
Abstract
Abstract
Purpose:
Early detection and timely intervention have potential to reduce late-stage lymphedema (LE) in patients with breast cancer undergoing axillary lymph node dissection (ALND). This study aims to determine if detection and early treatment of subclinical LE by using prospective monitoring with bioimpedance spectroscopy (BIS) can lead to reduced development of clinical LE.
Methods and Results:
Subclinical LE was prospectively detected using an L-Dex® U400 analyzer to measure BIS in 186 patients who underwent ALND between 2010 and 2013 through our LE monitoring program. Baseline measurements were obtained and at 3–6 month intervals for 5 years. Patients diagnosed with subclinical LE received short-term physical therapy, compression garments, and education about exercise, elevation, infection precautions, BMI, and hand usage. The control group had a preoperative baseline L-Dex® measurement, but had only clinical follow-ups with circumferential arm measurements. Mean age and BMI were 56 years and 28.3 kg/m2, respectively. The majority of the women underwent mastectomy (61%) and received chemotherapy (89%) and radiotherapy (77%). Thirty-three percent patients who had repeated L-Dex measurements were diagnosed with subclinical LE and received early intervention. Progression to clinical lymphedema occurred in 4.4% over an average of 20 months follow-up. In the control group, the incidence of clinical LE was 36.4%.
Conclusion:
Periodic monitoring of women at high risk for LE with BIS allows early detection and timely intervention for LE, which reduces the incidence of clinical LE from 36.4% to 4.4%. This may have implications for quality of life and health care costs.
Introduction
L
Early detection and timely intervention hold great promise in reducing incidence of late-stage lymphedema (LE) in patients with breast cancer undergoing ALND. 12 The components of our LE education, monitoring, detection, and reduction program include individual consultation with a physician, one-on-one education, and quarterly group meetings. These meetings facilitate dialogue among health care providers (physicians, nurses, physical therapists, and dieticians) and breast cancer survivors at risk for lymphedema. Early diagnosis of LE, particularly in the subclinical phase, facilitates early interventions such as education (hand usage, limb elevation, infection precaution, and weight reduction), and preventative and treatment recommendations (ready-made compression sleeves, physical therapy consultation, daily exercise, and avoiding overuse of the affected arm). Clinically apparent LE presents as visible or palpable tissue swelling, and diagnostic criteria for subclinical LE included a volume increase ≥3% in the affected upper limb measured by the Perometer compared with the patient's preoperative measurement and, with consideration of the contralateral limb volume changes or bioimpedance spectroscopy (BIS), uses resistance to low-frequency electrical current within the extracellular fluid compartment of limbs in order to determine volume differences.12–15 The goal of timely intervention for breast cancer-related LE is decreased edema, smaller limbs, reduced joint aches, muscle pain and tightness, decreased infection rates, heightened patient desire to continue treatment, decreased medical costs, and improved quality of life.6,13–15
Various methods have been described to measure limb volume after the development of breast cancer-related clinical LE. The standard modality involves tape-measuring limb circumference or water displacement, but both of these can be subject to wide variation as they are operator dependent. Imaging modalities, including MRI, are expensive and inefficient. In the last decade, Cornish et al. has described a new method called “bioimpedance spectroscopy.” 16 BIS provides a measurement of extracellular fluid volume by detecting the response of the body to an applied electrical current. Impedance within tissues is inversely proportional to fluid volume. Advantages of BIS include that it is more objective and more sensitive and specific than conventional methods. Furthermore, this method allows earlier recognition of LE in the subclinical phase, before it comes clinically evident by tape measure or water displacement.
In this study, we aimed to detect the incidence of subclinical LE in patients who underwent ALND and were prospectively monitored by BIS compared to a well-matched control group in which LE was detected only with tape measurements. We then evaluated the importance of monitoring and early intervention of subclinical LE. We hypothesize that the superior ability of BIS to detect subclinical LE will allow intervention when LE is most easily treated and will lead to a decrease in the development of clinical LE.
Materials and Methods
From January 2010 until June 2013, patients with breast cancer were enrolled in the Magee-Womens Hospital Breast Cancer Center LE Education, Monitoring, Early Detection, and Prevention Program prospective database. This project was approved by the University of Pittsburgh institutional review board. Age, BMI, operation type, number of lymph nodes removed, pathologic tumor (T) and node (N) stage, concordance between hand dominance and surgical side, receipt of chemotherapy, radiotherapy (RT), reconstruction, and follow-up time were recorded. In our institute the RT protocol is for patients who had breast conserving surgery done, radiation treatment included whole breast RT with addition of third field to include supraclavicular area and axillary level 3 nodes in patients with node-positive disease. For patients who had mastectomy RT volume included chest wall and with addition of third field to include supraclavicular area and axillary level 3 nodes in patients with node positive disease. IM node was only treated if involved by disease. Dissected level 1 and 2 axilla was only treated with there was gross extra capsular extension or more than 50% of dissected nodes were positive.
For all patients, girth measurements were determined through circumferential assessment using a tape measure at predetermined sites on the involved versus the uninvolved limb. Measurements were taken starting at the tip of the fourth finger and proceeding proximally in 5 cm intervals along the limb for six consecutive points. 9 Clinical LE was defined as girth difference of ≥2.0 cm in the involved limb versus the uninvolved limb. BIS measurement was done using an L-Dex® U400 device (ImpediMed, City, ST) and analyzed as previously described by Cornish et al. 17 Subclinical LE is defined as either L-Dex® values that lie outside the normal range (between −10 and +10 Units) or L-Dex® values that have changed +10 L-Dex® units from baseline may also indicate early LE. L-Dex® was recorded preoperatively, at 3–6 months after surgery, and then annually for 5 years after the operation. The clinical practice pathway is illustrated in Figure 1.
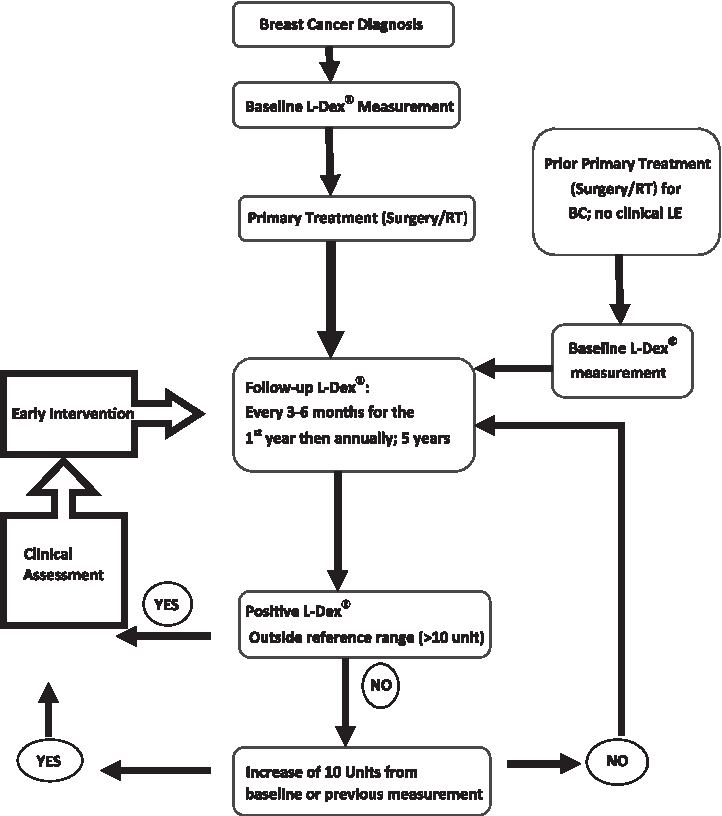
Clinical practice pathways.
Patients were divided into three groups for analysis. The “pre-op group” consisted of newly diagnosed patients with breast cancer whose first BIS reading was performed prior to surgery, and repeated according to the program mentioned earlier. The “no pre-op group” consisted of patients who showed no signs of clinical LE using limb circumference measurements, and whose initial BIS reading was measured within 6 months after the operation. The patients in the “no pre-op group” were then monitored in the LE Program with repeated L-Dex® measurements as above. The “control group” consisted of patients who had preoperative baseline L-Dex® measurements, but due to insurance constraints elected not to participate, had no post-operative BIS measurements, and were instead followed only by circumference measurements.
In order to detect differences in clinical LE in patients who had pre-operative L-Dex® measurements, the incidence of clinical LE in control group was compared with that in the pre-op group. After no clinical differences were identified between the pre-op and no pre-op groups, those that developed subclinical LE were combined into a single group, and progression to clinical LE was compared to the control group.
Statistical analysis was carried out using IBM SPSS Statistics Version 21. Categorical values were analyzed using chi-square test and mean values were analyzed using student's t test. A “p” value less than 0.05 was considered statistically significant.
Results
We enrolled 186 patients who had ALND from January 2010–June 2013 in our prospective database. Six patients were excluded because of death or loss to follow-up (Fig. 2). Of the remaining 180 patients, 116 had a L-Dex® reading prior to surgery. Of these patients, 72 had postoperative BIS measurements, and were classified as “pre-op group,” whereas the remaining 44 patients were followed with tape measurements and formed the “control group.” 64 patients had no preop L-Dex® measurements. Those who had no clinical LE at their first postoperative visit but were diagnosed with subclinical LE at that time were combined together (n=45) with those with subclinical LE in the “pre-op group.” The average follow-up was 19, 19, and 25 months in the “pre-op group,” “control group,” and “no pre-op group,” respectively (p=0.001).
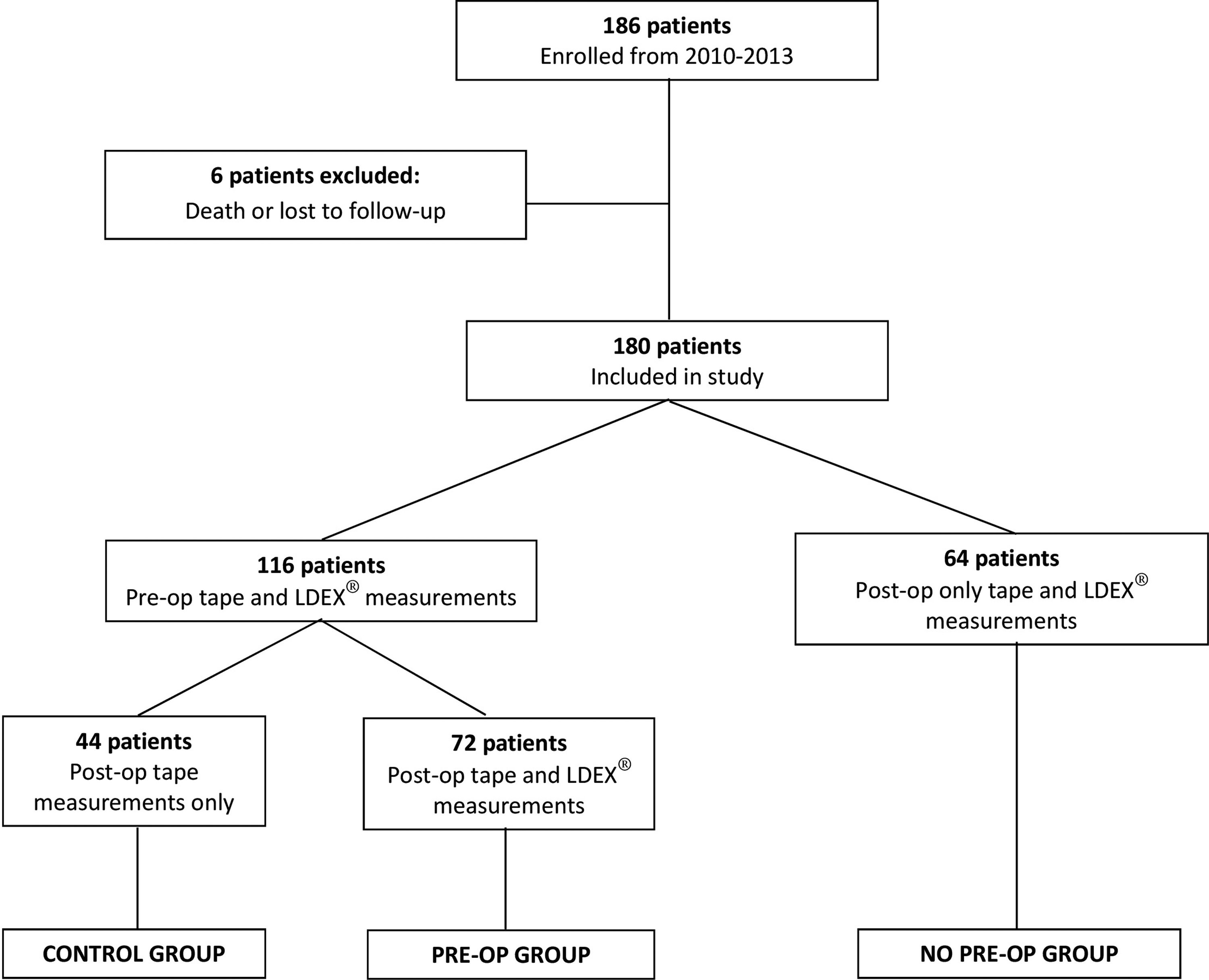
Study patient enrollment and group distribution.
The control group, pre-op group, and no pre-op group were well matched with respect to age, BMI, surgery type, number of lymph nodes removed, pathologic T and N stage, concordance between hand dominance and side of axillary surgery, chemotherapy, radiotherapy, or reconstruction. There was no statistical difference in patient demographics, tumor characteristics, and surgery between patients in the “pre-op group” and the “control group,” all of whom had a pre-surgical BIS measurement, or between patients in the “pre-op group” and the “post-op group,” all of whom had post-surgical BIS monitoring (Tables 1 and 2). The incidence of subclinical LE in the pre-op and the no pre-op groups were 38.9% (n=28) and 26.6% (n=17), respectively (p=0.28) (Table 2). The incidence of subclinical LE in this combined group was 33% (45/136).
BMI, Body Mass Index; LN, lymph node; SD, standard deviation.
BMI, Body Mass Index, LE, lymphedema; LN, lymph node; SD, standard deviation.
In the control group, 13 patients (29.5%) had clinical LE at the 12 month clinical visit and during the subsequent follow up, 3 additional patients (n=16) developed clinical LE. Therefore, the overall incidence of clinical LE was 36.4% in the control group. In the pre-op group (n=72), subclinical LE was diagnosed in 28 patients (38.9%). Two of the patients in the pre-op group progressed to clinical LE (2/72=2.8%) in the average of 19 months follow-up. Clinical LE in the control group was significantly higher compared with the pre-op group (p<0.001) (Table 1).
In order to analyze the progression of subclinical to clinical LE, we combined subclinical LE patients in the pre-op and no pre-op groups (n=45). Only 2 of them (4.4%) progressed to clinical LE in average of 21 months follow-up. Incidence of clinical LE in the control group was 8 times higher than patients diagnosed with subclinical LE who received early intervention (36.4% vs 4.4%; p<0.001) (Table 3).
BMI, Body Mass Index; LN, lymph node; SD, standard deviation.
Discussion
LE is one of the most dreaded complications of ALND, with a reported incidence up to 65%.5–8 There is no curative therapy, and therefore there is a critical need to improve breast cancer related LE risk prediction and prevention.10,11 Detection of LE in the early subclinical phase and timely intervention (education, compression sleeves, physical therapy, and daily exercise, etc.) led to the most successful outcomes in reducing clinical LE incidence. 12 BIS, described in the last decade by Cornish et al., 16 is superior to other techniques for measuring LE, because LE can be detected in the subclinical phase. This method measures the response of the body to an applied electrical current. The goal of our study was to detect the incidence of subclinical LE in patients who had ALND and were prospectively monitored by BIS, compared to patients who were followed only with limb girth measurement. We hypothesized that early detection and intervention afforded by BIS would decrease the development clinical LE. We also aimed to evaluate the importance of monitoring and early intervention of LE by comparing clinical LE incidences between patients followed with BIS and the control group. In our cohort of 180 patients, the incidence of any LE was 61/180 (33.8%), which is consistent with contemporary rates reported in the literature. 18 In the control group of 44 patients who did not receive close BIS monitoring, the incidence of clinical lymphedema was also 36.4%. In contrast, the incidence of clinical LE in patients who had ALND and then were monitored with BIS regularly after the surgery was 2.8% (p<0.001) in a 19 month of a follow-up time. With early recognition and early intervention, subclinical LE progressed to clinical in only 4.4% of these patients in a follow-up of average 21 months. A randomized study with 116 patients showed that early physiotherapy reduces the incidence of LE 18% in 1 year follow-up. 19 In our study with almost a 2 year follow-up with early diagnosis and intervention, the reduction rate of clinical LE was 32%. Although prophylactic intervention could help to prevent and reduce secondary LE in patients after breast cancer surgery involving ALND, it may not be feasible to offer this approach to all patients who undergo ALND. Offering early intervention to the patients who require it is more logical. Our prospective observational study found that one-third women need early intervention and only 4.4% progressed to clinical LE, which is comparable to the incidence in the intervention group of the randomized study of 7%. 19
Mean follow-up times in pre-op, post-op, and control groups were 19 months, 25 months, and 19 months, respectively. Although LE can occur any time after surgery, the majority of LE occurs within 2 years after surgery. 19 Our follow-up time was sufficient to study the incidences of breast cancer-related LE and the importance of early intervention, in order to test the effectiveness of monitoring and early intervention. We plan to follow the patients for at least 5 years.
Using L-Dex® measurement, subclinical LE was diagnosed in 28 patients in the pre-op group (38.9%) and 17 patients in the no pre-op group (26.6%) (p=0.28). BIS measurement is a relatively expensive modality compared to the traditional methods (circumference measurement using tape measure, water displacement etc.), and it is not covered by every insurance company. In this study, 44 patients (25%) of women did not get L-Dex® measurements because their insurance provider denied payment and they elected not to participate by paying out of pocket. During the early subclinical phase of LE, excess extracellular fluid is collected in the dermal or subcutaneous tissue and can easily be treated with cheaper treatment modalities (education, massage, etc.), thereby achieving a better outcome. Our study showed that with a limited intervention, 95.6% of patient diagnosed with subclinical LE by BIS did not progress to clinical LE. During the clinically evident phase, fibrotic tissue pockets are established, requiring more costly treatments (complex decongestive therapy-CDT, intermittent pneumatic compression, etc.) but still with suboptimal outcomes.20,21
Shih et al. studied the health care costs for patients diagnosed with LE after breast cancer surgery and found that total healthcare costs, after removing cancer-specific costs, were nearly $15,000 more in these group of patients requiring LE treatment. 22 Based on the high incidence of clinical LE in the group of patients who were not prospectively monitored and the very low rate of progression from subclinical to clinical LE in the group who were prospectively monitored, our study suggests that BIS monitoring and early intervention could be cost-effective. There is a need to prospectively study cost-effectiveness of BIS monitoring and early intervention for patients with subclinical LE.
LE affects quality of life measurements negatively. According to a recent review, patients with breast cancer-related LE reported a lower health related quality of life score compared to those without LE, due to resulting decrease in physical functioning and psychological and social well-being. 23
Our study was limited by small sample size and lack of randomization. However, groups in this prospective observational study appeared well matched. Also, these results describe outcomes from a single institution. Per our clinical practice pathway, which is illustrated in Figure 1, we plan to follow-up patients both clinically and with L-Dex® for 5 years; therefore, longitudinal information will provide us with the ability to detect subclinical LE and lead to a decrease in the development of clinical LE.
To our knowledge, this is the first prospective study of patients who underwent ALND for breast cancer in which BIS technology was used to detect LE and evaluate the benefits of early diagnosis and treatment interventions objectively. We demonstrated that periodic monitoring of women at high risk for LE, with BIS technology, allowed detection of subclinical LE and timely intervention for treatment, resulting in a reduction of clinical LE from 36.4% to 4.4%. Future studies will determine whether this translates into reduced total health care costs and improved quality of life for patients with breast cancer.
Footnotes
Author Disclosure Statement
No competing financial interests exist.