
Abstract
Abstract
Background:
The lymphatic system is the least studied of the body's systems, and as a result its contribution to human health and diseases is not well known. The failure of the lymphatic system to drain extravasated fluid efficiently leads to accumulation of lymph in the interstitial tissue, thus causing lymphedema. Despite developments in microsurgery procedures, the results of lymphedema treatment remain disappointing. The aim of this study was to develop an experimental animal model that is able to reproduce the disease and to apply various surgical and therapeutic approaches.
Methods and Results:
Lymphedema was induced in New Zealand white rabbits by a total skin denudation and destruction of the lymph channels via microsurgery in the right ear, leaving the left ear as control. Lymphedema generation was observed between days 7 and 15 after intervention. On day 15, a terminal venous lymphatic anastomosis was performed on the posterior edge of the right ear. Serial measurements of ear thickness were made during the study. Ear thickness was significantly (p < 0.05) increased after lymphedema induction compared to baseline (3.2 ± 0.4 vs. 1.3 ± 0.04 mm). After anastomosis, ear thickness was reduced (2 ± 0.26 mm).
Conclusion:
This animal model of lymphedema induction in the ear proved to be a reproducible alternative for studying new approaches to lymphedema treatment and for developing microsurgical skills.
Introduction
T
Lymphedema may be primary or secondary. The secondary form is much more common and is an acquired impairment of the lymphatic system, typically due to infection or trauma or as a complication of medical treatment, especially oncological surgery and radiation. It may also result from damage to lymphatic vessels due to chronic venous insufficiency. 3 Different therapeutic approaches, medical and surgical, such as autologous transplant of lymph nodes, venous lymphatic anastomosis, and other, 2 have been developed for lymphedema management.
Despite recent advances in microsurgery procedures for treatment of lymphedema, the results remain disappointing. 4 Reliable reproducible experimental animal models are needed to replicate the pathophysiology of the condition and thus to allow performance of surgical procedures and therapeutic approaches.
Numerous experimental animal models have been described for recreating chronic lymphedema, but the costs are high and the results are inconsistent. 5
The development of experimental models began with Halsted, a pioneer in the use of radical mastectomy as a treatment for breast cancer.
In 1936, working in a series of dogs, Halsted and Reichert divided all the tissues in the midthigh, with the exception of the femur, the femoral artery and vein, and the sciatic nerve. Normal healing was allowed to ensue. During the first days postsurgery, edema was observed but did not progress toward lymphedema. 6
Drinker and others attempted to reproduce a model by injecting sclerosing substances in the hind leg of dogs, with inconsistent results.
In 1977, Olszewski 7 reported a very encouraging experimental model of lymphedema using the thigh of a dog and concluded that the single section of the lymph channels did not suffice for the formation of lymphedema. He noted that lymph stagnation and chronic, resistant lymphedema could be obtained if, in addition to transection of lymphatics, a circular strip of skin, subcutaneous tissue, fascia, and periosteum were removed from the thigh, leaving a gap for the secondary healing by granulation.7,8 However, this model was very expensive and time-consuming and required very precise surgery.
In an experimental model, Cloudius in 19769 proposed the excision of soft tissue around the dog leg, except for bridges of anterior and posterior skin along the major vessels and nerves. The resulting fibrosis caused lymphedema for about five months. 10
In guinea pigs' ears, Yoon et al. 11 demonstrated that the resection of 2 mm lymphatic trunks does not cause regeneration. However, the most successful method for producing lymphedema and preventing lymphatic regeneration was the resection of 2 cm length of the lymphatic channels. A major conclusion of these studies was that the regeneration of lymph vessels can occur if the defect in the lymphatic channels is small, below 2 mm.
In an attempt to create a simple, reproducible, and lasting chronic lymphedema model, an experimental model in the rabbit ear was proposed.12–16 Eloesser 17 was the first to use the rabbit ear to study edema and lymphatic blockage. In this procedure, a simple incision was made in the back of the ear that caused lymphatic obstruction; however, it was not enough to produce lymphedema. 15
This model presents numerous advantages. For example, it is a fairly homogeneous area of tissue, and drainage is performed through a central venous trunk, which can be accessed by surgery. 18 Another advantage of the rabbit ear model for lymphedema is that it is accurate and easily reproducible and allows sampling for pathophysiological and microscopic studies. 18
Using New Zealand white rabbits, Piller and Clodius9,18 marked the lymph collector vessels with patent blue and removed a 4 cm strip of the skin, subcutaneous tissue, and perichondrium. A band of perichondrium was preserved to cover vessels from drying and wounds were covered with gauze.
With Japanese white rabbits, Huang and Hsin 15 operated on one ear and preserved the other as control. The technique consisted of the removal of a circumferential band of 1 cm of skin, subcutaneous tissue, and perichondrium to 2 cm from the base of the ear; the neurovascular pedicle was protected and the cartilage was preserved. For visualization of the lymphatic channels, 0.5%. methylene blue was injected intradermally into the tip of the ear. This injection allowed visualization of the largest lymphatic channels, about five or seven. Measurements and observations were made on days 3, 7, 15, and 30 postoperatively. Lymphatic dilatation occurred between days 5 and 20 after surgery, while the process of fibrosis began on postoperative day 30. 15
Yoon et al. 11 modified Huang's 15 model by cleaving a 3 cm wide band of skin, subcutaneous tissue, and perichondrium circumferentially from the base of the ear (1 cm), except for the central part of the skin on the back of the ear, leaving a “skin bridge” that was protected under the main neurovascular pedicle. The edges of the skin were sutured inversely to the perichondrium to avoid the approximation of the borders of skin and the rechanneling of lymphatic vessels. This technique resulted in stable lymphedema within 2 months and was effective in rabbits above the age of four years, but younger rabbits do not develop lymphedema. 19
We described an experimental model of secondary lymphedema with young rabbits (12–15 weeks, easily achievable) that develop consistent lymphedema within 2 weeks.
Materials and Methods
In the present study, seven male New Zealand White rabbits weighing 2.5–3 kg were used. The animals were housed in the Animal Research Unit of the Catalan Institute of Cardiovascular Sciences (ICCC) at the Hospital de Sant Pau, Barcelona. The experimental procedures were evaluated and approved by the Institutional Animal Care and Use Committee (CEEA-ICCC) and the Animal Experimentation Commission of the Government of Catalonia (registration number 6645).
Before starting the procedure, the length and thickness of the rabbits' ears were measured. The length of the ear was measured with a ruler placed perpendicular to the skull, placing the ears against each other in parallel. The exact thickness of each ear was measured using a Vernier caliper at 7 cm from the ear tip.
For the induction of lymphedema, the animals were anesthetized with ketamine (1 mg/kg) and medetomidine (1 mg/kg). All animals received a dose of prophylactic antibiotic (Ceftiofur(R) 0.1 mg/kg). Analgesia was controlled with a dose of Metacam (1 mg/kg, i.m.) and local bupivacaine 0.75% s.c. at the base of the ear. At the end of surgery, a single dose of buprenorphine (0.01 mg/kg) was administered to prevent postoperative pain. Animals were controlled daily to detect suffering or pain using a specific pain score.
Two animals (four ears) were used to standardize the technique in a pilot study. We performed a modification of the Huang's 15 technique. The ear was shaved and the external skin was incised all around the ear creating a wound of 1 cm wide at a distance of 2 cm from the base of the ear. Then, the skin was excised making a thorough destruction of lymph channels and blood vessels and preserving the perichondrium to avoid drying of cartilage. Some vessels were destroyed with the scalpel or thermal cautery electrode, while wider vessels needed to be sutured. The external edges of the wound were fixed with 3/0 silk invagination sutures to induce natural healing by second intention (granulation). This technique was performed under microscopy after staining the lymph vessels with Blue Patent V® infiltrated into the subdermal distal portion of the ear.
Animals were left to recover from the anesthesia in their pens. The ears were healed with SSF, iodine, and antibacterial cream and the rabbits wore a recovery collar to prevent them from scratching the ear.
Because measurement of the ear volume to estimate the lymphedema would require anesthetizing the rabbits and could result in a worse welfare condition, it was decided to evaluate lymphedema progression by measuring ear thickness on days 3, 7, and 15 after surgery in awake animals. To standardize the procedure, we observed that thickness increased at these time points and reached a plateau between days 15 and 20 after induction. The animals showed the characteristic clinical presentation of edema in the ear without pain. 4
Animals in the pilot study were observed and ears measured over 30 days after lymphedema induction. There was no significant reduction in the ear thickness (data not shown) with respect to day 15, and there was an increase in tissue fibrosis under skin, which ruled out experimental anastomosis surgery. The veins and lymph vessels were completely immersed in the fibrotic tissue. These observations determined that day 15 after generation of lymphedema was the best moment to perform the surgery.
The remaining rabbits (n = 5) were anesthetized following the protocol and surgery was performed in the right ear to induce lymphedema. The left ear rested as own control in each animal.
After 15 days, the main lymphatic collector was identified by staining the lymph vessels with Blue Patent V; an end-to-end lymphovenous anastomosis (LVA) was then performed (Fig. 1) at the trailing edge of the ear and 2 cm from the circumferential scar at the base of the ear. The LVA was performed using the distal end of the main lymphatic vessel (0.5 mm) and the proximal end of the vein (1.0 mm) with 11/0 nylon. The LVA could not be performed in one rabbit due to complications in the recovery and excess of fibrosis.
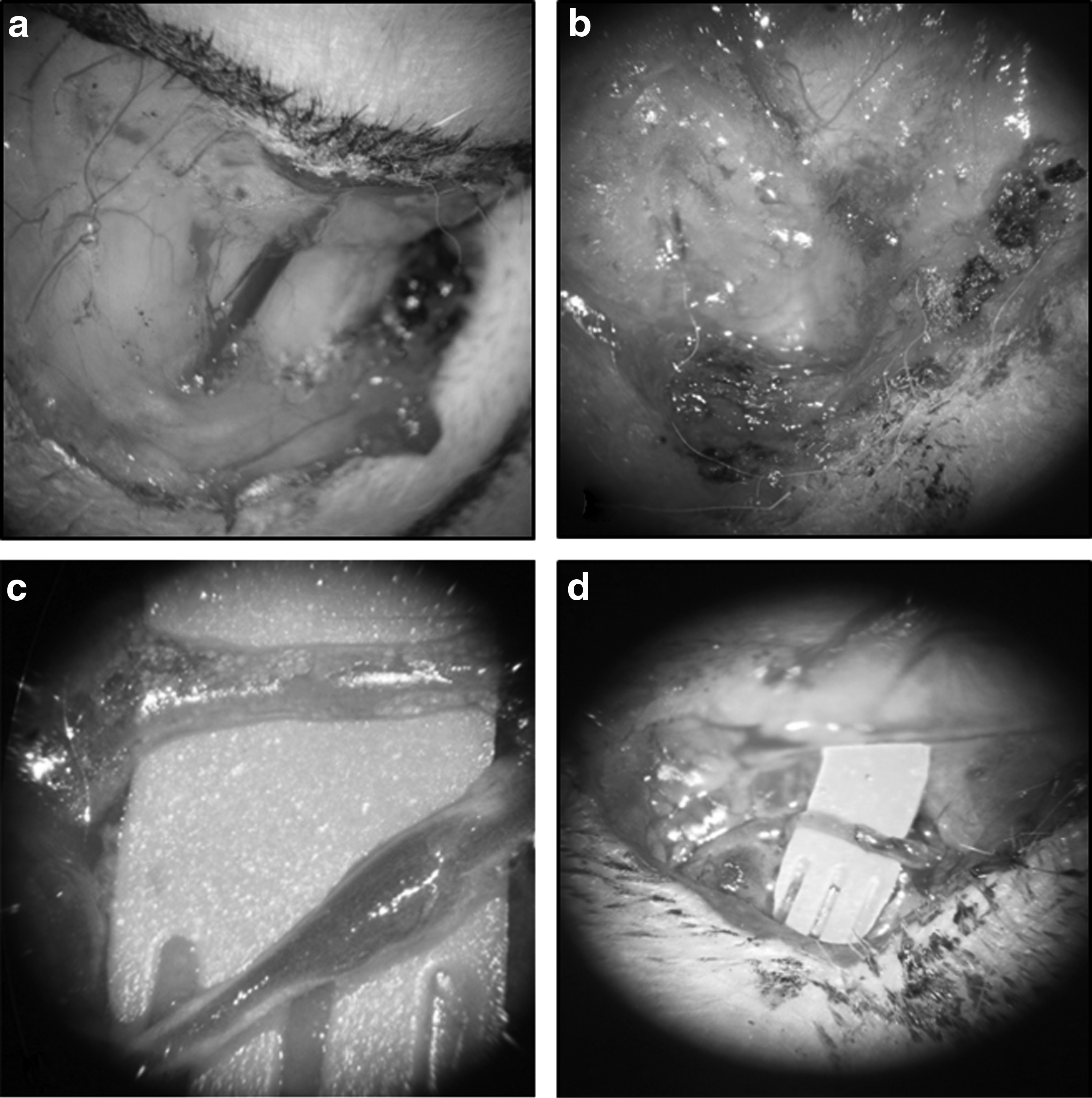
Surgical sequence in the formation of lymphedema.
Measurements were performed on days 3, 7, and 15 after LVA, and animals were euthanized on day 20 postanastomosis (day 35 postintervention).
Samples of tissue (control and treated ears) were obtained at the end of the study. After preserving the tissue with formalin, 6 mm paraffin-embedded serial cuts were performed for conventional staining (hematoxylin/eosin), immunochemistry for detection of lymph vessel wall (anti-LYVE1 antibody; Abcam) (Fig. 2), and histological visualization of interstitial collagen fibers (Picrosirius Red Stain). Images were captured at × 400 magnification with a Nikon eclipse 80i microscope and digitalized by a Retiga-1300i. Staining was calculated by a single blinded observer from an average of six-fields/sample as content (% positive stained area) using ImageJ®.
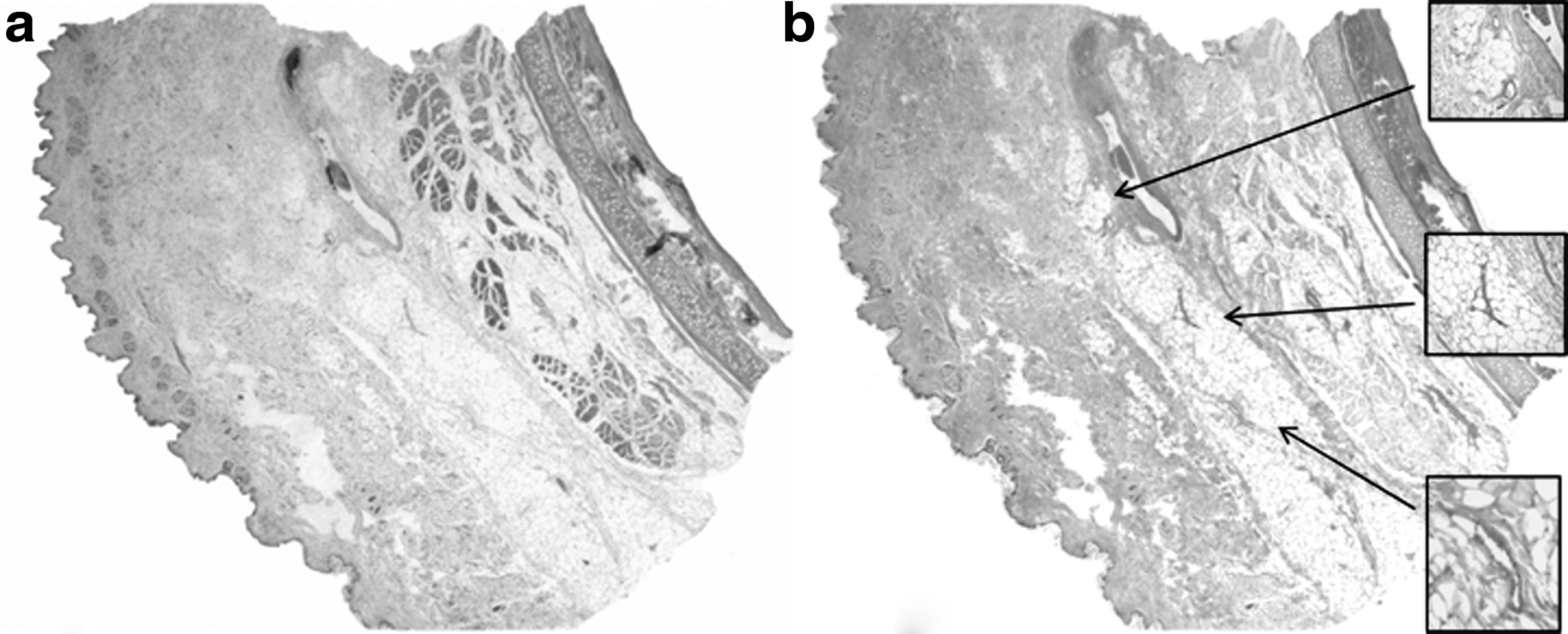
Healthy ear of a rabbit. Histological cross section from skin to inner side. The same cut is stained with
To evaluate the immunological response to the lymphedema, immunohistochemistry 6 μm dewaxed serial sections were incubated with the anti-macrophage mouse monoclonal (ab22506; Abcam) primary antibody according to the ABC method. Target retrieval was necessary. We used 3% hydrogen peroxide to inactivate endogenous peroxidase followed by normal horse serum to reduce nonspecific staining. The sections were incubated for 2 hours. Sections were then incubated with an appropriate biotinylated secondary antibody (1:200; Vector). The chromogen used was 3,3′-diaminobenzidine. Sections were counterstained with hematoxylin.
Statistical analyses
The number of animals to be included in the procedure was calculated using the formula based on serial incidents. 20
Continuous variables are expressed as mean ± SEM. The differences between ear thicknesses were evaluated using a one-way analysis of variance, followed by Scheffe's comparison. A value of p < 0.05 was considered significant. All statistical analyses were performed with the statistical software package StatView.
Results
No differences were observed at baseline between left (control) and right (treated) ear either in thickness (1.35 ± 0.01 vs. 1.34 ± 0.04 mm) or in total length (12.56 ± 0.1 cm).
After induction of lymphedema, the right ear was significantly thicker (p < 0.05) than at baseline. The maximum increase was recorded on day 7 after lymphedema induction (3.2 ± 0.4 mm). The edema then stabilized and day 15 was selected for LVA surgery (Fig. 3). The thickness of the left ear (control) became stabled throughout the study (1.41 ± 0.08 mm).
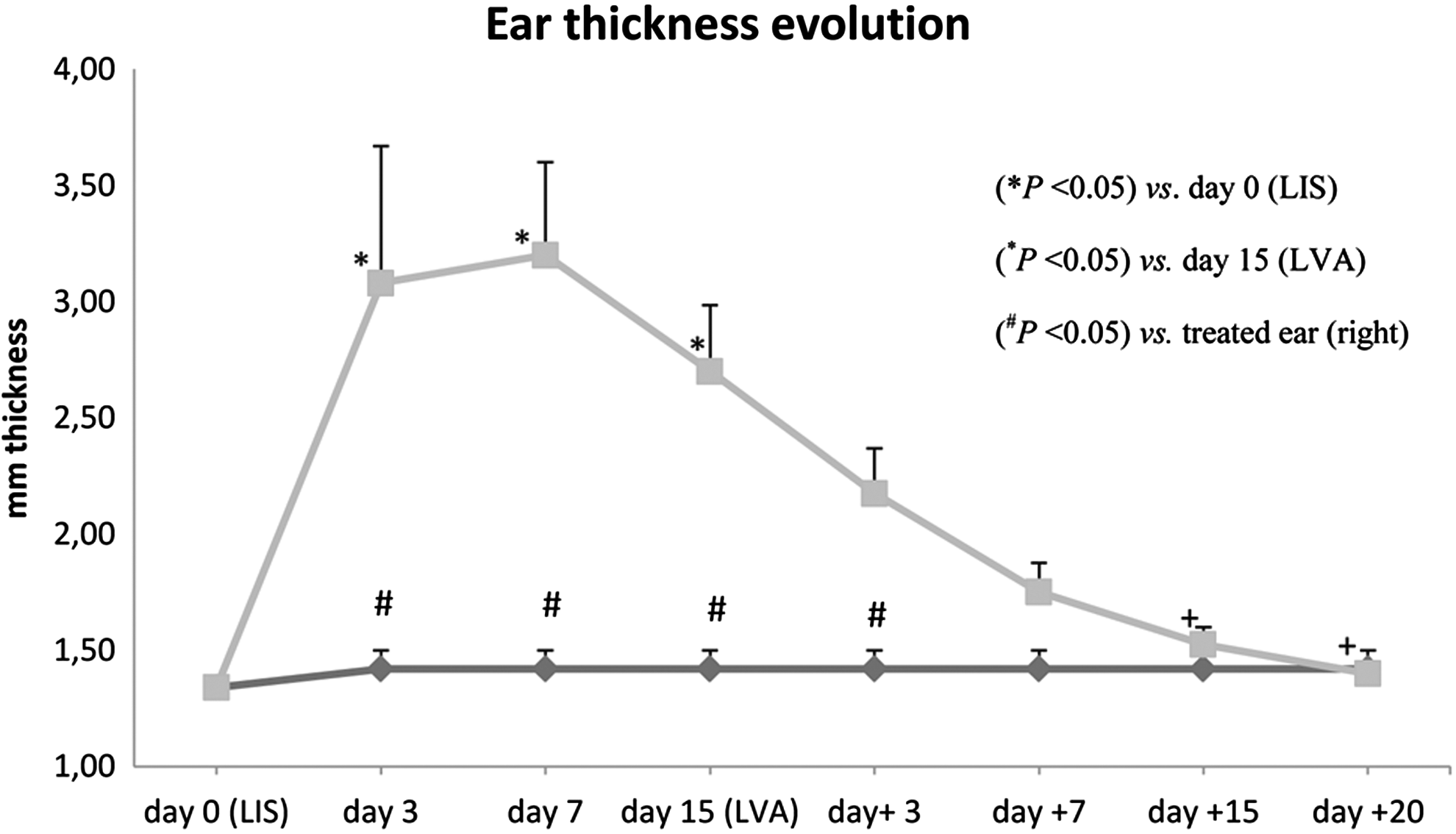
Ear thickness evolution shows the values of right rabbit ear thickness (gray squares) after surgery for the creation of lymphedema (LIS) and after lymphovenous anastomosis (LVA). The significant increase (*p < 0.05) in thickness is evident in the early days. LVA was performed on day 15. Ear thickness decreased progressively, reaching significance (+p < 0.05) on day 15 after the LVA and recovering baseline measures. Measures made in the left control ear (gray diamonds) are also shown (#p < 0.05) compared with injured/treated ear.
After LVA surgery, the ear thickness progressively decreased; the difference reached significance (p < 0.05) at day 15 after surgery (Fig. 3).
The analysis of collagen fibrils by Sirius red staining revealed a dermis with horizontally arranged collagen fibers (Fig. 4). Calculation of the% of positive stained area showed similar results in the different cuts quantified (8.87% ± 1.24%) of the animals at the end of the study.
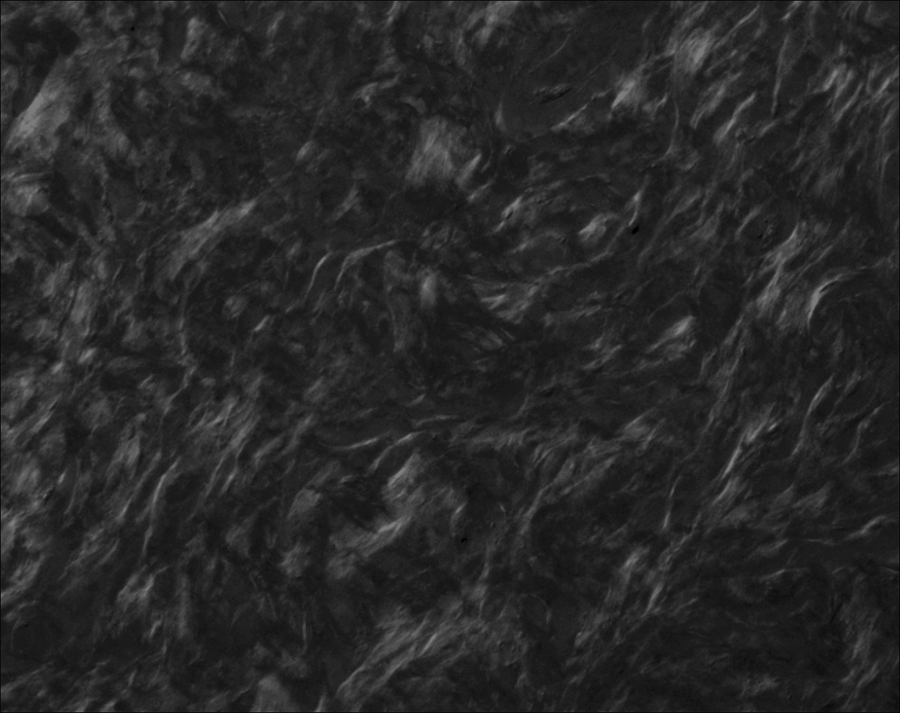
Picrosirius Red stain in sample connective tissue around LVA. Histological visualization of collagen I and III in parallel pattern.
The analysis of histological samples stained to detect inflammation revealed that there were no macrophages in the sample studies (images not shown).
Discussion
This new approach to the generation of lymphedema in rabbits' ears consistently achieved edema formation within a few days. Tissue samples obtained at the end of the study showed fibrosis, poor inflammation, and low infiltration of immune cells. The clinical and histopathological results suggested that the rabbits developed a lymphedema similar to that in humans.
The evolution of lymphedema is faster in rabbits than in humans. By three weeks after induction, the edema is progressively reduced, but the increase in ear thickness is maintained. This is because the condition becomes chronic earlier in young animals than in human adults due to the rabbit's ability to heal 21 ; the accumulation of interstitial and lymphatic fluid inside the skin and subcutaneous tissue stimulates fibroblasts, keratinocytes, and adipocytes leading to the deposition of collagen and glycosaminoglycans inside the skin and subcutaneous tissue, together with skin hypertrophy and the destruction of elastic fibers 12 as seen in the horizontally arranged collagen fibers. In this rabbit model and due to the rapid ability of rabbits to heal, we cannot observe macrophages, what could suggest a process of healing of the induced lymphedema.
A major problem in experimental lymphatic surgery is that no ideal animal model is available. It is difficult to compare results from different animal models with regard to the degree and permanence of the induced lymphedema, because no standardized parameters have been established to date. 2 The experimental data show that the structural changes observed in lymphedema patients, such as fibrosis, infiltration of immune cells, and adipose tissue deposits, should be clearly reproduced in the research environment.20,22
Attempts to reproduce lymphedema in the experimental setting and to reconstruct the lymphatic system have been underway since the 1960s and 1970s.2,16 LVA has been performed by several authors, especially using large animals, but the results have been inconsistent. Both end-to-end and side-to-side LVAs have been performed and experiments involving the use of growth factors (VEGF-C) in association with LVA have been carried out to accelerate the recovery of the lymphatic function. 11 Complications after LVA are reported in up to 38%, 23 although all the animals in our study responded positively to anastomosis.
Rabbit models are widely used in experimental studies, due to the size of the animals and the fact that their general anatomy is well known.24,25 However, the anatomy of their lymphatic system has not been thoroughly elucidated. 26 In the rabbit, the lymph channels are part of the circulatory system, but they are largely independent of the blood vessels; the nodes and conduits are usually considered to be a separate system. 27
Lymphedema studies have focused on the base of the rabbit's tongue and on the animal's upper limbs, although in fact in the upper limbs, there is no evidence of a significant reduction in the condition.28,29
In our model, we performed individual and total destruction of the vessels in the external side of the ear to induce lymphedema, and removed skin and subcutaneous tissue without manipulating the cartilage. We thus achieved consistent lymphedema. Histopathology of control animals showed that lymph vessels are located in the external side of the ear, above the muscle layer and far from the cartilage. No deeper injury in the muscles or in the cartilage was need to be performed, thus allowing animals to recover easily from surgery and avoiding malformation or twisted ear.
The lymph vessels were still dilated on day 20 after LVA surgery. The total destruction of lymph vessels during lymphedema induction inhibited lymph drainage, but the lymph endothelium continued to carry out its function and the accumulation of lymph in the vessels without drainage caused the vessels to dilate. In this experimental study, the animals were maintained no more than 20 days after LVA so we cannot hypothesize whether the dilated lymph vessels return to their baseline size and flow pressure.
The development of this model in the ears of rabbits, animals with a constant lymphatic anatomy that accompanies the principal veins, is likely to be of great benefit for training professionals in microsurgical techniques and may open up new lines of research.
Conclusion
The experimental rabbit lymphedema model described in this study is reproducible and permanent. The model is ideal for surgeons wishing to expand their microsurgical skills to treat lymphedema. The new techniques and surgical skills may improve lymphedema management and would help to optimize patient outcomes.
Footnotes
Acknowledgments
This study was funded by Fondo de Investigación (FIS) en salud del Ministerio de Sanidad y Consumo de España, Instituto Carlos III. Fondo Europeo de Desarrollo Regional (FEDER). Proyecto Numero PI1302793.
We thank Ignasi Gich, PhD, for his statistical and methodological assistance and Dr. J. Oriol Juan-Babot for performing histopathological sections.
Author Disclosure Statement
No competing financial interests exist.