
Abstract
Abstract
Background:
Histological changes in the collecting lymphatics in patients with lymphedema are classified as Normal type, Ectasis type, Contraction type, and Sclerosis type (NECST) classification. In this study, we investigated the condition of the lymphatic vessels in different sites of the legs.
Patients and Methods:
We prospectively investigated the lymphatic vessels of patients with lymphedema who underwent lymphaticovenous anastomosis (LVA) from August 8, 2014 to August 4, 2015 based on the NECST classification. Lymphedema was diagnosed using lymphoscintigraphy, indocyanine green (ICG) lymphography, and the International Society of Lymphology (ISL) Classification. The affected limbs were divided into four sites: proximal thigh (Site 1), distal thigh (Site 2), proximal crus (Site 3), and distal crus (Site 4).
Results:
A total of 109 patients (205 limbs and 1028 lymphatics) were included in this study. Of the 109 patients, there were 100 women and 9 men with an average age of 61 years. The ratio of Ectasis type vessels increased toward the distal end of the limb with the highest occurrence rate being 54% at Site 4. As ISL stage, ICG stage, and lymphoscintigraphy stage advanced, so too did the ratio of Sclerosis type. In secondary lymphedema patients with lymphedema, the ratio of Ectasis type was more predominant in the distal end of the limb, whereas this tendency was not observed in primary lymphedema patients.
Conclusions:
Sclerotic lymphatics are more predominantly found in the proximal limb whereas nonsclerotic vessels are more often found toward the distal end. These findings help lymphatic surgeon determine incision sites.
Introduction
I
In LVA surgeries, surgeons artificially anastomose lymphatic vessels to nearby veins under a surgical microscope, thereby creating a bypass for the congested lymph fluid to be discharged into the venous system. There already have been several prospective studies that have confirmed the effectiveness of LVA in treating lymphedema;5,6 however, parameters, such as the number of anastomosis per affected limb, the locations at which the anastomosis is made, and the methods of preoperative evaluation, still differ among clinics. For instance, Campisi et al. have reported the effectiveness of inserting and anastomosing adipose tissues containing multiple lymphatic vessels to a single vein 2–3 mm in diameter in areas such as the inguinal and axillary regions proximal to the effected limb.7,8 Seki et al. have reported the effectiveness of single-site LVA at the superior edge of the knee. 9 Koshima et al. have introduced the concept of multisite LVA10–12 and we have reported its effectiveness in treating lower limb lymphedema. 13 It is still controversial which method is superior when threating lymphedema patients.
In our previous report, we have described histological changes in the collecting lymphatic vessels in lymphedema patients and have classified the degree of lymphatic sclerosis into four stages: Normal type, Ectasis type, Contraction type, and Sclerosis type (Fig. 1). We named these stages according to the Normal type, Ectasis type, Contraction type, and Sclerosis type (NECST) classification. 14 In Normal type, the lymphatic vessels are translucent and usually collapse. In Ectasis type, the lymphatic vessels are dilated with an increased inner pressure. In the Contraction type, their appearance becomes cloudy and their walls become thickened. Ultimately, in Sclerosis type, the inner lumen is occluded. Hara et al. investigated the relationship between indocyanine green (ICG) lymphography findings and the NECST classification of lymphatic vessels found in the edematous limb and discovered that the sclerotic changes in the lymphatic vessel wall were more severe in cases where the ICG lymphography findings were more advanced. 15 Additionally, we have previously reported that selecting proper functioning lymphatic vessels, namely Ectasis type lymphatic vessels, is crucial in effectively reducing the circumference of the affected limbs. 13 As these studies have shown, the severity of lymphedema, effectiveness of LVA, and underlying NECST classification of the lymphatic vessels are correlated. 13

NECST classification 14). Staging of lymphedema and the macroscopic anatomical findings in the collecting lymphatic vessels associated with the stages. In normal type, microvascular networks were found to nourish the largely developed walls of the collecting lymphatic vessels. The microvascular networks were gradually lost with the progression of disease stages. In addition, the lymphatic vessel lumen was found to be dilated in Ectasis type, which was associated with an increase in endolymphatic pressure. Because increases in smooth muscle cells and collagen fibers are the major cause of the cloudiness and thickening of the lymphatic vessel wall, they were found to be prominent in the contraction type and the Sclerosis type. NECST, Normal type, Ectasis type, Contraction type, and Sclerosis type; LE, lymphedema. A color version of this figure is available in the online article at www.liebertpub.com/lrb.
In this study, we divided the affected limb into four predefined sites, Site 1–4 (Fig. 2), and investigated the condition of the collective lymphatic vessels identified during the LVA surgery in each site. We believe that the surgical outcome of LVA surgery can be greatly improved by determining the location of Ectasis type lymphatic vessels preoperatively. 13 The purpose of this study was to identify the location of functional lymphatic vessels in lymphedema patients that are most suitable for LVA surgery.
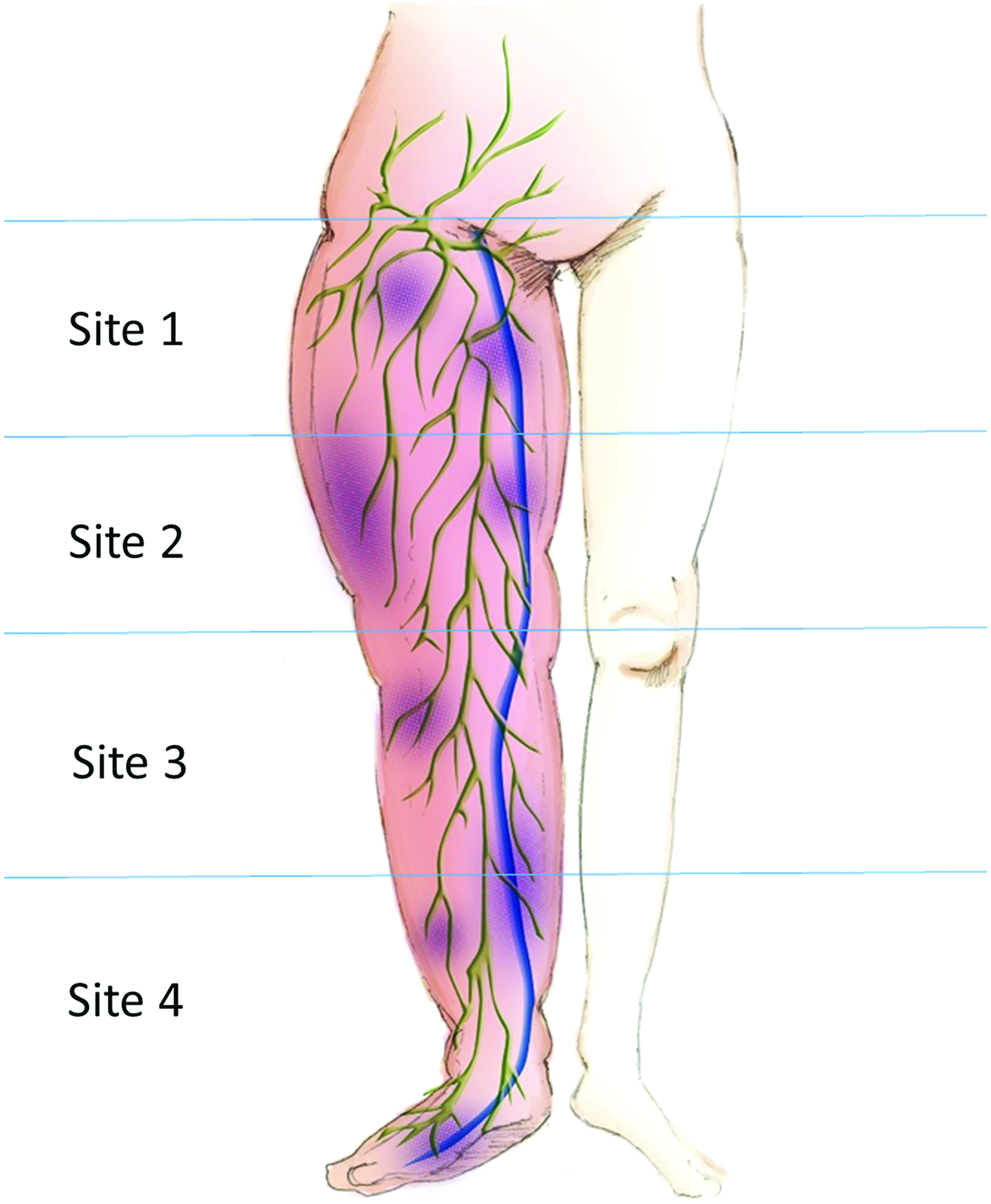
The lower limb was divided into four predefined sites: proximal thigh (Site 1), distal thigh (Site 2), proximal crus (Site 3), and distal crus (Site 4). A color version of this figure is available in the online article at www.liebertpub.com/lrb.
Patient and Methods
We investigated lymphedema patients who underwent LVA surgery during a routine procedure at the Department of Lymphatic and Reconstructive Surgery, Saitama Saiseikai Kawaguchi General Hospital, during the period of August 8, 2014 to August 4, 2015.
Lymphedema was diagnosed using lymphoscintigraphy and ICG lymphography. Lymphoscintigraphy was performed by injecting 0.3 mL (222 MBq) of 99mTc-labeled albumin radioisotope subcutaneously in the first inter-digital space of the foot and radiographs were taken at 15, 30, and 60 minutes after the injection. The results of the lymphoscintigraphy were classified using the Maegawa Classification. 16 ICG lymphography was performed by injecting 0.1 mL of ICG dye (0.5% Diagnogreen; Daiichi Pharmaceutical, Tokyo, Japan) subcutaneously into the first-interdigital space of the foot and observations were made using an infrared camera (Photodynamic Eye; Hamamatsu Photonics, Hamamatsu, Japan) 2 hours after the injection. The results of ICG lymphography were classified using the Yamamoto Classification. 17 Additionally, the severity of lymphedema in each patient was classified using the International Society of Lymphology (ISL) Classification.
LVA surgery was performed according to the methods described in our previous reports.13,18–20 To summarize the steps of LVA surgery, first, the proper mapping of lymphatic vessels and veins was performed preoperatively. Collective lymphatic vessels were identified and marked using imaging techniques, such as lymphoscintigraphy and ICG lymphography. Veins that were suitable for anastomosis were identified using the Non-contact Vein Visualizing System (AccuVein, Cold Spring Harbor, NY). Skin incision lines were designed at sites where the identified lymphatic vessels and veins approached each other. In areas where lymphoscintigraphy and ICG lymphography could not identify any lymphatic vessels, ultrasonography was performed at the medial region of the lower limb close to the great saphenous vein. Skin incisions were then made at areas where suitable subcutaneous veins with diameters of 0.5–1 mm were identified.
Three dividing lines, at the center of the thigh, center of the patella, and center of the crus, were first defined for each edematous limb. The limbs were then further subdivided into four predefined sites: proximal thigh (Site 1), distal thigh (Site 2), proximal crus (Site 3), and distal crus (Site 4) (Fig. 2). Lymphatic vessels found in each of these sites were classified based on the intraoperative findings, according to the NECST classification. The findings of the NECST classification were compared with the ISL and ICG lymphography staging.
This prospective study was approved by the Clinical Ethics Committee in Saitama Saiseikai Kawaguchi General Hospital (UMIN000014748). Proper informed consent was obtained from all patients who were involved in this study.
Results
Of the lymphedema patients who underwent LVA surgery at Saitama Saiseikai Kawaguchi General Hospital during the study period, a total of 109 patients and 205 lower limbs were selected as candidates for this study (Table 1). Among these subjects, 17 patients had a past history of allergic reaction to the contrast agent used in computed tomography (iodine system); therefore, ICG lymphography was performed in the remaining 92 patients only. Of the 109 patients, there were 100 female and 9 male subjects with an average age of 61 years (range: 31–86 years). The etiology of the subjects included 44 cases of cervical cancer, 27 cases of uterine cancer, 18 cases of ovarian cancer, 14 cases of malignancy of other origins, and 14 cases of primary lymphedema. Eight of the patients had multiple primary neoplasms. Ninety-one cases underwent lymphadenectomy following cancer surgery and 19 cases received postoperative radiation therapy. The average disease duration was 79.8 months (5–360 months) and 37 cases developed cellulitis during their clinical course. A total of 1028 LVAs were made and the average number of anastomosis per limb was 5.0. Among the lymphatic vessels used in these anastomoses, 34 were Normal type, 438 were Ectasis type, 414 were Contraction type, and 142 were Sclerosis type vessels.
ISL, International Society of Lymphology.
Figure 3 shows the NECST distribution of the lymphatic vessels found in each site. The ratio of Ectasis type vessels increased toward the distal end of the limb with a highest occurrence rate of 54% at Site 4. Conversely, the ratio of Contraction type and Sclerosis type lymphatic vessels increased toward the proximal end of the limb with the highest occurrence rate being 64.5% at Site 1.
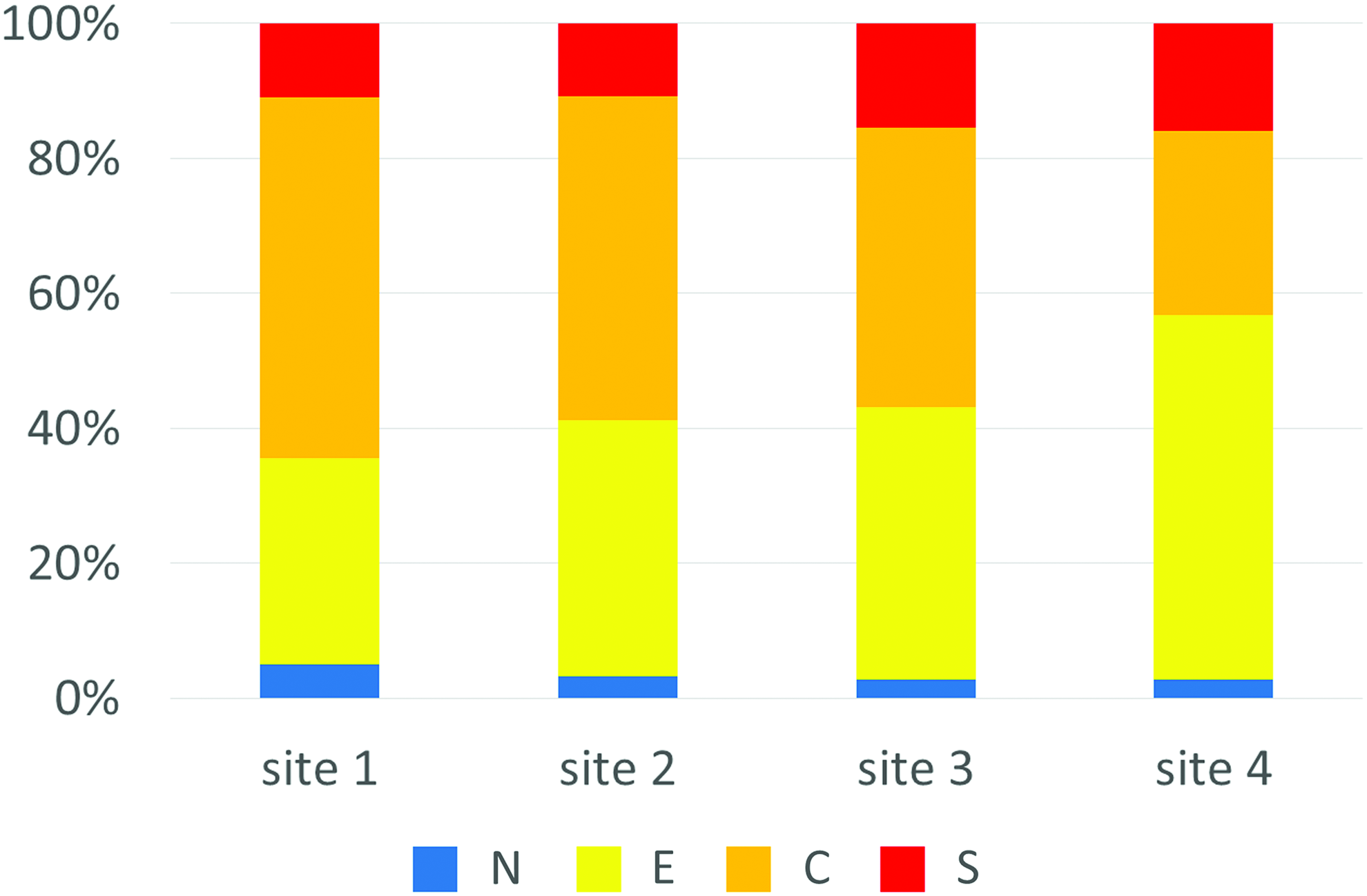
Distribution of the NECST vessel types found in each of the four sites. Ectasis type vessels were found more frequently toward the distal end of the limb. Contraction and Sclerosis type vessels were found more frequently toward the proximal end of the limb. A color version of this figure is available in the online article at www.liebertpub.com/lrb.
NECST distribution and ISL stage
The ratio of each of the NECST vessel types found among the four sites in each ISL stages was investigated (Fig. 4). For patients in ISL stage 1 and 2, the ratio of Ectasis type vessels was more predominant at the distal end of the limb, whereas that of Contraction type vessels was more predominant at the proximal end. There was no significant difference in the ratio of Sclerosis type vessels among each site. No significant difference in the distribution of each NECST type vessels were found in Stage 3 patients.
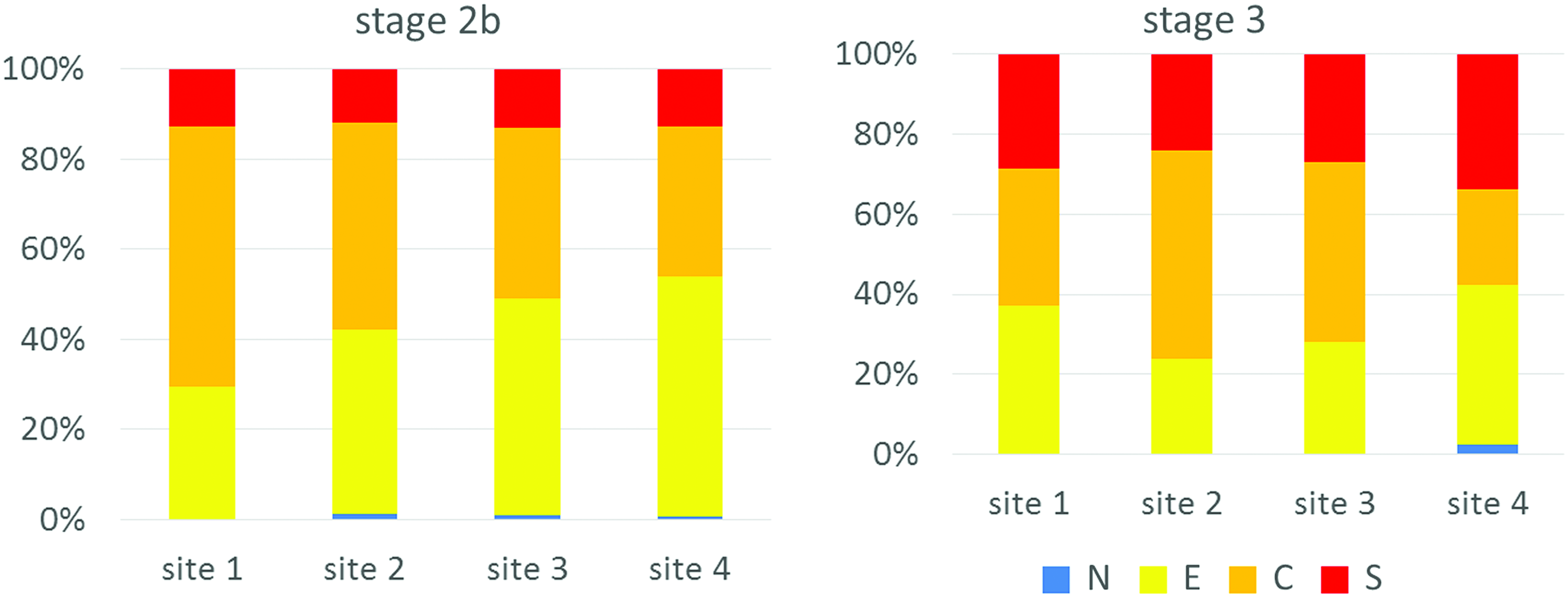
The ratio of each of the NECST vessel types found among the four sites in each of the ISL stages. For patients in Stages 1 and 2, Ectasis type vessels were found more frequently in the distal end whereas Contraction type vessels were found more frequently in the proximal end of the limb. There was no significant difference in the distribution of Sclerosis type vessels among the four sites. Furthermore, there were no significant differences in the distribution pattern of each vessel types in ISL Stage 3 patients. ISL, International Society of Lymphology. A color version of this figure is available in the online article at www.liebertpub.com/lrb.
NECST distribution and lymphoscintigraphy stage
The ratio of each NECST vessel types found among the four sites in each lymphoscintigraphy stages was investigated (Fig. 5). For patients who were in lymphoscintigraphy stages 1–4, the ratio of Ectasis type vessels were more predominant in the distal end of the limb, whereas the ratio of Contraction and Sclerosis type vessels were more predominant in the proximal end. The ratio of Ectasis type vessels was high in Sites 1 and 4 and low in Sites 2 and 3. Moreover, the ratio of Sclerosis type vessels was more predominant in the distal end of the limb in comparison with the other stages.
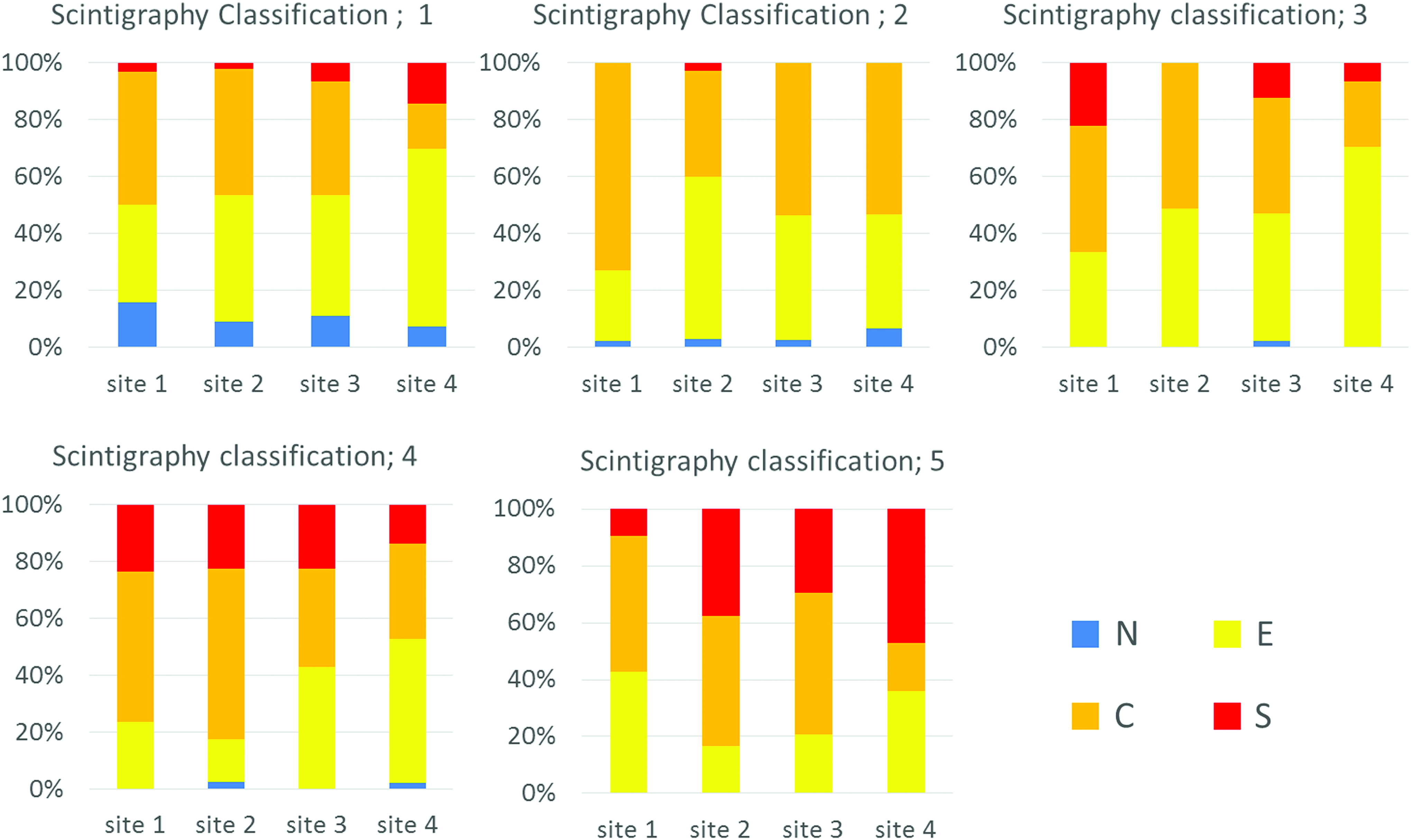
The ratio of each NECST vessel types found among the four sites in each lymphoscintigraphy stages. For patients in Stages 1 through 4, Ectasis type vessels were found more frequently toward the distal end whereas Contraction and Sclerosis type vessels were found more frequently toward the proximal end of the limb. For Stage 5 patients, the ratio of Ectasis type vessels was high at Sites 1 and 4 and low at Sites 2 and 3. The ratio of Sclerosis type vessels was higher toward the distal end of the limb in Stage 5 patients. A color version of this figure is available in the online article at www.liebertpub.com/lrb.
NECST distribution and ICG lymphography stage
The ratio of each NECST vessel types found among the four sites in each of the ICG stages were compared (Fig. 6). The ratio of Ectasis type vessels was more predominant in the distal end and less so in the proximal end of the limb in all ICG stages. For patients in ICG Stages 4 and 5, the ratio of Sclerosis type vessels was more predominant in the distal end of the limb compared to the proximal end. Moreover, sclerotic changes to the lymphatic vessels were observed in Stage 0 patients in the proximal end of the limb.

The ratio of each of the NECST vessel types found among the four sites in each ICG stages. The ratio of Ectasis type vessels was greater in the distal end and less so in the proximal end of the limb in all ICG stages. For patients in ICG Stages 4 and 5, the ratio of Sclerosis type vessels was greater in the distal end of the limb. Sclerotic changes in the lymphatic vessel wall were also observed in Stage 0 patients in the proximal end of the limb. ICG, indocyanine green. A color version of this figure is available in the online article at www.liebertpub.com/lrb.
Secondary lymphedema and primary lymphedema
The distribution of each of the NECST vessel types among the four sites in secondary lymphedema patients after cancer surgery was compared with the distribution of NECST vessel types in primary lymphedema patients (Fig. 7). In secondary lymphedema patients, the ratio of Ectasis type vessels was more predominant in the distal end of the limb, whereas that of Contraction type vessels was more predominant in the proximal end. In primary lymphedema patients, Ectasis type vessels were more predominant in the crus compared to the thigh region, with the highest ratio being in Site 3. The pattern of NECST vessels type along the proximal to the distal end of the limb that was observed in secondary lymphedema patients was not observed in primary patients. A Sclerosis type vessel was not found in the thigh region of primary patients.
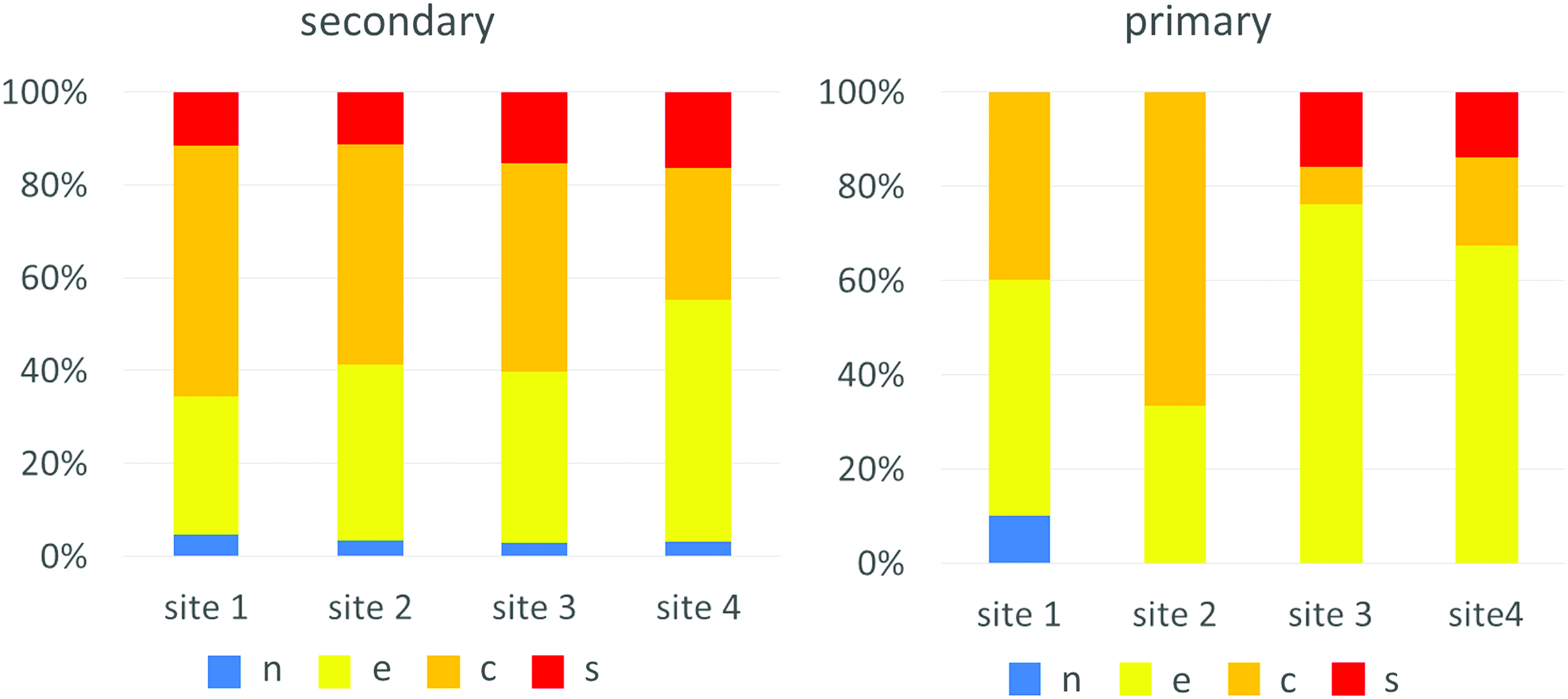
The distribution of each of the NECST vessel types among the four sites in primary and secondary lymphedema patients. In secondary lymphedema patients, Ectasis type vessels were found more frequently in the distal end, whereas Contraction type vessels were found more frequently in the proximal end of the limb. In primary lymphedema patients, Ectasis type vessels were found more frequently in the crus compared to the thigh region, with the highest ratio being in Site 3. Sclerosis type vessels were not found in the thigh region of primary patients. A color version of this figure is available in the online article at www.liebertpub.com/lrb.
Discussion
In this prospective study, we classified lymphatic vessels found during LVA surgery according to the NECST classification 14 and investigated the distribution of each vessel type in different sites in the edematous limbs of lymphedema patients. The degree of lymphatic vessel sclerosis was milder toward the distal end of the limb and vessels found in those areas were better suited for the LVA procedure. However, such distribution pattern could be reversed depending on the severity of the disease. This is a pioneering study that investigated the condition of the collective lymphatic vessels in each of the predefined sites in the lower limbs of lymphedema patients.
There have been many previously reported operative techniques of LVA.7–13 It is still controversial as to whether single-site or multisite LVA yields a better surgical outcome. From our current study, we were able to conclude that sclerotic lymphatic vessels are more often found at the proximal end of the affected limb; hence, performing LVA at the proximal end may not yield optimal results. Moreover, we were also able to show that there is no guarantee that lymphatic vessels with conditions suited for LVA can be found in the distal thigh area (Site 2). These findings indicate that performing LVA in one fixed site may not be suitable for all of the lymphedema patients and each patient may have his or her own best site for LVA. Therefore, it is necessary to readjust and select the most optimal site for LVA depending on the severity of the lymphedema and the preoperative lymphatic mapping images. Additionally, since it has been reported that anastomosis made during LVA surgery may become occluded as time passes,21,22 performing LVA at multiple sites with multiple anastomoses could result in a better surgical outcome.
When analyzing the results by ISL classification, there was no significant difference between the distributions of the NECST classification of the vessels found in ISL Stage 3 patients. Equal frequencies of Contraction and Sclerosis type vessels were found in the distal end of the affected limb in these patients. Although lymphatic vessel sclerosis was more predominant toward the distal end of the affected limb in patients who were classified as ISL stages 1 and 2, the sclerotic change of the lymphatic vessels might have already advanced toward the distal end of the limb for patients who are in Stage 3. This is supported by the fact that the ratio of Sclerosis type vessels was more pre-dominant in Stage 3 patients when compared with the other stages. Therefore, locating suitable vessels for LVA by thorough preoperative evaluation of lymphatic function and proper lymphatic mapping is imperative in achieve a better surgical outcome in Stage 3 patients.
When analyzing the results by lymphoscintigraphy classification, Contraction and Sclerosis type vessels were more predominant toward the proximal end of the affected limb in patients who were classified as lymphoscintigraphy stages 1 through 4. Thus, sclerosis of lymphatic vessels advances from the proximal to the distal end of the limb. However, Sclerosis type vessels were more predominant in the distal end of the limb in Stage 5 patients. Furthermore, the degree of lymphatic vessel sclerosis was more severe. Lymphoscintigraphy involves the subcutaneous injection of a radioisotope at the interdigital space of the foot. Therefore, it would be difficult to properly map and evaluate the lymphatic function of Stage 5 patients who have more advanced vessel sclerosis in the distal end of the limb. However, the proximal lymphatic vessels might still be functional and suitable for LVA in these patients. Hence, additional evaluations using other imagining techniques, such as ICG lymphography, is necessary to properly evaluate and locate the most optimal site for LVA in Stage 5 patients.
When analyzing the results by ICG lymphography classification, Sclerosis type vessels were more predominant in the distal end of the limb in ICG Stages 4 and 5 patients. Although linear patterns represent normal lymphatic flow in ICG lymphography, collateral lymphatic vessels are often observed in lymphoscintigraphy Stage 1 patients, thereby suggesting abnormal lymphatic function. Furthermore, even when a linear pattern is observed, only 7.3% of the lymphatic vessels found in these areas are of the Normal type, whereas the other vessels were either dilated or sclerotic.
Ectasis type vessels were more predominant in the distal end, whereas Contraction type vessels were more predominant in the proximal end of the limb in patients with secondary lymphedema. This implies that lymphatic vessel damage advanced from the proximal toward the distal end of the limb. This result supports the pathophysiology of secondary lymphedema as the edema originates from the proximal end and advances toward the distal end of the limb. Meanwhile, such distribution pattern of lymphatic vessels was not observed in primary lymphedema patients. For primary lymphedema patients, Ectasis type vessels were more predominant in the crus compared to the thigh area, whereas Sclerosis type vessels were found only in the crus area. As previously reported, the condition of the lymphatic vessels in primary lymphedema may vary among patients. 23 Therefore, it is important to preoperatively evaluate the lymphatic function of each patient before LVA or lymph node transfer surgeries.24,25 Through preoperative examinations, we can estimate the percentage that there is a good lymphatic vessel for each site based on the lymphoscintigraphic or ICG lymphographic staging, and we can increase the possibility that we can find it intraoperatively.
In this study, only the number of lymphatic vessels actually used in the anastomosis was recorded, despite multiple vessels having been found in a single skin incision site. Although lymphatic vessels of different NECST types may often be found in a single incision site, we did not record the vessels that were not used for anastomosis. For this reason, since the most optimal vessel was selected for LVA, the number of Ectasis type vessels may have been recorded more often when compared with the other types. The limitation of this study is that we did not assess all lymphatic vessels in the entire affected lymphedematous limb. Future studies should evaluate the condition of the lymphatic vessels in the entire limb, which could lead to a better surgical outcome for lymphedema patients.
In conclusion, sclerotic lymphatic vessels are more predominantly found in the proximal end of the limb in lymphedema patients, whereas non-sclerotic and dilated vessels are more often found toward the distal end. Conversely, Sclerosis type vessels are more predominantly found toward the distal end of the limb in advanced lymphedema patients who are classified as lymphoscintigraphy Stage 5 or ICG lymphography Stage 4 and 5. These results may help lymphatic surgeons determine the most optimal location to make an incision for the LVA surgery.10–13
In this study, it is clarified that the lymphatic vessels of Ectasis type are easily found in the distal side of the extremities. On the other hand, establishing LVA in the proximal side is more physiological, and we believe that developing a method to find Ectsis type lymphatics in the proximal side reliably is essential to achieve full effect of LVA.
Footnotes
Author Disclosure Statement
No competing financial interests exist.