
Abstract
Abstract
Purposes:
Conventionally, lower limb circumference is measured using a measuring tape; however, a measuring tape may not provide sufficient precision to measure the magnitude of the lymphedema. We report the use of three-dimensional photography (VECTRA®) for the evaluation of lymphedema in patients after lymphovenous anastomosis (LVA).
Methods:
We calculated the percent error in measuring lower limb circumference with a measuring tape. We performed VECTRA before and after LVA and measured the change in volume. Because of the limitation of photographic range, the measurement of the entire lower limb was difficult using this approach. We were limited to thigh measurements.
Results:
The ratio of error was calculated using the largest and smallest mean measurements. The largest measurement errors, 4.3%–5.8%, were observed for the measurement of thigh circumferences, whereas the smallest measurement errors, 2.3%–2.9%, were observed in the foot and lower leg areas. The change in volume postoperatively measured using VECTRA decreased by an average of 35.1 cc.
Conclusions:
The evaluation with a measuring tape for the foot and lower leg region was useful because a lesser content of soft tissue was not influenced to the error by power. Contrarily, VECTRA was useful for measuring the thigh region because of the higher quantity of soft tissue, and the combination of both reduced the error.
Introduction
E
Materials and Methods
All data in this study were entered into a spreadsheet using Microsoft Office Excel 2013. The mean and standard deviation (mean ± SD) were calculated with EXCEL.
Measurements obtained with a measuring tape
From April 2013 to March 2014, measurements to assess the presence and magnitude of lower limb lymphedema were obtained from 50 limbs of 36 outpatients attending clinic following LVA at the Department of Plastic, Reconstructive and Aesthetic Surgery, Chiba University Hospital, Japan. The mean age was 57.35 ± 13.3 years and comorbidities included the following: 19 endometrial cancers, 14 cervical cancers, 1 rectal cancer, and 2 primary lymphedema. According to the clinical staging by the International Society of Lymphology, 17 most of the patients were type 2 (31 patients), the others were type 1 (3 patients) and type 3 (2 patients). Five patients were evaluated before the operation of LVA and the others were after the operation. All the patients performed conservative therapy. We evaluated the use of a measuring tape to estimate lower limb lymphedema by calculating the percentage error in the circumference measurements taken at six points on the lower limb. Duplicate measurements were taken from the following locations on the lower limbs: at the foot instep, around the ankle, around the largest circumference of the lower leg, at the patellar superior border, at the 10 cm cranial side from the patellar superior border, and around the thigh. In this case, duplicate means the same physician measure twice, it is almost same meaning as “repeat”. All the patients were measured between 10 AM and noon. Each measurement was obtained in duplicate. We divided the duplicate measures for each location, and we calculated the percentage mean difference for each of six locations measured on the limb.
Three-dimensional photography (VECTRA) measurements
From April 2013 to March 2014, VECTRA images of 21 limbs of 16 female patients were taken before and after LVA, and changes in volume (cc) were measured at the same hospital. The mean age was 55.12 ± 12.1 years and comorbidities included the following: eight endometrial cancers, six cervical cancers, one rectal cancer, and one primary lymphedema. All patients, except those with primary lymphedema, were status post pelvic lymphadenectomy. Lower limbs measured for lymphedema included the following: both legs in five patients, two right legs, and nine left legs. All the patients were measured at 10:00–12:00 AM because they were also outpatients both before and after operation of LVA. All the patients were restricted conservative therapy on the day they visited our hospital. All cases were performed under local anesthesia. The mean number of LVA anastomoses was 6.33 ± 2.05 (2–11), and all of them were performed by an end-to-side anastomosis. The location and total anastomoses of LVA were dorsum of foot 46, lower leg 53, and thigh 34. All the patients had ICG lymphography. Yamamoto et al. categorized secondary lymphedema into five stages based on ICG lymphography findings and demonstrated that the stage of ICG lymphography correlates with clinical severity.18,19 According to this categorization, there were 9 limbs of type 2, 10 limbs of type 3, and 2 limbs of type 4. In our hospital, the operative indication for LVA is type 2 and type 3. Because LVA is a less invasive method than vascularized lymph node transfer, one patient with type 4 who hoped to have LVA was performed. Of course, other lymphedema patients such as conservative therapy only could be evaluated by VECTRA, almost all the lymphedema patients were before or after the operation of LVA in our department. Therefore, we restricted LVA cases in this time.
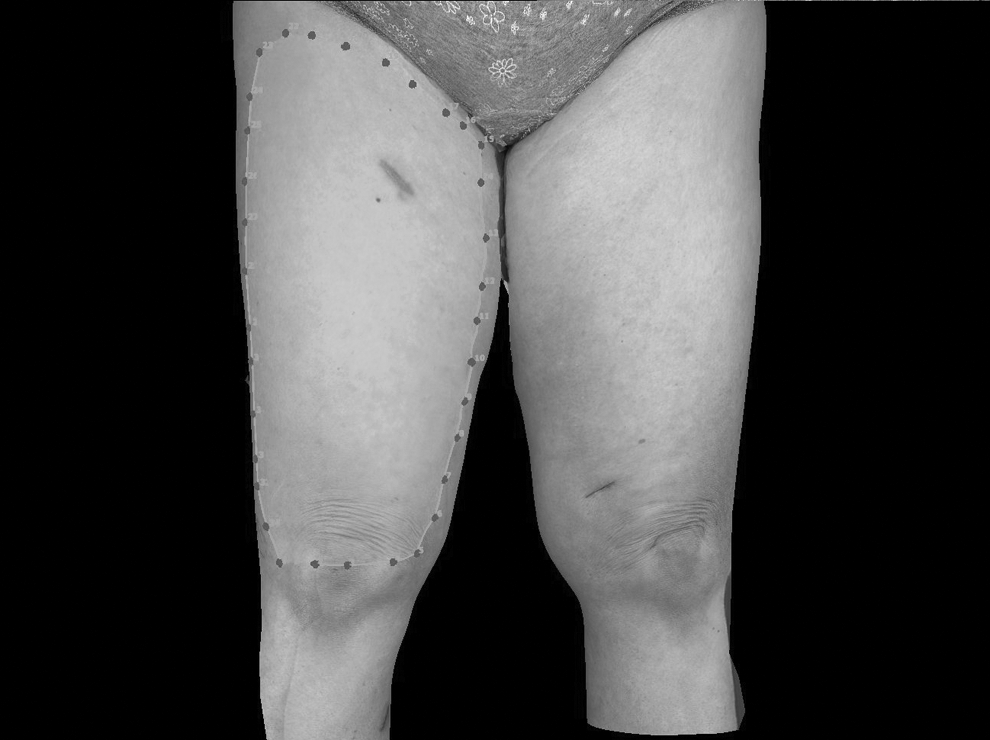
The mean follow-up period after LVA was 5.5 ± 1.69 months. The photography range of VECTRA was limited because the foot and lower leg were below the field of view. If the foot and lower leg were included to the range of VECTRA, it needed a footstep with the height very much. Such a footstep was dangerous and time consuming for the patients. We were unable to photograph the entire lower limb and the volume measurements were limited to the thigh. The measurement procedure was as follows. We put a footstool in front of the VECTRA device and marked the location of the footstool and the location where the patient's foot was placed on the footstool (Fig. 1). Three or more marks on the skin were used as points of reference in pre- and post-LVA images to evaluate the change in volume. We used unique skin anomalies for each individual, such as a nevus, a scar, or an epidermal capillary, as points of reference. We avoided using movable points of reference, such as knee joints. (Fig. 2). We compared the preoperative and postoperative VECTRA images and measured the change in volume. Increased volume appeared as light areas, whereas decreased volume appeared as dark areas in VECTRA images (Fig. 3). In the scale of this case, complete light color means the projection of this area increased 20 mm after the operation, and complete dark color means it decreased 20 mm. Between light and dark, the change in volume appeared according to the scale. We measured the change in volume as much as possible, including the area where both regions overlapped (Fig. 4).
Placement of foot stool relative to VECTRA®. We put a footstool in front of VECTRA and marked the place to put the footstool and the location where the patient was placed on the foot stool.

Preoperative and postoperative reference skin markings. We used at least three marks or anomalies on the skin, such as nevi, scars, or epidermal capillaries, as reference points on VECTRA images.
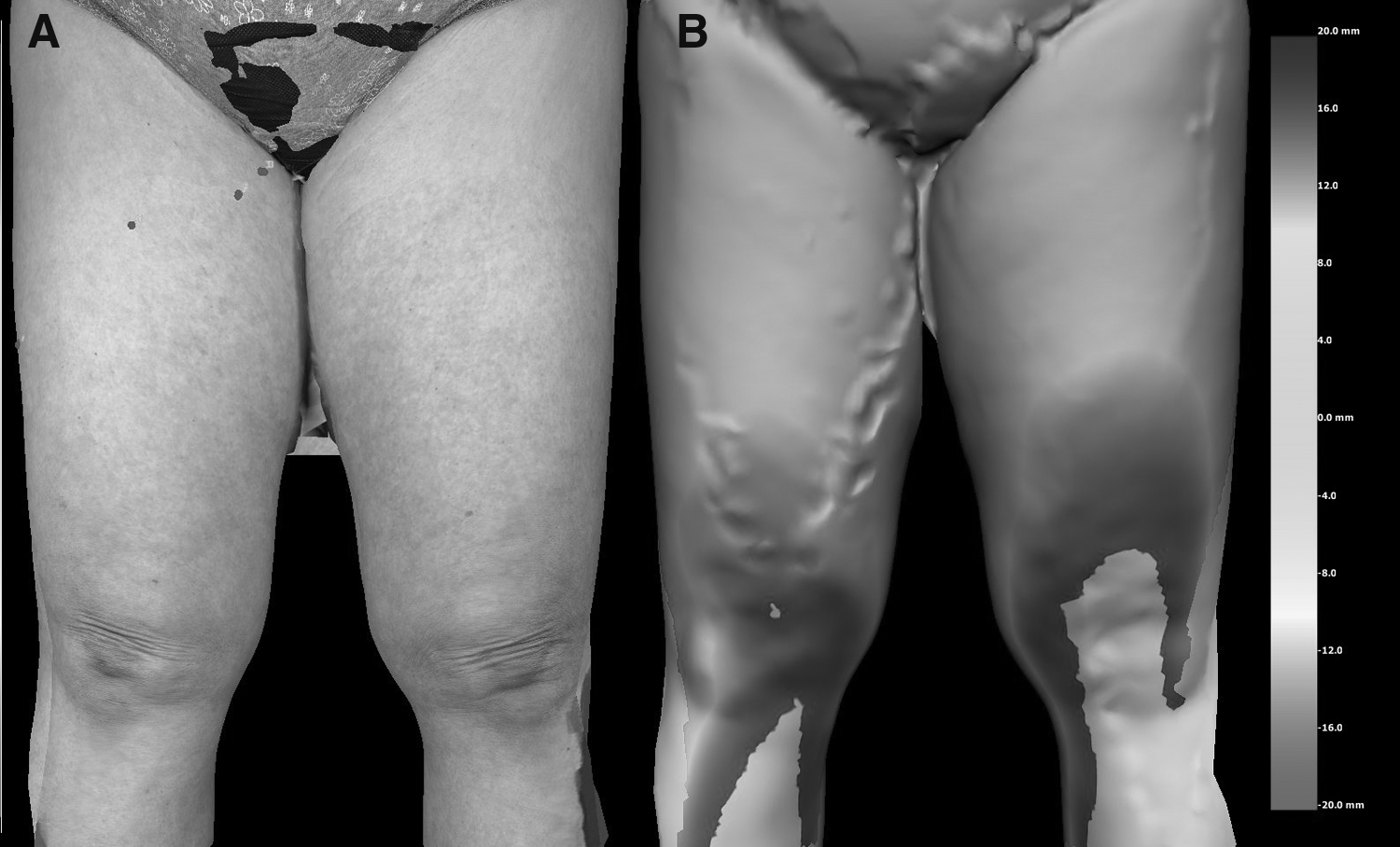
The photographs of VECTRA. After putting photographs together with VECTRA
The measurement capacity with VECTRA. We measured capacity change as much as possible, including the overlapping areas.
Results
Measurements obtained with a measuring tape
We measured twice when we measured a measuring tape milder and when we measured stronger. We calculated the average of the totals of the stronger measured value of all cases and a milder measured value each other, and defined the difference of the value of both as an error in this time. The ratio of error was calculated using the largest and smallest mean measurements. The largest errors, 4.3%–5.8%, were observed for the measurement of thigh circumferences taken at limb locations 4–6, whereas the smallest errors, 2.3%–2.9%, were observed in the foot and lower leg areas. (Table 1).
Calculation of Percent Error from Duplicate Measurements Taken Using a Measuring Tape at Six Points on the Lower Limbs Following Lymphovenous Anastomosis
The error in the thigh was bigger than the error in the foot and lower leg.
Three-dimensional photography (VECTRA) measurements
We defined a volume change of <5 cc as unchanging and defined the volume as increasing or decreasing when a change of >5 cc was observed. A decreased volume was observed in 11 limbs, increased volume was observed in five limbs, and no change in volume was observed in four limbs. The change in volume measured from VECTRA images demonstrated that postoperative mean volume change in thigh region decreased by 35.1 cc (Table 2).
The Change in Volume Observed Using VECTRA Photography
The postoperative one decreased at an average of 35.1 ± 98.8 cc.
Discussion
LVA is a microsurgical approach that makes a bypass between lymph and blood circulation. This bypass conveys congestive lymph fluid to venous circulation. LVA is performed through an incision of about 2–3 cm in length and the location of anastomosis is chosen according to ICG lymphography. Because LVA is less invasive and can be performed under local anesthesia, it in recent years it has become one of the most popular surgical treatments for lymphedema patients. Lymphedema symptom atology such as the occurrence of cellulitis episodes, is statistically decreased by LVA. 20 However, VECTRA can only evaluate the volume change. Onoda et al. suggest that the utility of LVA for most patients with primary lymphedema is not confirmed. 21 However, because LVA is a less invasive method than vascularized lymph node transfer we performed LVA here as well. Another study suggests that there is a beneficial role for LVA to prevent the progression of lymphedema when compared to conventional therapy alone. 22
Some reports suggest LVA can be effective in volume reduction of lymphedema, particularly in patients with early-stage upper extremity lymphedema. 23 However, in patients with late-stage lymphedema with few functioning lymphatic vessels and significant tissue fibrosis, LVA will not be effective in large volume reduction of lymphedema. 24 In this study, most patients had late-stage lower extremity lymphedema following much earlier dissection of lymph nodes. So the effect of volume reduction in the thigh region were such that, although it was effective in a few patients, the postoperative mean volume change only decreased by 35.1 cc.
Measurement of volume changes to estimate limb lymphedema using various approaches, such as water displacement method,16,25–27 bioelectrical impedance,28,29 and perometer,30–32 has been performed. However, these methods are labor intensive and time consuming for the patients. There were many advantages to using VECTRA for the evaluation of lymphedema in patients following LVA. The photographic speed (1.5 msec) and the ease of use of VECTRA were similar to that of a digital camera and the cost of taking VECTRA virtually nothing. In addition, using image analysis, we were able to quantify improvement, no change, or lack of improvement in lymphedema. Volume measurements were generated using a Bezier patch method, interpolating information from the boundary of the selected area to determine the enclosed volume. 15
We used a minimum of three unique skin markers as points of reference to aid in the calculation of volume changes and excluded movable points of reference, such as joints.
Because the photographic field of view was limited, VECTRA was not possible for evaluation of the entire lower limbs. Lymphedema increases the amount of soft tissue due to adipose deposition, fibrosis, and water content. Some studies have shown that the lymphatic system plays a key role in adipose physiology.33,34 Other symptoms such as dermal sclerosis and cellulitis confound the objective evaluation of lymphedema. Therefore, we evaluated the effect of LVA according to the volume change of soft tissue.
The soft tissue in the foot and lower leg region was less than that in the thigh and such a less soft tissue region was not influenced to the error by power in the measurement with a measuring tape. Therefore, the error in the measurement with a measuring tape was less in the lower leg region. On the other hand, because the thigh region had the higher quantity of soft tissue, the measurement with a measuring tape was easy to be influenced by the power. Therefore an error was easy to occur in the thigh region. So VECTRA was useful for measuring the thigh region because of the higher quantity of soft tissue, and the conventional evaluation with a measuring tape was useful for the foot and lower leg region. The combination of both brought down an error.
For this study, the evaluation of lymphedema was completed by VECTRA using lower limbs. VECTRA has been used to evaluate lymphedema of facial, pubic, and hypogastric sites. Because in these regions volume changes are difficult to evaluate using conventional methods, that is, using a tape measure, VECTRA has been especially useful in the evaluation of these regions. Because debulking surgery by liposuction is more effective than LVA volume reduction, it is thought, in particular, that it is more likely to be useful about the evaluation in that setting.35–37
Conclusions
We evaluated VECTRA as an approach to measure lymphedema of lower limbs following LVA. VECTRA was useful for the thigh region, and the combination of both, using the conventional evaluation with a measuring tape for the foot and lower leg region, was useful and reduced measurement error.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Ethical Standard
Hideki Tokumoto and other coauthors performed this study in accordance with the ethical standards of Chiba University Faculty of Medicine.