
Abstract
Abstract
Background:
Lymphoscintigraphy is commonly used to assess breast cancer-related lymphedema. However, a reliable quantitative method that clearly distinguishes normal lymphatic function from lymphedema is desired. We propose a quantitative method based upon the physiological mean transit time (MTT) measure of lymph fluid passing through the arm.
Methods and Results:
Eleven patients, aged 34–68 years, with unilateral arm lymphedema following breast cancer treatment underwent simultaneous bilateral lymphoscintigraphy using intradermal injection of 99mTc-labeled human serum albumin (HSA). Imaging was performed at 30–45 minute intervals for 5 hours. Time activity curves from each injection site and each arm region were recorded. The input into the arm region was obtained as the (minus) time derivative of the injection site activity curve. In the proposed model the arm activity curve was considered to arise from the convolution of the retention function and the input function. The retention function was obtained by fitting the calculated arm activity curve to the measured arm activity curve. The MTT of activity passing through the arm was calculated as the time integral of the resulting retention function. All measured time activity curves were well described by the model. The MTT of the lymphedema arm (mean 60.1 minutes, range 22–105 minutes) was markedly different from that of the contralateral normal arm (mean 5.4 minutes, range 1.2–8.7 minutes), p < 0.0001.
Conclusion:
The proposed model showed great similarity with measured time activity curves and was capable of quantitatively distinguishing lymphatic function of the lymphedema arm from that of the normal arm in terms of calculated MTT.
Introduction
L
Lymphoscintigraphy is an imaging technic of the pathways of the lymph flow and lymph nodes after injection and absorption of a radiopharmaceutical. In patients with unilateral BCRL, lymphoscintigraphy shows asymmetric uptake in the arms and axillary lymph nodes. From tracer distribution the assessment of lymphatic function is qualitatively easy to perform. However, many factors like choice of tracer, injection route, injection site, and patient movement during imaging influence the result of scintigraphy.2,6,7 An ideal tracer for the study of the lymphatic system is one that enters the lymphatic system quickly without any clearance through the microvascular blood circulation. Macromolecules like 99mTc-labeled human immunoglobulin (HIG) and 99mTc-labeled human serum albumin (HSA) exhibit these features. It has been shown that intradermally injected HSA has a fast migration into the lymphatic vessels,8–10 whereas colloidal tracers like 99mTc-labeled Nanocoll reveal a slower removal rate and are less suited for visualizing lymphedema. 2 Previously described quantitative measures of the lymphatic system were based upon the removal rate of the injection depot,7,11–14 time of arrival, or uptake in the axillary lymph nodes.15–17 However, removal rate correlates poorly with lymphedema,11,12 and measurement of uptake in axillary lymph nodes is of limited value in patients having undergone axillary lymphadenectomy.
Lymph transportation through the lymphatic arm vessels has to our knowledge only been quantified sparsely using contrast-enhanced magnetic resonance lymphangiography.
18
Evaluation of potentially new treatments of BCRL would greatly benefit from a truly objective and quantitative measure of the lymphatic function. In the present study, we propose a simple model to describe the activity uptake in the lymphatic arm vessels and fluid. In this model, the activity uptake in the arm is considered a function of the activity draining from the injection depot and the retention of activity within the arm. The mean transit time (MTT) measured in minutes of lymph through the arm is related to the distribution volume (mL) of the lymph and the lymph flow (mL/min) in the arm.
In BCRL the lymph volume is increased and due to axillary lymph node dissection it is expected that to some degree lymph flow is reduced, hence MTT is expected to be longer in the lymphedema arm compared to the normal arm. We will show that from the model data we are able to calculate the MTT of lymphatic fluid through the lymphatic arm system making it possible to quantitatively measure the functional level of the lymphatic system of the arm.
Materials and Methods
Scintigraphy
Eleven women, aged 34–68 years, with unilateral arm lymphedema following breast cancer treatment, including lymphadenectomy, were included after giving informed consent. The study was approved by The Regional Committee on Health Research Ethics of Southern Denmark (S-20150109) and registered at the Danish Data Protection Agency (2008-58-0035). All patients underwent bilateral lymphoscintigraphy using intradermal injection of ∼20 MBq 99mTc-labeled HSA (Vasculocis; CIS Bio International) in 0.1 mL into the interdigital space between the second and third fingers. The subject was placed on the scan bed in supine position with arms slightly bent and hands placed on the stomach. Data acquisition was initiated immediately after injection. Imaging was performed using a dual headed SKYLight (Philips) gamma camera equipped with LEHR collimators, 20% energy windows centered around the 140 keV photo peak of 99mTc. The detectors were positioned in an oblique anterior projection, and care was taken that the entire arm and hand were within the field of view of the detectors. A dynamic acquisition (30 × 1-minute frames) was initially obtained. Hereafter, every 30–45 minutes for the next 5 hours, the patient was put in the same position and imaged for 5 minutes. In between imaging sessions, the patients were allowed to sit or walk around.
Data analysis
Regions of interest were manually drawn around the left and right hand injection depot, and a region around each arm was also drawn. Regarding the arm region, care was taken to include all lymphatic vessels and regions with excess uptake. Two background correction regions were drawn, one above the injection depot and another immediately outside the outer boundaries of the arm region (Fig. 1). Due to slight changes in patient position between imaging sessions the regions were drawn separately on each time frame. All time activity curves were background and decay corrected. The time activity curve of the injection depot has previously been described by a two-phase clearance behavior.
7
Therefore, the measured time activity curve was approximated by a simple function

Scintigraphic images 60 minutes after injection in lymphedema arm and normal arm. ROIs are drawn; red ROIs represent injection depot region and arm region; blue ROIs are background regions of depot region and arm region, respectively. ROIs, regions of interest. A color version of this figure is available in the online article at www.liebertpub.com/lrb.
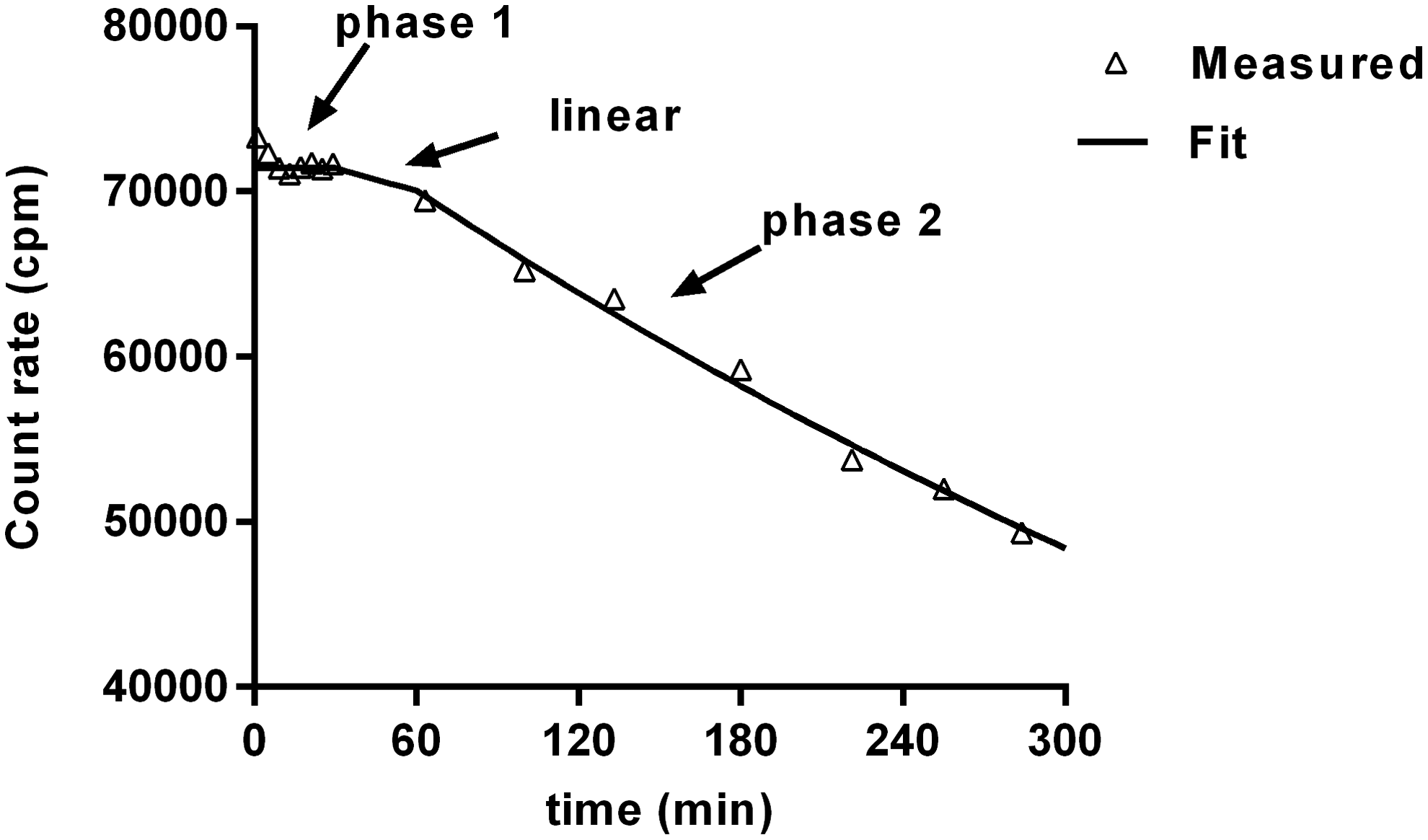
Measured activities and fitted time activity curve from the injection depot in one hand of a patient. The full line represents the fitted curve.
The activity that had cleared from the injection depot was the time derivative (minus) of the injection depot time activity curve
We assumed that all activity leaving the injection depot entered the lymphatic system of the arm region.
Retention function
The lymph was assumed to follow different paths in parallel; some paths exhibited slow transit times, while other parts were fast. In the proposed model we described the retention of lymph fluid as a sum of only two parts: a slow part with long transit time corresponding to the formation of lymphedema; and a fast part corresponding to normal lymphatic function with fast transit through the lymphatic system. The retention of activity in the arm was modeled by the function:
A Fermi function described the slow part that corresponded to long retention of activity in the arm region, and the fast part was chosen to be a Dirac delta (δ) function that corresponded to a very fast transit of activity through the arm region. The dimensionless k parameter [0;1] scaled the amount of activity with slow transit, and the rest (1−k) was the amount with a fast transit. The Fermi function was chosen because by changing only the two parameters α and β a broad spectrum of functions was obtained, ranging from mono exponential functions to square functions. An example of a retention function is illustrated in Figure 3a.The measured arm activity curve
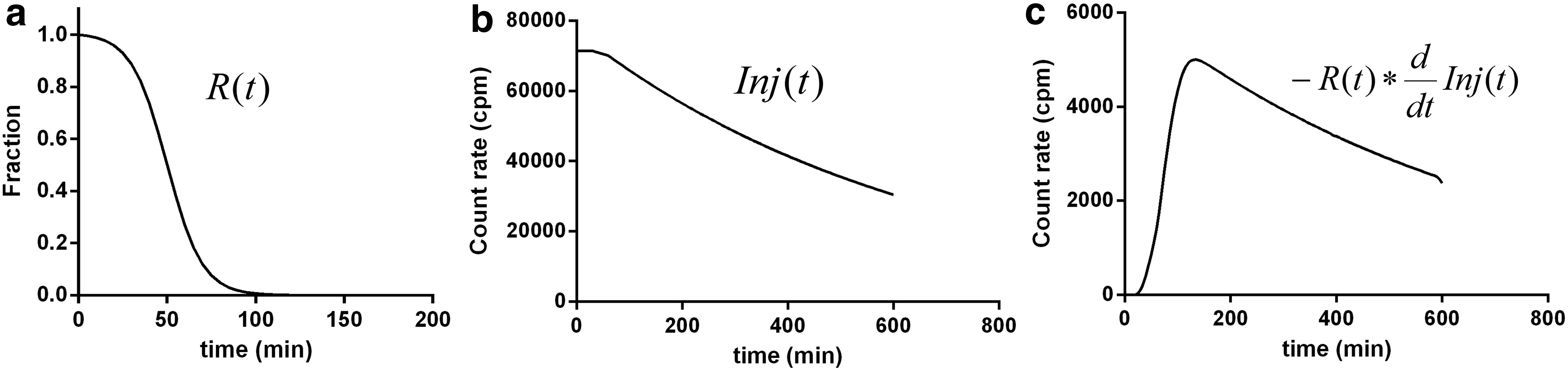
A graphical representation of this equation is shown in Figure 3a–c. The functional state of the lymphatic system was calculated as the MTT of lymph through the arm. MTT was given by the formula:
This integral was difficult to calculate and required knowledge of the entire arm activity curve from acquisition start and until all activity had left the arm. Inserting Equation (4) into the MTT integral (5), we got the following:
This reduces the MTT computation to a much simpler problem of calculating the integral of the retention function
Statistics
Statistical analyses were performed using GraphPad Prism 6 (GraphPad Software, LA Jolla, CA). All parameters are given as mean and range. Comparison between arms was performed using the paired t-test. A two-tailed p-value of p < 0.05 was assumed to be statistically significant.
Results
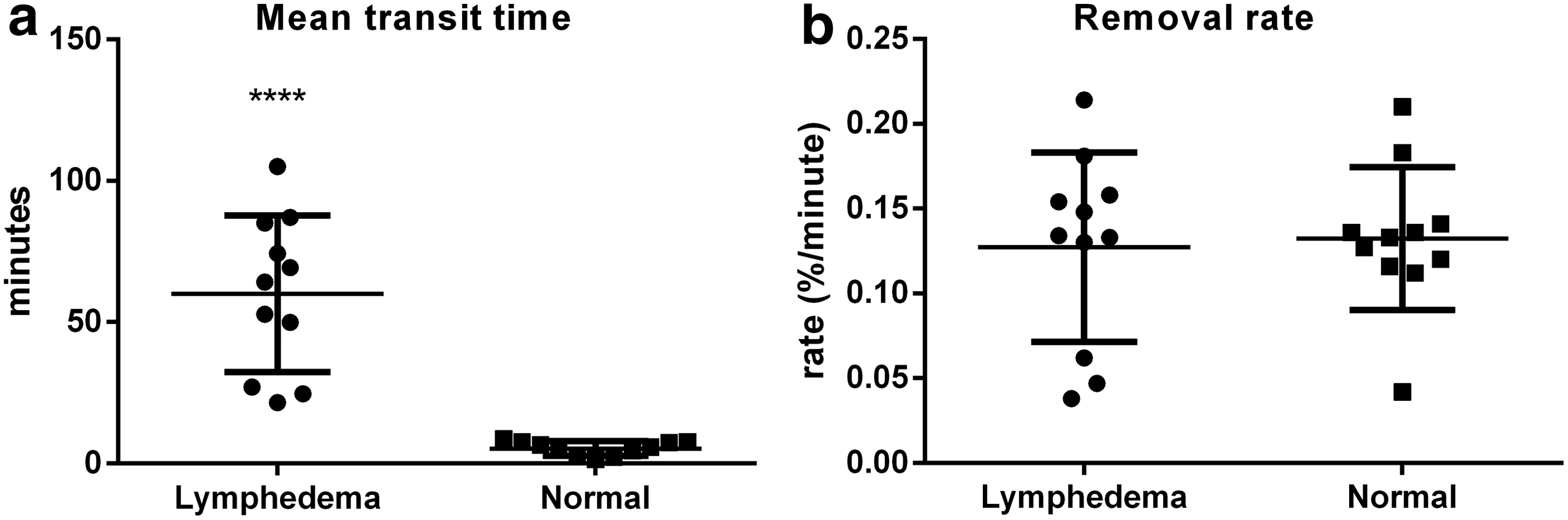
Arm time activity curves for all patients are shown in Figure 4. All cases showed an uptake in the arm region; the uptake was in general delayed for ∼30 to 60 minutes after injection. In five arms, three normal and two edematous, there was a transient uptake within the first 30 minutes; see time activity curves from subject nos. 3, 5, 9, 10, and 11 (Fig. 4). The modeled time activity curves and the directly measured time activity of both normal and lymphedema arms showed a high degree of similarity beyond ∼60 minutes. Mean values and ranges of k, α, and β derived from the best model fit are listed in Table 1. In two patients, nos. 8 and 9, the arm activity curves showed an increasing uptake beyond the acquisition time limit; hence, the α parameter of the retention function was poorly determined. Due to the upper limit of α <300 minutes the calculated MTT was a lower limit of the unknown true MTT in these two subjects. In the entire material, MTT was significantly (p < 0.0001) increased in the lymphedema arm (mean 60 minutes, range 22–105 minutes) compared to the normal arm (mean 5.4 minutes, range 1.2–8.7 minutes) (Fig. 5a). The time activity curve from the injection depot showed dual phase behavior; an example is given in Figure 2. The first phase <30 minutes showed an almost constant lag phase with only little drainage from the injection depot; however in five arms, one lymphedema arm and four normal arms, we saw a rapid activity decline in the first phase (results not shown). In the second phase >60 minutes the activity decline showed an exponential behavior. The removal rate (% min−1) from the injection depot was calculated from data beyond 60 minutes. The removal rate was insignificantly slower in the lymphedema arm (mean 0.127% min−1, range 0.038–0.214% min−1; p = 0.81) compared to the normal arm (mean 0.132% min−1, range 0.042–0.210% min−1) (Fig. 5b).
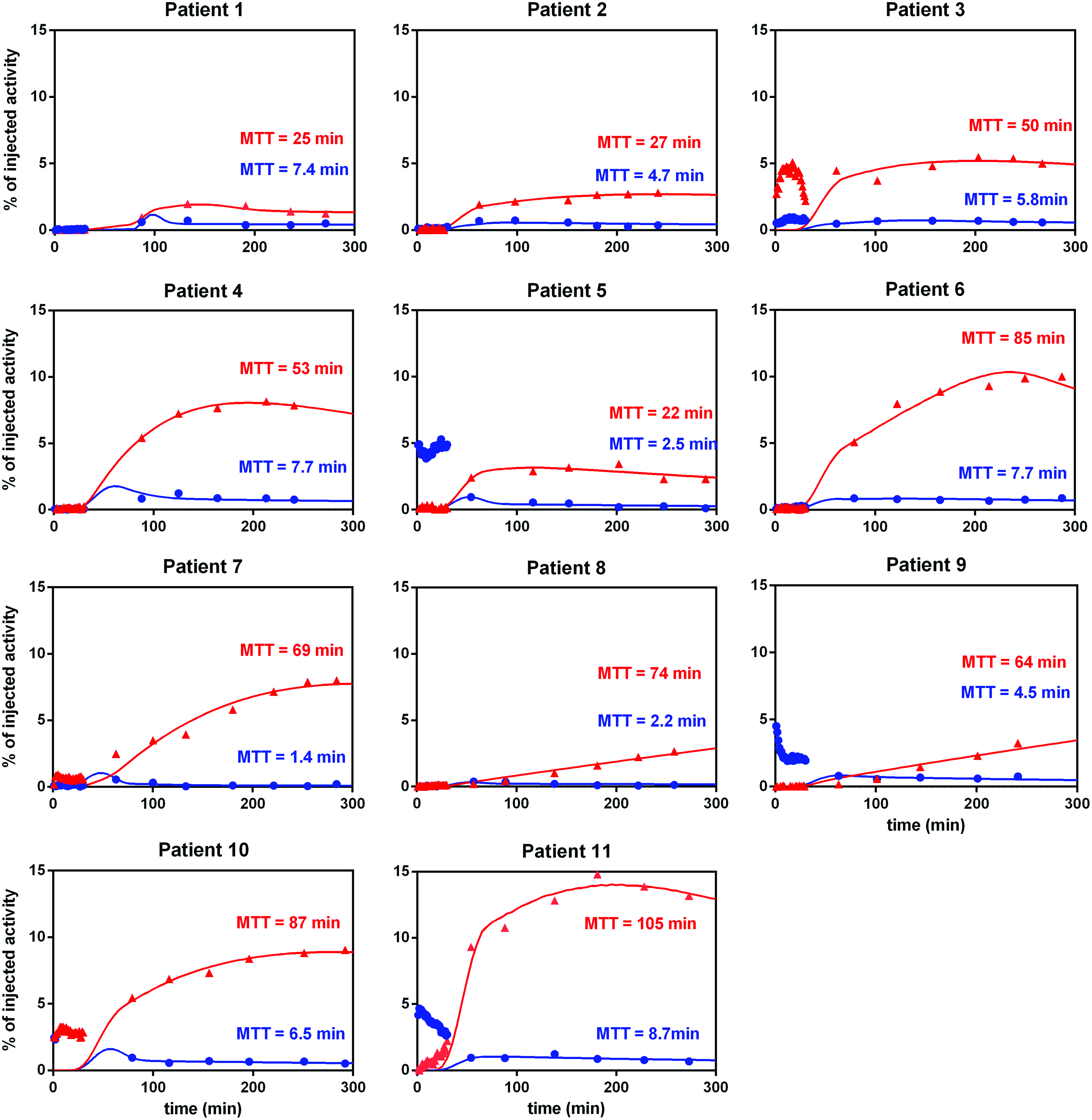
Time activity curves of measured arm activity with fitted model data. Blue (●) represents normal arm activity data; red (▲) represents lymphedema arm activity data. Red curves are model fit of lymphedema arm. Blue curves are model fit of normal arm. MTT, mean transit time. A color version of this figure is available in the online article at www.liebertpub.com/lrb.
Values are given as mean (range).
Discussion
Principal findings
The suggested model showed a significantly longer MTT in all 11 lymphedema arms than in the contralateral normal arms; MTT was on average 15 (3–50) times longer in the lymphedema arm compared to the normal arm. The advantage of the convolution model was the ability to compute the lymphatic response to an individual injection. From a mathematical point of view the lymphatic response was described by a retention function R. If the input activity was injected instantaneously into the lymphatic arm vessels the arm activity curve would simply be given by the retention function. From the derived retention function it was possible to calculate the MTT of lymph through the arm region. This makes the MTT in theory independent of injection route whether this is intradermal, subcutaneous, or subfascial. Moreover, the method is independent of choice of tracer; 99mTc-HIG or even 99mTc-labeled colloidal tracers could be assumed to show similar results. However, tracers with slow removal rates may prove clinically impractical due to the need for very long acquisition times.
Poor lymphatic function of the arm could be expected to yield an increased arm activity. However, such a simple measure of the lymphatic function does not take into account the complex nature of activity accumulation in the arm. In subject nos. 3 and 4 we saw an arm activity uptake of 5% and 8%, respectively, of injected activity at 200 minutes after injection. Thus, subject no. 4 had a 60% higher arm uptake than subject no. 3, but the MTT was only 6% higher. Therefore, the MTT seems to be important in the evaluation of lymphatic function in the individual subject, and in our opinion it is more informative than simple uptake values.
The removal rate from the injection depot was in our study not correlated to lymphedema. Previously, quantitative findings in BCRL have shown significantly lower removal rates from the injection depot in the lymphedema arm than in the normal arm.11,19 However, these findings were based on a different tracer (99mTc-labeled HIG) injected subcutaneously. Other groups did not see any significant difference between removal rates in lymphedema arm and normal arm.12,14 The local removal rate is probably more related to the local lymphatic function around the injection site which only partially reflects the lymphatic system of the entire arm.
In 8 out of 22 arms we saw a transient uptake in the arm within the first 30 minutes after injection. The intradermal injection can be assumed to create a local pressure and a physiological perturbation in the interstitial space that might promote a fast migration of tracer into lymphatic vessels and due to the high pressure the lymph would show a transiently fast clearance through the arm. In the current study we used a syringe with a small dead space between needle and piston. Unintended this small air volume might have partially been injected and caused the transient uptake. In new studies (data not presented here), we changed the syringe to a type without a dead space and this almost entirely solved the issue of transient uptake.
Strengths and weaknesses
The proposed model is very simple and determined by only three parameters. Although simple, the model produced curves that fitted the measured time activity curves to a high degree. The model parameter k was in the range 0.19–0.61 in lymphedema arms, indicating that 19%–61% of the injected activity was transported with a high retention within the arm region, whereas the remaining 39%–81% showed a fast clearance through the arm region. Even though the patients had all undergone axillary lymphadenectomy, some remaining intact lymphatic function must persist and, therefore, to some degree normal transportation through the lymphedema arm was to be expected.
The model is incapable of distinguishing fast transit through lymphatic vessels and clearance through blood vessels; however, the rather slow removal rate of ∼0.13% min−1 in our study compared to previous findings14,20 ranging from 0.12 to 0.31% min−1 and the high fraction of activity retained in the lymphedema arm indicate that clearance directly into blood vessels was a minor issue. A system response is often described as a convolution of a retention function R and an input function I. In many cases the retention function is calculated by direct deconvolution of Equation (4), however, this approach is very sensitive to noise and the solution may vary enormously with only small changes in the dataset. Instead of deconvolution we chose to define the retention function as a sum of two known functions: a Dirac delta function and a Fermi function. By direct calculation of the convolution term in Equation (4) and changing only the three parameters we were able to fit the measured arm activity curve with reasonable accuracy. The Dirac and the Fermi functions were chosen due to their mathematical characteristics and the ability to describe the measured curves with few parameters. The three parameters do not correspond to any obvious physiological parameters; however, the integral of the retention function equals the MTT as shown in Equation (6).
Concern about the labeling stability of 99mTc-HSA has been raised.14,21 Unlabeled 99mTc pertechnetate most likely has a fast clearance from the injection depot; previous studies have shown that subcutaneously injected sodium 131I is cleared from the injection depot with a removal rate of 5.8% min−1 (T½ = 11.8 minutes) 22 ; that is, more than 40 times faster than our intradermal removal rate of ∼0.13% min−1. We used a commercially available HSA Kit and did several tests of the labeling efficiency without finding any unlabeled 99mTc in the used HSA; the labeling efficiency was higher than 99% in all tests. In the proposed model we assumed that within the first 30 minutes after injection the tracer was redistributed throughout the interstitial space and transported toward the lymphatic collectors. Within the first 30 minutes we would expect that more than 80% of any unlabeled 99mTc would clear from the injection depot. Any clearance due to unlabeled 99mTc, the intradermal injection pressure or disrupted lymph vessels were neglected by setting the injection depot curve to a constant within the first 30 minutes.
Meaning of the study
We suggest the described method as a tool to objectively evaluate lymphedema in BCRL and maybe also to evaluate the risk of developing arm lymphedema. Furthermore, the method might prove just as beneficial in diagnosing and evaluation of lymphedema of the lower extremity. Imaging of the lower limbs is a little more challenging due to the large imaging area covering feet to pelvis. We have found that an imaging technique with three consecutive 5-minute planar imaging sessions covering the feet, knees, and upper thighs provides useful data allowing calculation of the MTT of the lower limbs (data not shown)—another new clinical application calling upon further investigations.
Unanswered questions and future research
Imaging protocols involving exercise have shown to increase the removal rate from the injection depot and increase the arm uptake. 12 In our model a high removal rate would result in a high arm uptake; however, to our knowledge it is not known to what degree the lymphatic system in the affected arm responds to exercise. Exercise might promote a relatively shorter MTT in the normal arm compared to MTT in the lymphedema arm and, therefore, promote distinguishing lymphedema and normal arm. Exercise might help shortening the acquisition time and provide knowledge regarding lymphatic flow reserve, a quantity similar to myocardial blood flow reserve measured by myocardial rest–stress perfusion imaging. The MTT is equal to lymph volume divided by lymph flow, and since during rest and exercise volume is constant, any changes in MTT are contributable to changes in flow. The described imaging protocol included an initial 30-minute dynamic acquisition. However, the analyses only used data from beyond 30 minutes, and in hindsight we could have reduced the acquisition protocol to static 5-minute imaging sessions every 30 minutes beginning 30 minutes after injection. Quantitative evaluation of patient with BCRL is of considerable clinical importance especially when new approaches are to be examined. Procedures like lymphovenous shunts, lymph node transplantation, and stem cell transplantation have shown promising results. However, proper selection of patients who will benefit from treatment and quantitation of the therapeutic response is a challenge.23,24 All abovementioned aspects call for future research.
Conclusion
The proposed novel approach was capable of describing the measured time activity curves of the arm regions and provided a quantitative MTT measure of lymphatic fluid through the arm that clearly distinguished the lymphedema arm from the contralateral normal arm in women suffering from BCRL. The method may have promising clinical perspectives, not only with regard to grading the degree of lymphedema but also possibly for evaluating the effect of new treatment measures and perhaps also for preoperative assessment of which patients are most at risk of developing lymphedema postoperatively.
Footnotes
Acknowledgment
The skilled technical assistance of Camilla Bergholdt is gratefully appreciated.
Author Disclosure Statement
No competing financial interests exist.