
Abstract
Abstract
Background:
Early detection and tracking of breast cancer treatment-related lymphedema have been helped by quantitative assessment methods and parameters, including bioelectrical impedance spectroscopy and tissue dielectric constant (TDC). Such measurements are evaluated with respect to interarm differences or ratios that (when exceeding specified thresholds) are suggestive of lymphedema. Specific threshold ratios depend on the assessment method and have been reported for arms. However, there is far less information available on thresholds to assess lymphedema that manifests in at-risk hands and essentially nothing known about TDC ratios in healthy hands. Such information is essential to establish reference values from which lymphedema threshold TDC values may be estimated. The specific aim of this research was to determine such interhand TDC ratios applicable to both young and mature women.
Methods and Results:
A total of 70 women (35 under 30 years of age, YOUNG, and 35 over 50 years of age, MATURE) participated after signing an approved institutional review board informed consent. TDC values of the hand dorsum web were measured bilaterally in triplicate with participants in a supine resting position. Results showed MATURE TDC values to be about 15% less than YOUNG (p < 0.01) on dominant and nondominant hands, but no statistical difference in dominant/nondominant interarm ratios (1.026 ± 0.100).
Conclusions:
Based on this data set's overall mean and two standard deviation value, an age-independent interhand TDC threshold ratio of 1.23 emerges as potentially useful for lymphedema detection. This is a good initial start threshold that is usable in future clinical and research assessments.
Introduction
E
In contrast to the availability of threshold ratios for at-risk arms, there is far less information available on possible thresholds to assess lymphedema that manifests in the at-risk hand, a significant deficiency as recently recognized.12,13 In part, this state of affairs is because hand parameter measurement methods are less available and less used. The historical gold standard of using water displacement volumetry (WDV) has provided important information in a number of areas. Hand volumes obtained by WDV from affected limbs of 20 patients with BCRL 14 indicated an affected hand to be about 78 mL (25%) greater than that similarly measured in dominant hands of 20 control subjects.
Contrastingly, when at-risk hands were compared with each woman's contralateral hand using automated optoelectronic measurements (Perometer®), these workers found an average difference of only about 24 mL (5.7%). Similarly, when both hands of 33 healthy subjects (20 females) were evaluated by WDV and compared with volumes calculated from a simple metric calculation model, 15 the dominant hand volume by WDV was 4.6% greater and was 4.3% greater using the calculation algorithm. Further analyses of these data that focused on hand volumes just of women showed that the average dominant hand volume (306 ± 55 mL) was 5.1% greater than the nondominant hand volume (292 ± 54 mL).
An additional hand volume procedure available is the figure-of-eight method, reported to have good concurrent validity compared with water displacement measurements in nonedematous hands.16,17 WDV measurements of 50 healthy subjects (37 female) showed the dominant hand to have about 5% greater volume. Application of the figure-of-eight method to 24 women with BCRL and visually apparent hand swelling showed it to also correlate with that measured by the gold standard water displacement method with an average edematous hand volume of 556 mL. 18 An evaluation of hand palm volume of 50 healthy subjects (30 female), based on calculations of BIS data, 19 indicated a 20.9 mL (9.1%) greater dominant hand volume. Contrastingly, when measurements of the same hands were done using the Perometer, dominant hands had a 10.8 mL (5%) greater volume.
As may be seen from the limited available data, there appears to be an ∼5% differential in volume between dominant and nondominant hands of healthy persons, but with considerable individual variation. A potential alternative to utilizing indicators of hand volumes as a way to characterize interhand lymphedema presence or to track its change is the use of interhand TDC values.
Prior work using this measurement as an index in the form of at-risk/contralateral ratio has shown itself not to be dependent on hand dominance. 20 This is an advantage, especially when baseline or presurgery measurements are not available since corrections for handedness dominance are not needed. However, there is essentially nothing known about such TDC ratios in healthy hands and its possible dependence on chronological age. Such information is an essential requirement to establish reference values from which lymphedema thresholds may be estimated. Thus, the specific aim of this research was to determine such potential thresholds based on the distribution and differences in interhand TDC ratios of both young and mature women.
Methods
Subjects
A total of 70 adult women participated in this study as volunteer subjects after signing an approved institutional review board informed consent. Included were 35 women who were less than or equal to age 30 (YOUNG, 25.1 ± 2.2; range 18–29 years) and 35 women who were greater than or equal to 50 years of age (MATURE, 67.3 ± 9.9; range 50–87 years) with all data given as mean ± standard deviation (SD). MATURE had a significantly greater body–mass index (BMI) than YOUNG (28.9 ± 5.4 vs. 23.7 ± 3.7, p < 0.001) with 43% of MATURE being classed as overweight (BMI 25.0–29.9 kg/m2) and 31.5% classed as obese (BMI >30 kg/m2). This BMI distribution is in contrast to YOUNG, in which 28.5% were classed as overweight and only 1 (2.85%) of the 35 subjects was classed as obese.
Most of the young women who participated were first- and second-year medical students, whereas the mature women who participated were from multiple sources, including faculty and staff. Entry requirements were that there be no history of hand or arm trauma or edema and there was no skin condition affecting the hand area to be measured. Three MATURE were self-reported left-hand dominant and two YOUNG were self-reported left-hand dominant. All others were self-reported right-hand dominant.
Measurements
Measurements were done while subjects were supine on a padded examination table with their arms resting at their sides, palms down. A target site located within and near the middle of the web space of the hand dorsum was marked on both hands with a small dot using a surgical marking pen. Figure 1 shows the TDC measurement device (MoistureMeterD Compact; Delfin, Kuopio, Finland) and illustrates the approximate location on the hand dorsum where measurements were made. The measurement is based on the principle that the dielectric constant as measured by an open-ended coaxial cable at or near a frequency of 300 MHz is largely dependent on the amount of water within the tissue. As a reference frame, pure water at a temperature of 32°C would have a dielectric constant of about 76.

TDC Measurement. The TDC measurement device is pictured in
The TDC measurement procedure requires that the device sensor (Fig. 1B) be placed in contact with the skin for 6–7 seconds whereupon the reading is displayed on the device readout. A built-in pressure sensor allows for reasonably consistent applied pressures to be achieved. For this device, the effective measurement depth is 2–3 mm where effective depth is usually defined as the depth at which the applied field falls to 1/e of its surface value. Measurements are taken on both hands in triplicate.
The procedure is to first measure the dominant hand once and then measure the nondominant hand and repeat this sequencing pattern twice more. This sequencing procedure helps minimize carryover of any of the immediately prior measurement effect. The average of the three measurements at each hand is taken as representative of the target site TDC value. For the current data set, the mean ± SD of the coefficient of variation for these triplicate measurements was 2.97% ± 2.24%. The use of TDC values as an index of skin tissue water has been widely reported and validated in the literature.21–26
Results
The major experimental results of this study (Table 1) show that TDC values measured on the hand dorsum of MATURE are less than measured on YOUNG on the dominant hand (p < 0.008) and also on the nondominant hand (p < 0.002). These MATURE-related reductions correspond to 14.1% in TDC for the dominant hand and 15.1% for the nondominant hand. The possible role of BMI differences was tested by grouping subjects above and below the median BMI of 26.0 kg/m2. The lower BMI group tended to have a higher TDC value (41.4 ± 7.8 vs. 37.7 ± 9.7), but the difference was not statistically significant (p = 0.095).
Data entries are mean ± SD TDC values for dominant and nondominant hands and the dominant/nondominant TDC ratio for 35 YOUNG and 35 MATURE. MATURE TDC values on both hands are statistically less than for YOUNG. However, there is no statistically significant difference in the ratio.
SD, standard deviation; TDC, tissue dielectric constant.
Despite significant differences in absolute values between age groups, the dominant-to-nondominant TDC ratio was similar for YOUNG and MATURE (1.017 ± 0.109 vs. 1.035 ± 0.090, p = 0.452). The distribution of TDC ratios for all 70 women is shown in Figure 2 along with a superimposed Gaussian distribution. The overall mean and median of the distribution are 1.026 and 1.027, respectively, with a standard deviation of 0.100. For this distribution, a plausible conservative reference threshold TDC ratio, above which would suggest the presence of hand lymphedema, is its mean value plus 2.0 SD, which equals 1.226 and practically can be rounded to 1.23. For the presently measured values, no subject's ratio exceeds this value and only one subject (1.4%) has a ratio greater than 1.200.
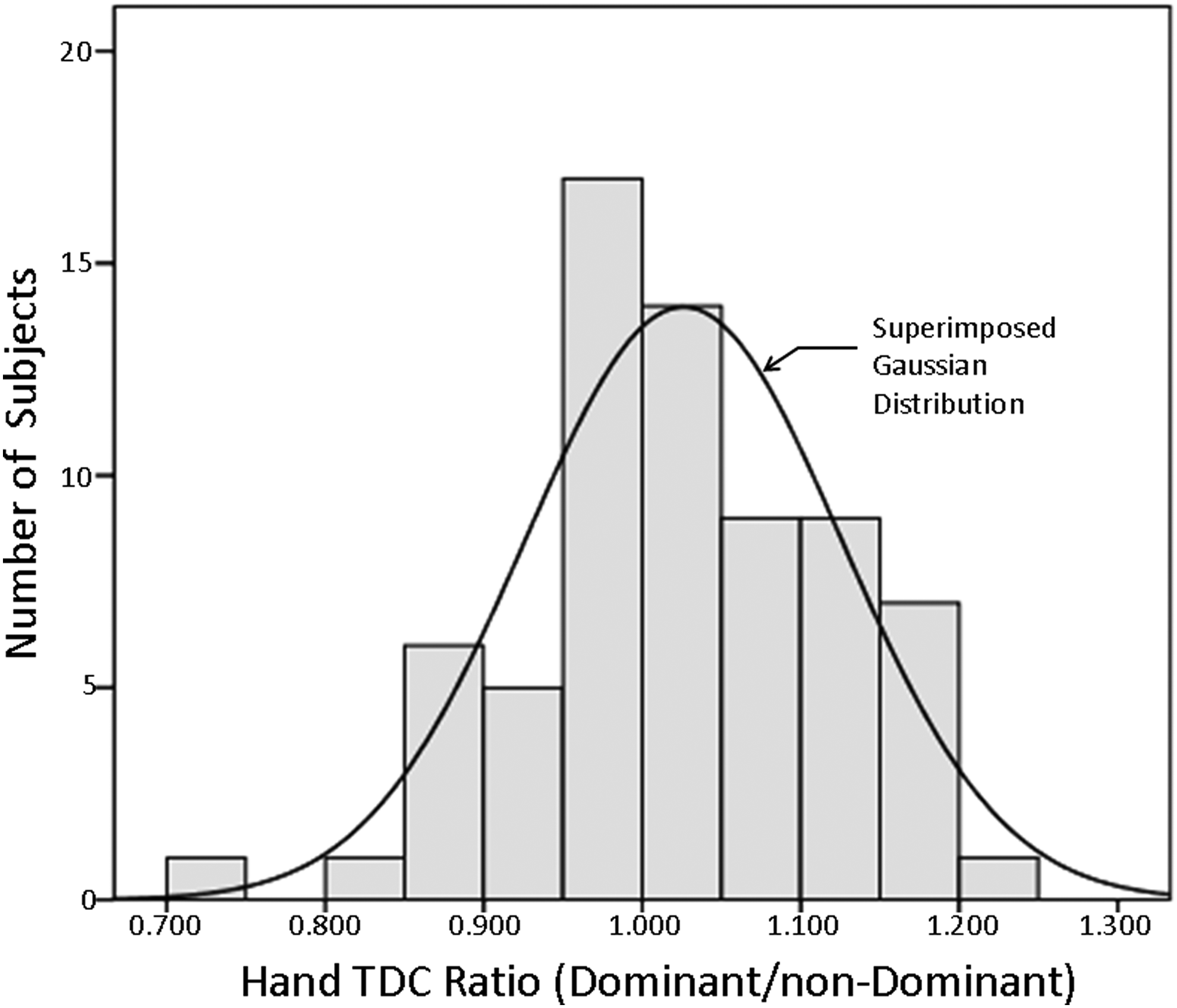
Distribution of hand TDC ratios for 70 women. Graphic shows the distribution of the dominant/nondominant hand TDC ratios for all 70 women who were evaluated. Mean value of the distribution is 1.026 with a median of 1.027. Standard deviation of the distribution is 0.100.
Discussion
The targeted specific aim of the present research was to provide a practical way to detect and possibly track hand edema or lymphedema using the method of TDC measurement. The hand dorsum web area was chosen for this initial investigation based on our personal observations that it is an area that sometimes becomes edematous. Based on the present measurement set, the interhand TDC ratio appears to be a useful parameter, in that despite variance in absolute TDC values among women of various ages, the ratio appears to be relatively consistent.
The threshold ratio herein suggested (1.23) is somewhat arbitrary since no measurements have as yet been prospectively made on lymphedematous hands to verify its efficiency. However, its formulation method, based on the mean plus multiples of the standard deviation of values obtained on nonlymphedematous targets, is similar to other successful approaches taken for developing lymphedema threshold ratios.27–29 Although it is clear that further follow-up research needs to be done measuring lymphedematous hands, the present reference measurements provide a framework for this to move forward in both clinical and research settings.
Footnotes
Acknowledgment
The authors wish to express their sincere thanks to the many volunteer participants without whom this research could not have been done.
Author Disclosure Statement
No competing financial interests exist.