb, and mediastinum LM in association with left subclavian vein and innominate vein enlargement.
Bisdorff confirmed a strong association between periorbital LMs/lymphatic venous malformations and intracranial vascular anomalies. In fact, it is known that patients with extensive facial venous malformations have a high incidence of associated intracranial developmental venous anomalies. 19
In any case, we recommend that infants with thoracic LM undergo contrast-enhanced MRI of the thorax soon after clinical diagnosis is made, to identify those patients who require additional treatment or observation. Once diagnosis is obtained, the use of continuous-wave Doppler may be most helpful in the follow-up of venous aneurysms. 20
Making decisions about management of mediastinal LMs is challenging since most of patients do not develop symptoms, and total excision is uniformly unfeasible. Current treatment methods include surgical resection, sclerotherapy, or a combination of both. Surgery used to be the mainstay or even the only treatment of choice. However, with technical advancements and accumulation of clinical experience in sclerotherapy, many authors agree that the treatment plan of LMs should depend on the primary sites and type of the lesions, rather than using surgery as the only effective treatment option.
Management of venous aneurysm remains controversial. There is an agreement that the majority of venous aneurysms in the adult population should be managed surgically to avoid their potential morbidity, such as pulmonary thromboembolic disease, rupture, and partial or total venous compression with subsequent obstruction, and sometimes, death. 21 Unfortunately, an international consensus about the best timing for venous aneurysm repair is lacking and experience in small children is anecdotal. Therapeutic guidelines and indications for surgery have not been clearly established. Operative intervention may consist of tangential excision and lateral venorrhaphy or excision with or without interposition grafting. 22
Conclusion
The association between mediastinal congenital thoracic LM and venous ectasia is extremely rare. The relative rarity of both entities makes it difficult to determine the relationship between the two; however, it seems unlikely that their coexistence may be just coincidental. We hypothesize that there is a molecular background that justifies the association between these two entities. Treatment guidelines for the management of this entity in the pediatric population are not yet established and an international consensus in order to decrease its significant morbidity and mortality when left untreated is needed.
Footnotes
Author Disclosure Statement
Drs. Soares-Medina, López-Gutiérrez, MD, PhD, Fernández-Pineda, and Vivas have no conflicts of interest or financial ties to report.