
Abstract
Abstract
Background:
Detection of lymphedema, particularly its mild stage, is clinically challenging. The aim of this study was to determine whether segmental bioimpedance spectroscopy (BIS) provided additional information to whole arm BIS in assessing women with or at risk of lymphedema following breast cancer.
Methods and Results:
Participants (n = 66), aged 61.6 ± 10.5 years (mean ± standard deviation [SD]), were grouped according to lymphedema status: (1)
Conclusion:
Segmental BIS classified as many or more cases of lymphedema than whole arm BIS thresholds without finding lymphedema where it was likely not present while also providing additional information regarding the distribution of lymphedema within the limb.
Introduction
L
Bioimpedance spectroscopy (BIS) is a noninvasive quantitative measure of breast cancer-related lymphedema of the arm,12–14 detecting lymphedema up to 10 months before other assessment methods. 12 During BIS measurement, a small electrical current is passed through the body region of interest and the impedance to the current determined. At low frequencies, this current does not enter the cells, rather passing through the extracellular fluid (ECF). 12 The impedance at low frequency is inversely related to ECF volume, 15 and as lymph is a major component of ECF, 16 BIS is particularly well-suited for detection of the higher levels of ECF found in lymphedema.
Current practice for breast cancer-related lymphedema uses interlimb BIS ratios calculated from the impedance of the arms to determine the likelihood of lymphedema being present. The use of both arms to calculate interlimb ratios removes the effect of weight and whole body fluid changes that are unrelated to lymphedema. To determine whether lymphedema is present, an individual's interlimb ratio is compared to BIS interlimb ratio thresholds previously determined for the dominant and nondominant limb from a normative population.12,17 A BIS ratio that exceeds the BIS threshold is an indication that lymphedema is likely present. BIS ratios can also be monitored over time for progressive increases that are suggestive of lymphedema development, 12 and used to determine treatment effectiveness.18,19
BIS thresholds, traditionally set at three standard deviations (3SDs) above a normative population mean, 12 have been used widely in clinical practice and research.19–22 Its use has been challenged as it may be too high for identification of mild lymphedema. 13 Fu et al. 13 found 34% of women with previously treated lymphedema who still had a 200 mL volume difference between their arms (affected and unaffected) were not detected by 3SD whole arm BIS ratios. Similarly, Dylke et al. 23 found that the 2SD whole arm BIS threshold, rather than the 3SD threshold, had higher sensitivity and specificity for identifying women with mild to moderate lymphatic changes as determined by lymphoscintigraphy. One method, therefore, to improve lymphedema detection could be to use the more liberal 2SD BIS thresholds; however, another method to improve identification of localized or mild lymphedema may be to use segmental rather than whole arm measurements. 11
Previously, we demonstrated that BIS can reliably quantify impedance in smaller segments of the arm and the hand.24,25 Normatively based BIS thresholds for four arm segments and the hand, accounting for limb dominance, in women without history of breast cancer or lymphedema were determined. 24 However, it is unknown whether segmental BIS assessment of the upper limb provides additional information to whole arm interlimb BIS ratios in women thought to be developing or currently living with lymphedema. Segmental BIS of the upper limb could potentially detect mild or localized cases of lymphedema and identify the distribution of lymphedematous changes within the limb. As a consequence, this knowledge may facilitate intervention at a very early stage and allow customization of lymphedema treatment for individual presentations, potentially improving treatment outcomes. The aims of this study, therefore, were to
1. Determine whether classification of lymphedema, based on segmental BIS ratios is in agreement with classification of lymphedema based on the 3SD and the more liberal 2SD whole-arm BIS ratios.
2. Determine whether additional cases of lymphedema are identified using segmental BIS ratios.
3. Describe the pattern of lymphedema distribution at a segmental level.
Materials and Methods
Participants
Sixty-six women who had completed treatment for unilateral breast cancer, including axillary node removal, were recruited through media advertisement and from health services in western New South Wales, Australia. The women were classified according to lymphedema status: (1) at risk for but currently no lymphedema (
Women who were pregnant, had cardiac implants (pacemaker, defibrillator), metal implants in upper limbs, or medical conditions that could impact upper limb fluid volumes (e.g., cerebrovascular accident, limb deformity) were excluded from participating in the study. The participants' characteristics are reported in Table 1. The women in the
Values are mean (SD) by Kruskal–Wallis test.
Values are median (IQR) by Kruskal–Wallis test.
BMI, body mass index; IQR, interquartile range; MCP, metacarpalphalangeal; R:L, right:left; SD, standard deviation.
The BIS ratios for the whole arm in women in the
Ethics approval was obtained from the Human Research Ethics Committee of Catholic Healthcare (Lourdes Hospital and Community Health Service) and the University of Sydney's Human Research Ethics Committee. All participants provided written informed consent.
Assessments
All participants attended an assessment session of ∼30 minutes duration in which all measurements were completed. Height, to the nearest 5 mm and weight, to the nearest 0.1 kg, were measured for calculation of BMI (kg/m2). Whole arm and segmental BIS was used to quantify volume of ECF in the whole arm, hand, and arm segments using an SFB7 impedance spectrometer (Impedimed, Ltd., Brisbane, Australia) following previously described, reliable protocols.24,25,27
In brief, sites for electrode placement were marked with an indelible pen with participants seated, shoulders extended to 90 degrees forward flexion with full elbow extension. After cleaning the sites with an alcohol wipe, electrodes were applied. The measurement electrodes were placed at the metacarpalphalangeal (MCP) joint of the third digit, mid-wrist (dorsum) in line with the ulnar styloid and on the dorsum of the arm at 10, 20, 30, and 40 cm proximal from the ulnar styloid process. The current drive electrodes were placed at the base of the third toe on the right foot, over the third MCP (for whole arm BIS) and the base of the nail bed of the third fingers (for hand and segmental measurements).
Participants were positioned in supine on a nonconductive surface for BIS measurement. The impedances, extrapolated to zero frequency (R0), for the whole arm, hand, and arm segments for both upper limbs were obtained. The measurement electrodes for the whole arm measures were positioned based on the principles of equipotential. 28 In contrast, the measurement electrodes for the hand and segmental measurements spanned the region of interest. The hand and arm segments were defined as follows: hand segment from the third MCP joint to the ulnar styloid, 25 Segment A (Seg A): wrist to 10 cm; Segment B (Seg B): 10–20 cm; Segment C (Seg C): 20–30 cm; and Segment D (Seg D): 30–40 cm.24,27 Calibration of the SFB7 was assessed daily using the test cell supplied by the manufacturer.
BIS files were analyzed using the Bioimp software (version 5.2.4.0). As R0 is inversely proportional to ECF volume, BIS ratios were calculated by dividing the resistance of the unaffected limb/segment by the affected limb/segment (R0unaffected/R0affected) and then compared to thresholds according to limb dominance.12,24
Participants were classified as having lymphedema if their interlimb BIS ratio exceeded previously established thresholds based on normative population.12,24 The different criteria for classification of lymphedema status explored in this study were based on whole arm measurements, including exceeding ≥2SD and ≥3SD above the mean for the whole arm12,23 and on segmental measurements, including one arm segment exceeding ≥3SD above the mean or ≥2 arm segments exceeding ≥2SD above the mean. 24
Statistical analysis
Participant characteristics, absolute impedance and BIS ratio data were checked for normality using the Shapiro–Wilk test. Differences between groups were assessed using analysis of variance and Kruskal–Wallis test. Due to lack of differences, the
Results
For the whole group, whole arm BIS criteria and segmental BIS criteria agreed in classification of the lymphedema status for 78.8% of all participants including 65.9% of those with lymphedema. Neither 3SD whole arm nor the segmental BIS criteria classified women in the
Segmental BIS and the conservative 3SD whole arm BIS criteria were in agreement in the classification of 32 women in the
Adoption of the more liberal 2SD whole arm criteria slightly improved overall agreement between segmental and 2SD whole arm criteria in the classification of lymphedema in the
Segmental BIS detected patterns in lymphedema distribution in the

Individual participant data for women with
Two different lymphedema distribution patterns were identified in the women categorized as having lymphedema by segmental BIS criteria: (1) generalized lymphedema that extended through at least half the limb, that is, at least two adjacent segments (n = 24); and (2) localized lymphedema, in which lymphedema was confined to only small areas of the limb (n = 6). The women who presented with generalized lymphedema met both segmental BIS criteria, that is, one segment exceeded 3SD thresholds and ≥2 segments exceeded 2SD thresholds. In addition, 21 of these 24 women also exceeded the 3SD whole arm threshold, two women exceeded only the 2SD whole arm thresholds and one woman was within 1.2% of the 2SD threshold but had two segments over 2SD and one over 3SD.
The six women with localized lymphedema met only one of the segmental BIS criterion, that is, one segment exceeding 3SD or two segments exceeding 2SD. Four of these six women had a single segment over a 3SD threshold; three were in the
Conclusions
Segmental BIS criteria based on normatively determined thresholds for the hand and 10 cm segments of the arm provided information additional to that provided by whole arm BIS. Segmental BIS thresholds distinguished those with breast cancer-related lymphedema of the arm from those who displayed no signs or symptoms in women with mild to moderate swelling. In addition, segmental BIS quantified the often-uneven distribution 29 of lymphedema within the limb.
Segmental BIS classified more women with lymphedema than the conservative 3SD whole arm BIS criteria. Notably, the additional women classified by only segmental BIS had either localized or mild lymphedema that was unlikely sufficient to exceed the whole arm BIS threshold. The segments that exceeded the segmental criteria were typically in the forearm or around the elbow, with the proximal upper arm and hand least affected. Previous studies have similarly found this pattern, finding that it may be predictive of intractable lymphedema. 29 Furthermore, it is in agreement with current hypothesis of development of lymphedema in which there is localized failure of lymphatics in the mid-arm region. 30
Lowering the whole arm BIS threshold for classification of lymphedema to the 2SD whole arm criteria classified more women as having lymphedema than the 3SD criteria. However, as three women in the
One participant in the
Neither segmental nor the whole arm BIS criteria detected the presence of lymphedema in some women with or suspected of developing lymphedema. The most obvious reasons are that lymphedema was never present, it had resolved or it had reduced to below threshold levels. However, the use of absolute thresholds may be another explanation why some women with lymphedema may not exceed segmental or whole arm BIS criteria for identification of lymphedema. Absolute thresholds, such as those used in BIS, detect lymphedema when BIS ratios meet or exceed thresholds based on a set number of SDs above the mean of a normative population. When women have prebreast cancer surgery BIS ratios below the population mean they must experience an increase in their BIS ratios of more than 3SD to reach the absolute diagnostic thresholds (Fig. 2). Cornish et al. 12 proposed a change of 0.1, from a presurgical baseline, in whole arm BIS ratio as an alternate method of lymphedema detection, with 0.1 being the sum of 3SDs of the mean of a normative population. Thus, women with naturally low presurgery BIS ratios can develop lymphedema before achieving either of the absolute 2SD or 3SD whole arm thresholds. Segmental BIS ratio change values could also be calculated from Svensson et al's data 24 ; however, both whole arm and segmental change values require validation in a longitudinal study.
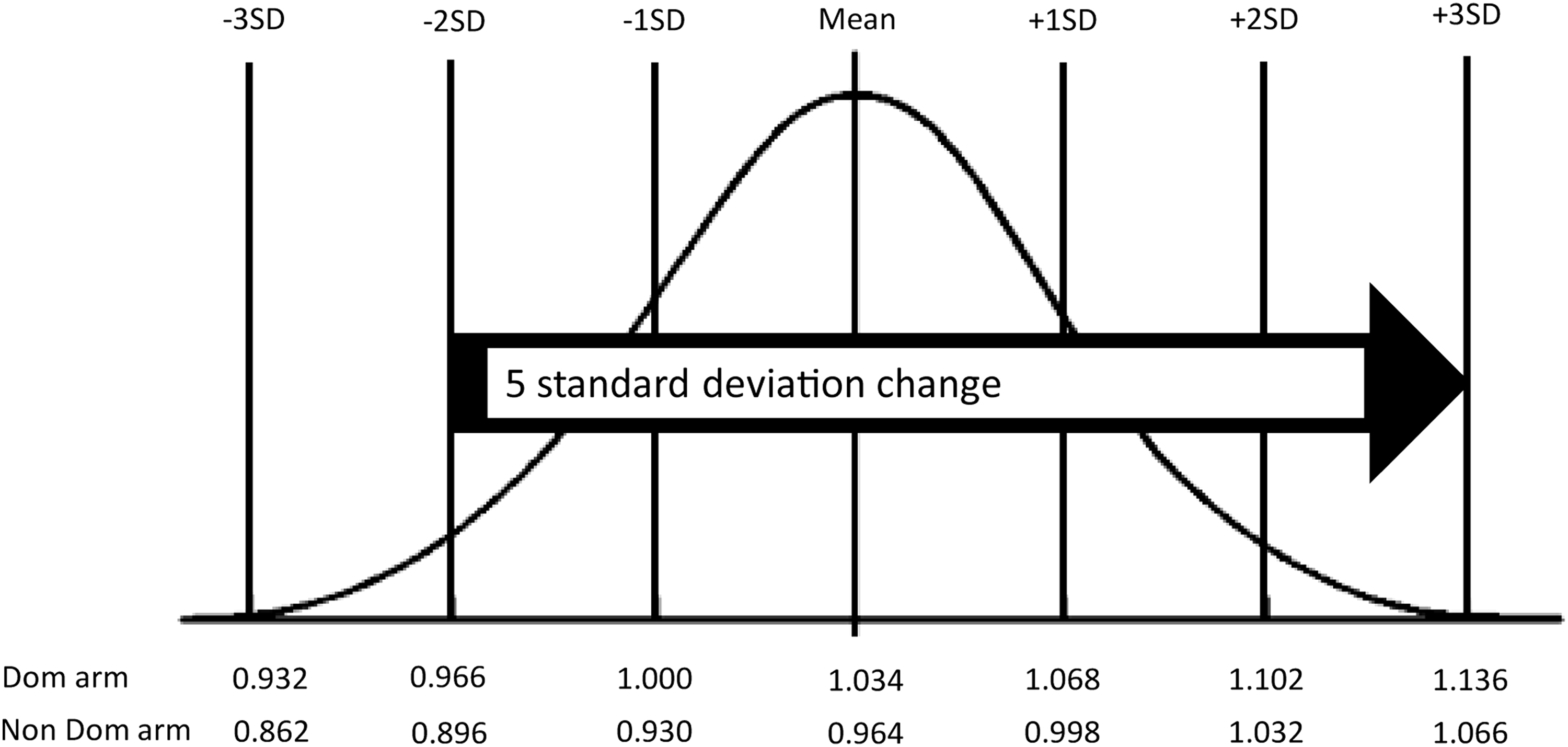
Normal curve distribution diagram. The arrow indicates the number of SDs required to exceed the 3SD absolute threshold from 2SD below the population mean. A woman with a healthy BIS ratio 2SD below the mean may develop lymphedema at 1SD above the population mean, this lymphedema would be detected by BIS ratio change but not absolute BIS thresholds.
Despite the small sample size, this study found that segmental BIS criteria classified additional women to the whole arm BIS criteria in both the
Segmental BIS can supplement whole arm BIS in the detection of lymphedema and evaluation of treatment in women with and at risk of developing breast cancer related lymphedema. There was significant agreement between segmental BIS and whole arm BIS in the classification of lymphedema status; however, segmental BIS identified additional cases of lymphedema without falsely detecting lymphedema in the at-risk population. Segmental BIS provided information regarding the patterns of lymphedema distribution within the limb, including the presence of localized lymphedema in women with newly developing and previously treated lymphedema that was not detectable with whole arm measurements.
Footnotes
Acknowledgment
B.J.S. was supported by project funding from the NSW Health Education and Training Institute (HETI).
Author Disclosure Statement
B.J.S., E.S.D., and S.L.K. have no competing financial interests. L.C. Ward consults to Impedimed, Ltd. Impedimed had no involvement in the design, undertaking, or article preparation of this study.