
Abstract
Abstract
Background:
Secondary lymphedema is a complication following breast cancer therapy and constitutes the main form of lymphedema in the western world. The purpose of the current study was to provide a clear overview of the genetic predisposition and secondary lymphedema.
Methods and Results:
A systematic search was performed between February and June 2017 in MEDLINE and Embase. Search terms included Genes, Genetic Predisposition to Disease, Lymphedema, Breast Cancer Lymphedema, Secondary Lymphedema, Breast Cancer-Related Lymphedema, and Humans. Only original articles regarding the possible relationship between genetic variation and the development of secondary lymphedema in humans were included in this review. A total of 459 records were collected. After removal of duplicates, non-topic-related publications, and records not presenting original data, six full-text studies were included. Associations between genetic factors and the development of secondary lymphedema were found for variations in HGF, MET, GJC2, IL1A, IL4, IL6, IL10, IL13, VEGF-C, NFKB2, LCP-2, NRP-2, SYK, VCAM1, FOXC2, VEGFR2, VEGFR3, and RORC.
Conclusions:
In patients with secondary lymphedema following breast cancer therapy, genetic variations were found in 18 genes. These compelling, although preliminary, findings may suggest a possible role for genetic predisposition in the development of lymphedema following breast cancer therapy. This notion may add to the classical, more mechanistic explanation of secondary lymphedema.
Introduction
T
Lymphedema can be defined as a condition that arises when the lymphatic system fails to adequately drain fluid and macromolecules from the interstitium and to circulate lymphatic effector cells, resulting in the accumulation of protein-rich fluid in the interstitial space.6–8 Lymphedema develops when the microvascular filtration rate exceeds lymphatic drainage because the filtration rate is high, lymph flow is low or obstructed, or a combination of these two mechanisms. 3 Reduced lymph transport capacity may occur in association with cancer and its different treatment modalities, such as surgery, radiation therapy, and chemotherapy. 7 Lymphedema can occur in the viscera, genitalia, the head and neck, breast, and in one or more of the limbs, among others. 9 The condition remains an ongoing health problem for breast cancer survivors. 10
Traditionally, a distinction between primary (often congenital) and secondary (acquired) lymphedema can be made.1,4 Primary lymphedema is a rare genetic condition caused by mutations in the relevant genes for lymphatic development (lymphangiogenesis) or function, whereas secondary lymphedema might commonly start following trauma or cancer therapy, such as surgery and/or radiation to the axilla in the case of breast cancer.8,11
Research on possible risk factors for the development of lymphedema show largely inconsistent relationships, although evidence is mounting for treatment-, disease- and patient-related factors.6,7,11 However, it is evident that these risk factors may partially explain the development of lymphedema in breast cancer survivors, giving rise to the hypothesis that inherited genetic susceptibility may play a role in the pathogenesis of lymphedema following breast cancer therapy. 6 It is becoming increasingly apparent that the binary categorization of lymphedema into the primary and secondary variant might be inaccurate, as substantial overlap between primary and secondary populations can exist.1,9 It can be hypothesized that some cases of secondary lymphedema are conditioned by mutations in genes that cause primary lymphedema, thus influencing development or function; and that individual genetic variation in the response to lymphatic injury might contribute to a relative risk for or protection from the development of lymphedema following breast cancer therapy.11,12
To investigate the possible relationship between genetic predisposition and the development of lymphedema following breast cancer therapy in women, a systematic review of the literature was performed to assess the presence of genetic mutations in women with and without lymphedema following breast cancer treatment.
Materials and Methods
Eligibility criteria
All articles describing the occurrence of genetic mutations in women with and without lymphedema following breast cancer therapy were included. Female participants of any age following breast cancer treatment were considered. Studies describing the presence of genetic mutations in female breast cancer survivors were included. The presence of lymphedema was ascertained by means of clinical observation, lymphoscintigraphy, bioimpedance spectroscopy, perometry, and sum of arm circumferences. No minimum length of follow-up was determined. No restrictions regarding language, publication status, and year of publication were made for inclusion in this systematic review.
Information sources
Records were identified between February and June 2017 by searching the electronic databases Medline and Embase. The search was developed by two researchers (S.S.Q. and J.V.) and was conducted by J.V.
Search
The following search terms were used: ((“Genes”[Mesh]) OR (“Genetic Predisposition to Disease”[Mesh]) OR (gene) OR (genes) OR (genetic predisposition)) AND ((“Lymphedema”[Mesh]) OR (“Breast Cancer Lymphedema”[Mesh]) OR (lymphedema) OR (lymphoedema) OR (breast cancer lymphedema) OR (breast cancer lymphoedema) OR (secondary lymphedema) OR (secondary lymphoedema) OR (bcrl)) AND ((“Humans”[Mesh]) OR (human)).
Study selection
All the stages of the assessment of identified records (identification, screening, assessment of eligibility, and inclusion) were performed independently in a nonblinded, standardized manner by two reviewers (S.S.Q. and J.V.). Disagreements between reviewers were resolved by consensus. All retrieved records were screened based on their title and, if available, their abstract. With the exception of articles reporting on animal studies, no record types or study designs were excluded from eligibility assessment.
Data collection process
Before data collection from the included articles, a data extraction sheet was developed by two researchers (S.S.Q. and J.V.). This data sheet was based on consensual agreement of relevant factors for the assessment of the possible relationship between genetic predisposition and the development of lymphedema following breast cancer therapy. This data sheet was not pilot-tested on a selection of included studies. One review author (J.V.) extracted the predetermined, relevant data from the included studies. The second review author (S.S.Q.) checked the collected data. Disagreements were resolved by discussion between the two authors. No authors were contacted for further information.
Double counting of multiple reports of the same study was avoided by using a reference manager (EndNote). In addition, the presence of duplicates was assessed manually by juxtaposing author names, sample sizes, outcomes, and year of publication.
Data items
Information on the following was extracted from each included article: (1) patient characteristics (including number, gender, pathology, and treatment), (2) method of lymphedema diagnosis, (3) rationale for selection of candidate genes, and (4) reported genetic variations in secondary lymphedema. In addition, the reported affected genes were classified in gene families according to their overall function. The functions of the individual genes were also reported.
Risk of bias in individual studies
No interventions were being investigated and, consequently, no random allocation sequence of treatments was generated in the original articles. Assessment of genetic variation was performed blindly for lymphedema status in three of six included studies.7,11,13 No intention-to-treat principle was followed in any of the included articles, since no treatments were being allocated and investigated.
Summary measures
The presence of genetic variations in women suffering from lymphedema following breast cancer treatment was the primary outcome.
Results
Study selection
A total of six original articles were identified for inclusion in the review. See flow diagram in Figure 1.
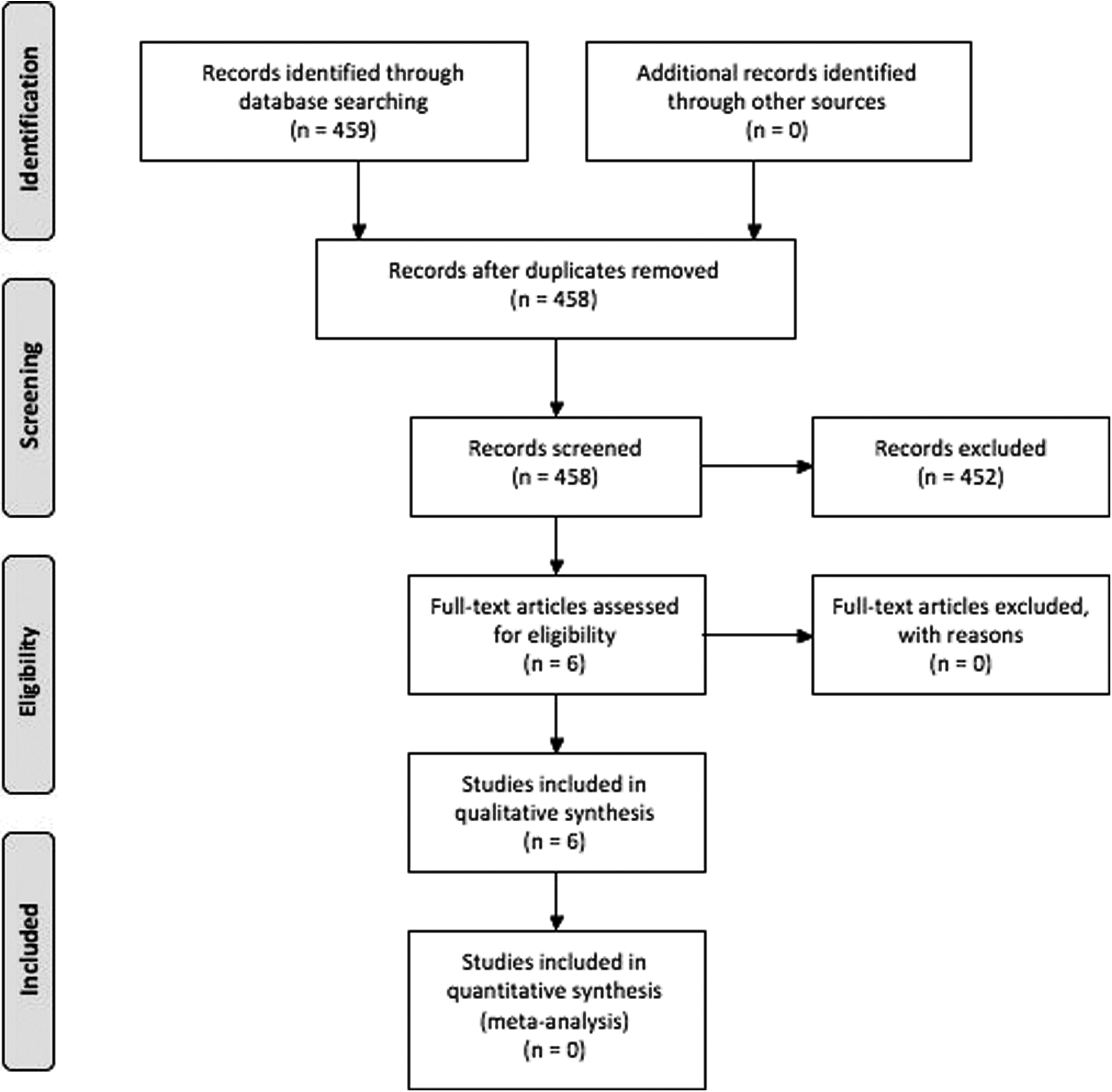
Flow diagram study selection according to PRISMA guidelines.
Study characteristics
The six included articles were based on one cross-sectional study, one case–control study, one prospective cohort study, one combined cross-sectional/longitudinal study on which two articles were based, and one nested case–control study. All articles were published in English. Only three of the six studies stated that analysis for genomic data was carried out blinded to lymphedema status.7,11,13
The studies included involved a total of 1379 participants. The inclusion criteria comprised female adults (18 or 21 years or older) with or without lymphedema of the upper limbs who were diagnosed earlier with primary and unilateral breast cancer and had received treatment (complete local excision, lumpectomy, or mastectomy with or without sentinel lymph node biopsy (SLNB), axillary lymph node dissection, radiation therapy, and/or chemotherapy), and were willing to provide a DNA sample. Candidate genes for genotyping were selected on the basis of earlier reports, known causative genes for primary lymphedema, genes in familial lymphedema/lymphangiogenesis, and inflammatory cytokine genes (Table 1).
CLE, complete local excision; NS, not supplied; SNP, single-nucleotide polymorphism.
Synthesis of results
Because of the study designs, patient characteristics, method of lymphedema diagnosis, and rationale for the selection of candidate genes varied markedly, the authors focused on describing the studies and their results in a qualitative manner rather than performing a meta-analysis.
Risk of bias within studies
No randomized controlled trials were included in this review, and hence, no interventions were allocated or investigated. Although the articles included represented different study designs, the primary outcome was determined through genotyping at one moment in time in all included records. By doing so, the primary outcome measure was determined in a cross-sectional manner.
Results of individual studies
In all studies, the primary outcome assessed was the presence of genetic variations in female breast cancer survivors. Genetic variations were found in 18 genes. These variations included several mutations in GJC2, leading to amino acid substitution and multiple single-nucleotide polymorphisms (SNPs) associated with a variety of genes involved in the development of lymphedema.6–8,10,11,13 These genes were HGF, MET, IL1A, IL4, IL6, IL10, IL13, VEGF-C, NFKB2, LCP2, NRP2, SYK, VCAM1, FOXC2, KDR, FLT4, and RORC (Table 2). However, FOXC2, HGF, MET, and FLT4 were excluded for mutations in the patient cohort, in which GJC2 variants were identified, contradicting the SNP-association studies. 11
FLT4, fms-related tyrosine kinase 4; FOXC2, forkhead box C2; GJC2, gap junction protein gamma 2; HGF, hepatocyte growth factor; IL, interleukin; KDR, kinase insert domain receptor; LCP2, lymphocyte cytosolic protein 2; MET, mesenchymal to epithelial transition; NFKB2, nuclear factor kappa B subunit 2; NRP2, neuropilin 2; RORC, RAR-related orphan receptor C; SYK, spleen-associated tyrosine kinase; VCAM1, vascular cell adhesion molecule 1; VEGF-C, vascular endothelial growth factor C.
Assessment of genetic variations in women suffering from lymphedema following breast cancer therapy showed a substantial overlap between the affected genes, identified in separate studies. This might lead to the hypothesis that the involvement of certain common genetic pathways might attribute to the development of lymphedema following breast cancer treatment. To elucidate the functions of these genes, an overview of these genes according to their function was performed (Table 3). Of these, four genes (HGF, VEGFR3, NFKB2, and FOXC2) were identified as playing an essential role in lymphangiogenesis and the development of primary lymphedema. 4
Discussion
Summary of evidence
All included articles reported on the association between genetic variation and development of lymphedema in women who had received breast cancer treatment. A total of 18 genes possibly associated with this type of lymphedema were found. Affected genes include GJC2, possibly HGF and MET, and possibly associated genes, IL1A, IL4, IL6, IL10, IL13, VEGF-C, NFKB2, LCP-2, NRP-2, SYK, VCAM1, FOXC2, KDR, FLT4, and RORC.6–8,10,11,13 Of these, only missense mutations in GJC2 affecting amino acids in the protein, connexin 47 (Cx47) may be causally linked to predisposing to lymphedema. 11 The remaining studies reported on SNPs associated with genes involved in the development of lymphedema. These SNPs are largely located outside the coding regions of their associated genes and are not linked to proved mutated proteins.6–8,10,13 A categorization of these genes according to their overall function revealed a substantial overlap with those mutated in the development of primary lymphedema due to erroneous lymphangiogenesis, supporting the notion that the traditional binary categorization of lymphedema into a primary and secondary variant might be inaccurate.1,4,9
Limitations
The level of evidence regarding the relationship between genetic predisposition and the development of breast cancer-related lymphedema was relatively low. The evidence was limited by small sample sizes, as recognized and described by different groups of authors.6,7,10,13 Risk of bias was introduced in three of six included articles by missing data on the method of genotyping; study-blinding of researchers for the participants' lymphedema status was not mentioned in these records.6,8,10 However, it can be postulated that the major limitation was provided by the degree of heterogeneity between the included articles. The method of recruitment of the study populations varied markedly, in addition to the heterogeneity in the definition of lymphedema. Moreover, the method of diagnosis of lymphedema differed across the included studies. Further limitations were conferred by preselection of lymphedema candidate genes, ruling out all possible associations with other genes and genes that have yet to be identified.
Conclusions
Through this systematic review, the authors assessed and reported the available evidence on the relationship between genetic variations and the development of lymphedema following breast cancer therapy in women. The current evidence may demonstrate an association between variations in 18 genes and the development of breast cancer-related lymphedema. The low level of evidence and the considerable heterogeneity of the included studies resulted in an inability to draw definite conclusions from the available literature. This underscores the need for a more complete, consistent, and standardized reporting of findings in future studies, preferably including larger numbers of participants, and an unbiased genome-wide association study to include all possible genes instead of preselected ones. In addition, future studies should be aimed toward the confirmation of previously performed genetic analyses and functional assessment of associated SNPs with their causal genes.
Footnotes
Author Disclosure Statement
No competing financial interests exist.