
Abstract
Abstract
Background:
Pneumatic compression has been used for more than 40 years in the management of lymphedema (LE). Modes of application have evolved with little consensus regarding optimal treatment parameters or dosage. The aim of this systematic review was to report the evidence for dosage of intermittent pneumatic compression (IPC) for people with LE and, particularly, that for upper versus lower limbs or child versus adult dosage.
Methods:
Medline, Embase, CINAHL, PubMed, and Scopus were searched with terms, including LE and IPC devices, with no restriction on time. Other materials searched included reference lists of included articles.
Study Selections:
Systematic review registration: PROSPERO ID: CRD42017054338. Studies were assessed according to PRISMA (preferred reporting items for systematic reviews and meta-analyses) guidelines and were excluded if they were not in English, not human, had physiological outcomes, or studied IPC in combination with other therapies. Quality appraisal, using the McMaster University Critical Review Tool, was undertaken by two researchers with differences resolved by a third. One hundred twenty-two full-text studies were screened for eligibility.
Results:
Sixteen met inclusion criteria for final analysis. Of these, four were reported separately due to concurrent use of compression garments during the study period. One randomized controlled trial met the requirements for a level II (National Health and Medical Research Council) rating; the remainder were level III-2 and below. Devices applying compression via multichamber sleeves were more commonly used in the past 20 years, with a trend toward lower pressures and shorter treatment times compared with earlier studies. Little evidence exists for application of specific dosage of IPC for children or a particular limb. New devices utilizing lower pressures support home use and self-management of LE.
Conclusion:
Low-level evidence of moderate quality shows significant outcomes achieved with dosage times of 45–60 minutes, applying pressures between 30 and 60 mmHg in sequential IPC programs. Methodological limitations in most studies suggest caution in drawing conclusions.
Introduction
Compression is the mainstay of lymphedema (LE) management. Intermittent pneumatic compression (IPC) is used as an adjunct treatment to compression garments (CG), bandages, and wraps; however, there is ongoing debate about optimal IPC dosage for the management of acute LE 1 and chronic LE. 2 Clinically, when CG are being prescribed, the level of compression is varied according to individual tolerance of pressure, upper limb (UL) or lower limb (LL), children or adult, and for early- or late-stage LE (according to the condition of skin and subcutaneous tissues). There are currently no guidelines to indicate how pneumatic compression dosage should be varied to optimize outcomes according to these factors.3–5
Lymphoscintigraphy6,7 has shown lymph movement in response to pneumatic compression with 50–125 mmHg pressure and near-infrared fluorescent lymphatic imaging (NIRFLI) 8 with low mean pressures (<15 mmHg). Fluid movement has been demonstrated after 3 hours, 6 1 hour, 9 and even 1–3 minutes 10 of IPC application. Hence, both optimal pressure and duration of compression for lymphatic movement are unclear.
Historically, single-cell IPC sleeves 11 and application of constant pressure gave way to sleeves with multiple cells or chambers and the development of varied time cycles to prevent backflow of lymph and address patient discomfort.12,13 More recently, IPC devices have been developed to replicate manual techniques of a therapist's hands, utilizing low pressure with short repetitive application moving progressively along a limb to simulate manual lymph drainage (MLD) 14 and sleeves that incorporate the root of the limb to clear the pathway for drainage.14–16
Varied application and dosage in IPC trials have resulted in a wide range of outcomes. 17 As well, IPC has mainly been investigated as an addition to standard decongestive treatment rather than in isolation, and hence, the effect of IPC alone remains unclear. In a recent systematic review of IPC for secondary UL LE, which included studies with contamination between interventions, only two of seven randomized controlled trials (RCTs) investigated IPC alone (both of which are included in this review). Understandably, the benefit of IPC was not clear from a meta-analysis of three RCTs where IPC was combined with complex decongestive therapy (CDT). 17
An earlier review (2010), focusing on IPC for UL LE, found a lack of evidence for (1) the benefit of IPC over skin care alone; (2) the benefit of one IPC cycle type over another (e.g., intermittent vs. sequential); and (3) lack of agreement over pressure dosage. 18 Few reviews have investigated the effect of IPC in isolation from other management strategies and no reviews have previously investigated dosage specifically. To date, flow has been explored by both imaging (lymphoscintigraphy, NIRFLI) and invasive methods (needle-wick measures); flow has been demonstrated in the LL under both low 8 and high pressures, 19 and the occlusion pressure of superficial vessels in the UL has been shown to be relatively high. 20 However, what pressure is both comfortable for a limb and producing optimal flow (indicated by a reduction in limb size of importance to the patient) over what length of time?
Studies using a combination of reduction therapies provide no information regarding the optimal dose of IPC that is safe, comfortable, and effective. This systematic review aimed to (1) identify the literature with outcomes of IPC alone applied to lymphedematous limbs with or without maintenance CG use; (2) review the quality of the research; (3) consider objective limb reduction outcomes to identify dosage that was most effective with least adverse effects; and (4) identify evidence for dosage specific to age or limb.
Methods
This systematic review was registered with PROSPERO (ID: CRD42017054338) (https://www.crd.york.ac.uk/PROSPERO/) and followed the PRISMA (preferred reporting items for systematic reviews and meta-analyses) protocol.
21
Databases searched included Medline, Embase, CINAHL, PubMed, and Scopus until March 2018. Terms included LE and IPC devices and were limited to English:
lymphedema/or elephantiasis/or non-filarial lymphedema/ Intermittent Pneumatic Compression Devices/ (((intermittent or pneumatic or sequential or lymphapress or lympha-press) and (compression or pump* or massage* or hose or device)) or impulse or ArtAssist or Flexitouch or FLOWTRON or Plexipulse or (SC-2004 adj Sequential) or Walkcare).tw, kf, hw. 1 and (2 or 3) limit 4 to English language
Screening of articles was undertaken by two people (J.J.P., S.J.G.); any difference in inclusion was resolved by discussion with reference to a third researcher if necessary.
Study selection
Studies included were peer-reviewed studies of National Health and Medical Research Council (NHMRC) level III-3 or higher, with IPC being the intervention under investigation or comparator where IPC was applied in isolation from other therapies, or if they incorporated the use of CG between IPC treatments (in accordance with clinically accepted maintenance therapy for LE management 22 ). Studies where CG were applied during the study period were assessed and reported separately.
Eligible studies provided objective limb reduction outcomes (such as limb volume or circumference) of greatest relevance and translation to practice for clinicians; those utilizing physiological or imaging outcomes, such as measures of lymph flow, were not included (e.g., Adams et al. 8 and Aldrich et al. 9 ). Studies were also excluded if they were retrospective, expert opinion, provided incomplete or variable dosage parameters, or the study population was not human or did not have LE. Studies investigating constant pressure devices were excluded, 23 as they are no longer used in practice.
Quality assessment and data extraction
Each study was critically appraised by two of three assessors (J.J.P., RP/AB) using the McMaster University Critical Review Tool, 24 a generic validated quantitative appraisal tool. Differences in appraisal were resolved by discussion, and where there was an unresolved difference, a third assessor (S.J.G.) was consulted. Critical appraisal scores were categorized as poor (≤8); fair (9–10); good (11–12); very good (13–14); and excellent (15). 25
Information relating to devices, dosages, and outcomes was extracted for all eligible studies (J.J.P.). Primary outcomes were limb volume or circumference; secondary outcomes included subjective response, skin or tissue assessment, or other objective assessments (e.g., bioimpedance). Dosage parameters of pressure, duration, cycle timing (inflation and deflation time, where available) were extracted, as well as sample characteristics, limb treated, and outcomes (percent volume or circumference reduction, if available; where this information was not reported in the publication but able to be calculated from the data provided, it is reported in italics). Clinical and statistical significance and adverse events were also extracted for both those investigating IPC alone and IPC in combination with CG.
Results
A total of 2173 studies were identified. After consideration of title, abstract, and full text, 16 studies met inclusion criteria and were accepted for critical appraisal (Fig. 1).
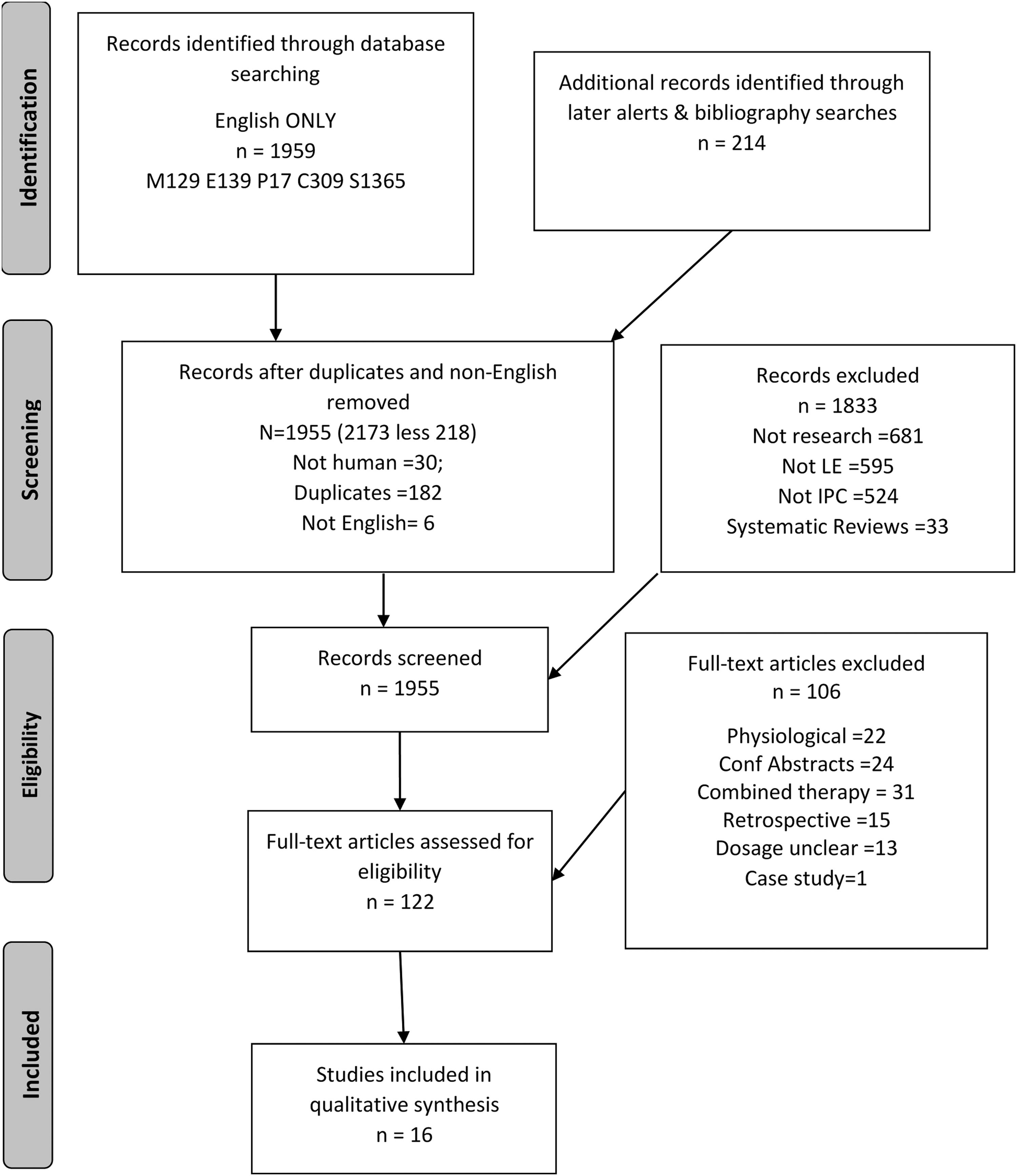
PRISMA (preferred reporting items for systematic reviews and meta-analyses) diagram 21 of IPC study selection. C, CINAHL; E, Embase; M, Medline; P, PubMed; S, Scopus. IPC, intermittent pneumatic compression.
Twelve studies reported the use of IPC alone and four investigated IPC with maintenance CG use between IPC treatments (IPC+CG). Several studies provided results for a device that is not currently commercially available and were excluded unless adequate information regarding dosage allowed replication with a current IPC device. Study characteristics, including population, intervention and comparators, and device and dosage parameters, are provided in Table 1.
Population, Device Characteristics, and Dosage
BC, bio compression; BP, blood pressure; CG, compression garments; Cycle, InfT+DefT; DefT, deflation time; Flowt, flowtron; FT, flexitouch; FTF, flowtron flowpac; FTP, flowtron plus; HF, hemaflow; InfT, inflation time; IPC, intermittent pneumatic compression; LL, lower limb; LO; L-P, Lympha-Press; MLD, manual lymphatic drainage; NHMRC, National Health and Medical Research Council; NR, not reported; PLE, primary lymphedema; Pn-L, pneumo-lymph; SLE, secondary lymphedema; UL, upper limb; WLP, Wright Linear Pump; SD, standard deviation.
Level of evidence
Of 16 studies, Dini et al. 26 (IPC alone) was the only level II (NHMRC) randomized controlled study. Berlin et al. 27 (IPC+CG) included a control group wearing CG only; however, participants were not randomized to group, so rated level III-2. Several studies commented on the ethical dilemma of a control group. Most other studies were either single-case design (before/after) studies or were comparative studies without concurrent controls (level III-3).
Quality of evidence
Comparative studies differed in population with relation to limb, stage, or duration of LE, resulting in nonequivalent comparisons between studies. Study limitations included selection bias (self-selection for group), baseline differences between groups, protocol variation according to participant response, lack of information regarding reliability of outcome measures, lack of evaluation of participant experience, lack of evaluation of between-group differences, and poor reporting and clarity of results (Table 2).
Outcome, Significance, Limitations, and Adverse Events
AE, adverse events; BIS, bioimpedance spectroscopy; Circ, circumference; NS, not significant; Pts, participants; TDC, tissue dielectric constant; Vol, volume; VTC, volume by truncated cone calculation; VWD, volume by water displacement.
Overall, the quality was poor for IPC-alone studies, with a mean score of 8 out of 15 (12 studies: range 4–11) and fair for IPC+CG studies: mean 9 out of 15 (4 studies: range 8–11) (Table 3).
Critical Appraisal Summary: Evaluation Questions from McMasters Critical Review Form (Quantitative Studies)
Population
Of the total number of people investigated in all studies, those with UL LE (338) were more than double those investigated with LL LE (151). Study sample sizes ranged from 9 to 67. The mean age of participants ranged from 37.8 (14–80) years 28 to 71 (54–83) years, 29 largely reflective of the demography of secondary cancer-related LE. Most studies investigated breast cancer-related UL LE; three included LL LE with a mixed population of secondary and primary LE30–32 and three investigated LL alone.28,33,34
Only one study investigated the use of IPC with children, in a sample of nine with a mean age of 13 years (5.5–17 years). 33
Study design
One study utilized a control group with skin care only, four IPC alone, two IPC+CG studies investigated the effect of one type of IPC device or dosage or sleeve configuration against another, and five studies investigated a cohort exposed to treatment with a pneumatic device, in a single-case pretest/posttest design. Remaining studies compared retrospective IPC results, manual lymphatic drainage, or IPC combined with exercises with a prospective IPC-only cohort. Study characteristics are described in Table 1.
Devices
The Lympha Press (Orthopaedic Appliances Pty. Ltd., Rowville, Australia, https://www.lympha-press.com/distributors/) (OR: Patriot Medical Distributors, West Chester, PA, www.patriotmedical.com) and Wright Linear Pump (Wright Therapy Products, Inc., Oakdale, PA) were the most commonly used devices (Table 1). Device- and manufacturer-specific factors such as the sleeve configuration, number of cells per sleeve, and the timing cycle of the pressure applied are aspects of dosage not controlled by the clinician in these studies.
Indeed, device variety resulted in differences between studies based on cycle time, sleeve configuration, number of cells per sleeve, and pattern of pressure application, quite apart from dosage (Table 1). Modes of compression described included the following:
While many studies compared one IPC with another, one investigated pressure time cycles with either single-cell or three-cell garments with the same device. 35 Having found significant reductions in all groups, it was concluded that all types of timing and sleeve configuration are effective. 35 In contrast, another study 32 reports that a 10-chamber IPC delivered a significantly greater reduction in percentage volume than either single-cell or three-cell devices. However, both studies had limitations that restrain conclusions (Table 2).
Duration of IPC application
Before 1995, IPC was applied for 4–9 hours per day30,33,36; then 2 hours per day26,31,32,37 in the late 1990s and reduced to 1 hour or less over the last 20 years.29,34,35,38–40 Two studies stand out against the norm of their era for applying IPC for longer (8-hour application in 2010) 28 and shorter (2-hour application in 1980) 12 durations.
Pressure settings
Older studies more than 20 years ago used higher pressures (100–150 mmHg), 12 while nearly all studies from the last 20 years applied pressure between 30 and 60 mmHg. The exceptions were two studies treating LLs that used 80–120 mmHg in 2010 28 and 100–120 mmHg in 2014, 34 and studies using the “mild” pressure Flexitouch device (Tactile Medical, Minneapolis, MN).38,39 The mean standard pressure of the Flexitouch is reported by Mayrovitz 15 to be 13.7 ± 4.9 mmHg for the preparation phase and 9.0 ± 4.2 mmHg for the drainage phase. In 1998, Johansson et al. 37 described application of 40–60 mmHg as being “standard practice” (Table 1).
High pressures common to the era (1991) (≥80 mmHg) were also applied to children. 33
UL versus LL pressures
Studies that included investigation of IPC for UL and LL applied similar pressure irrespective of the limb to be treated.30–32 Other than those using the low-pressure Flexitouch device, pressure between 30 and 60 mmHg was applied to the UL in five of six investigating UL LE,26,29,35,37,40 while those investigating LL LE used higher pressure (80–120 mmHg).28,34
Variation of pressure within a study
Pressure was varied (Table 1) according to the following:
Blood pressure. Maximum pressure was kept below diastolic blood pressure
35
and below the mean of the systolic and diastolic pressure in two.33,36 Skin resistance. Pressure was varied in opposite directions according to tissue condition in two studies, applying either higher
28
or lower pressure
35
in response to increased tissue hardness/fibrosis, with no description of how tissue hardness was determined.
Intervention period
The length of IPC use varied across studies, from one application of 16 minutes 29 to multiple applications over 3 years. 34 Intensity of treatment within the study period also varied from early intensive treatments of 16 hours over a 24-hour period (and hospitalization) to clinic-based studies of 5 weeks (25 applications) 35 or 20 applications over 9 weeks. 26 In contrast, the low-pressure device (Flexitouch) was investigated in home settings with daily applications over 30 days 38 and 84 days. 39
Outcome
Range of outcome measures
Circumference (10 studies) and volume (by water displacement; 6 studies) were the most common outcome measures reported (Table 2). Other outcomes were derived from dimensional measures: sum of the difference between limbs 26 or volume calculated from circumferences.38,39 Other outcome measures included tonometry, 34 tissue dielectric constant, 39 and bioimpedance. 38 Subjective feedback, quality of life (QOL), or symptom improvement were often discussed, but formally reported in only two studies.37,38 Outcomes of percentage reduction, where available, are reported in Table 2.
Greater response to intensive IPC was found in early than later stage fibrosis using xeroradiography. 30 Tissue softening was observed throughout 3 years of daily IPC using tonometry. 34
Adverse events
Fife et al. 39 alone reported comprehensively on the range of adverse events, their seriousness, and likelihood of being caused by the IPC, with seven events described as definitely (three), possibly (three), or unlikely (one) to be related to IPC use. Those definitely likely to be related to the IPC treatment included increased swelling of hand and torso; pain in axilla and back; and pain in forearm and numbness in fingers (Table 2). Possibly related events included swelling of lymph nodes in the contralateral axilla; breast inflammation with increased swelling and pain, infection, fibrosis, and increased arm swelling. Assuming 7 events affected 7 participants of a sample of 36, 19.4% is a considerable proportion to be affected. It is unclear how or when these events occurred or were resolved or if participation for those involved was discontinued.
Only three further studies reported adverse events; two related either to transient symptoms or to the issue of pain with high pressure settings where subsequent adjustment to lower pressures relieved pain in most instances.12,36 In the third, increased swelling was noted in 16%–25% of participants, dependent on group 27 with no further information on site or resolution. Generally, little or no information was provided about resolution of adverse events, particularly of increased swelling.
Discussion
This review of studies using IPC in isolation excluded many recent studies that applied concurrent cointerventions, such as bandaging or wraps,41–44 CDT,45–48 CG during IPC treatment, 11 or specific exercises,49,50 on the basis that the effect of IPC could not be isolated from that of other interventions.
Pressure and timing
Device parameters that are typically adjustable by the clinician or investigator include pressure and duration of application, in contrast with pressure cycle characteristics commonly specific to the device. Assessment of lymphatic function under a range of IPC pressures has used lymphoscintigraphy,6,51 histology, 52 and more recently NIRFLI9,19,20 providing evidence of lymph flow at both high and low pressures. However, damage to the lining of lymph vessels following 3–5 minutes of high-pressure manual massage (70–100 mmHg) was reported in 1995 in both dogs and people with LE. 52 These findings may have influenced the IPC dosage choices in subsequent studies.37,49
More recent assessment of lymph flow during IPC using NIRFLI has demonstrated optimal flow under pressures up to 80 mmHg 20 and in a comparison of low (45 mmHg) and high (90 mmHg), Kitayama et al. 19 demonstrated optimal flow at the higher pressure. Further studies have also shown fluid movement under high IPC pressure (80–120 mmHg), but with high pressures applied manually, little fluid movement was demonstrated. 10 Others using plethysmography 53 concluded high pressures and long cycle times were needed for fluid flow.
Further investigation of the interaction of IPC with the skin, where uptake of fluid is initiated in the initial lymphatics and where pressure is widely distributed around a limb in comparison with the focused manual application of pressure, may elucidate the optimal mode of application for fluid flow. Furthermore, it has been suggested that NIRFLI to outline fluid pathways before compression therapy might enable individually tailored IPC application. 9
Many factors influence IPC pressure applied to a limb (1) within the sleeve, (2) at the sleeve/skin interface, and (3) within the tissues, with the result that it is difficult to determine what pressure is translated to the tissues and if that is the key factor influencing lymph flow.
The pressure within an IPC sleeve cell has been reported to be higher than that set at the controls of an IPC, 54 yet the pressure in the tissues has been reported to be far lower than the pressure in the pneumatic sleeve cell. 53 Added to this, some investigators have varied pressure according to tissue resistance, on the basis that lymph flow is affected by this factor, and have applied decreased pressure for hard edema (and increased it for softer tissue) 35 ; whereas, conversely, others report much higher pressures were required to move fluid where there was significant tissue resistance caused by fibrosis. 55 Studies investigating tissue pressures during IPC, however, use an in vivo needle-wick pressure measurement method53,55 and cause alteration in the tissues due to the necessarily invasive nature of the method. 56
The role of tissue resistance in fluid flow under the influence of IPC was supported by in vitro simulations, although many assumptions were necessary to this model. 57 Furthermore, an investigation by Theys et al. 58 of pressure at the skin/sleeve interface has reported pressure differences depending on the surface to which it is applied: increasing by 25%–67.5% (dependent on device) with semi-rigid objects but remaining stable for rigid objects; and decreasing by 10%–15% for soft objects. While Pilch et al. 35 give no measurement criteria for rating edema hardness, the decrease of pressure for hard edemas and increase for soft edemas in that study agree with the findings of Theys et al., 58 at least on the skin surface. Outcomes may then, at least in part, be affected by individual characteristics such as tissue condition, and not dosage alone, in agreement with physiological investigations. 57
However, when the tonometer was indented to a depth of 10 mm, in a recent investigation of the pressure/flow relationship in different stages of LE, no correlation was reported between tonometry and stage; at least 1000 g/cm 2 force was required for flow (measured using the needle-wick method). 55 Further controlled studies of pressure applied to tissues of differing consistencies may elucidate optimal pressure settings for LE according to stage. Meanwhile, observation by clinicians of the response to IPC proportionate to relative tissue resistance may assist dosage decisions. (Clinical tools for measurement of tissue resistance are not readily available, a limitation for clinicians.)
Whatever may be demonstrated physiologically or in models, decisions on the optimal pressure and time cycle settings require translation of physiological findings into successful and safe clinical outcomes.
Dosage: evidence from studies with significant outcome
From this review, a limited body of available evidence was found, based on small samples of predominantly UL secondary LE, and equipment that may no longer be available; yet for dosage guidance, studies with significant outcomes and sound methodology, with no adverse events, are sought to provide the basis of evidence for optimal dosage and future research. No studies from this review met these criteria or scored in the upper quartile on critical appraisal (Table 3); those forming the basis for comment in this discussion have the best available rating, yet lack of adverse event reporting and methodological flaws indicate caution in adopting outcomes. Methodological limitations exist for those studies with the best outcomes:
- The greatest change of 32.6% mean volume reduction may be questionable due to lack of information regarding the effect of the crossover design.
32
- The next best outcome, within an IPC+CG study, was marred by seven adverse effects of varying seriousness and while statistical analysis indicated significant improvement, differences in control limb responses between groups raise questions over conclusions.
39
This study, while allowing usual home self-management to continue, was strengthened by assessment of factors that might have affected outcomes, yet on finding between-group differences, the significance of the difference was not reported.
A reduction in duration of application from 2 hours to 1 or less has occurred over the past 20 years in parallel with the growing need for independent, home-based self-management compared with treatment applied in a clinician-/clinic-centered model. Earlier still (1970–80s), treatments of 8–16 hours were common in a hospital inpatient model of care.30,36 Self-management models consider the time and burden of any treatment juxtaposed with the potential benefits resulting in the likely adherence to proposed treatment. The impact on the consumer and requirements of managing a chronic condition has been well documented.59–61
LE management requires at least once-daily attention, with most strategies (whether self-lymphatic drainage, or bandaging, garment, or IPC application) being particularly time-consuming. Dosage time for IPC application suggested by manufacturers has also decreased, perhaps reflecting both the development of multicell sleeves and sequential pressure applications, as well as being responsive to consumer uptake and needs.
Manufacturers' recommendations for devices that are common and currently available are for treatment duration of 1 hour or less: Medi-Rent's LX9 (30 minutes to 1 hour) 62 ; Lympha Press (60 minutes or less, once or twice daily; Lympha Press Protocol; Orthopaedic Appliances Pty. Ltd.). Flexitouch programs vary according to the area, with 45 minutes being recommended for LL only, 30 minutes for UL only, and 60 minutes for LL or UL with adjacent trunk. 63 Device evolution, utilizing different cycle times with sequential pressure, perhaps accounts for improved outcomes with shorter application time.32,35,39
Studies investigating LE self-care and IPC in home-based models generally administered IPC for 60 minutes or less16,38,64 or dependent on the surface area to be treated (greater the area, the longer the treatment time). 42 Given the time commitment required to manage LE, QOL, function, and patient satisfaction in use of IPC were central to studies of home use, as well as objective measures of LE reduction. Adherence to IPC home protocols has varied from less than ideal at 47% and 37% per group 16 to very high (95%–99%). 39 Further research could focus on home dosage programs that combine acceptable time burden for the consumer with satisfactory limb maintenance outcomes. However, even so, most studies report significant positive patient satisfaction and functional outcomes, along with decreases in health care costs, hospitalization, and outpatient care, from IPC use as part of participants' home-based LE management.16,42,64–66
Choice of optimal duration and pressure of IPC has been limited by the variation in aims, design, and study period of the above studies, which may have influenced outcomes. The number of times IPC was applied was one source of variation, and sleeve application another, with the root of the limb and upper affected side of the trunk sometimes included.38,39
The addition of chest and trunk to IPC treatment of the UL alone resulted in no statistically significant difference in objective (limb circumference) outcomes between groups 38 ; flow into adjacent truncal areas (from the LL across the inguinal crease) under IPC has not been demonstrated. 51 While a significant incidence of genital swelling has been identified in a retrospective study of IPC use, 67 reports of increased swelling at the root of the limb have been rare 39 or have not been found in others since,29,34 despite a reported increase in tissue pressure proximally. 68 Conservatively, clinical guidelines advocate the use of MLD to clear truncal areas and the root of the limb when the trunk is not included in IPC treatment. 69 The findings from NIRFLI of individual variation of drainage pathways and collateral flow 70 highlight the need for individual monitoring of response during treatment.
Despite these variations, small but statistically significant reductions have been demonstrated in studies using 30–60 mmHg, whether the IPC was applied for 2 hours or less than 1 hour26,32,35,37,39,40 (Table 2).
UL versus LL pressures
Studies in this review investigating both UL and LL applied similar pressure for both. In contrast, upper limits for compression pressures determined using bandages, have been reported to be different for UL and LL: 30 mmHg for UL and 50–60 mmHg for LL.71,72 While the nature of bandages is quite different to IPC, the latter study demonstrated bandaging pressures above this ceiling having a negative effect on limb volume reduction over a 2-hour period. 72 Differing IPC pressure settings according to limb have been applied in 1985 13 using maximum pressures of 110 mmHg for UL and 150 mmHg for LL. (The latter study 13 was excluded from this systematic review due to variation in dosage.)
The ceiling pressures described by Partsch et al. 72 contrast with studies using NIRFLI 20 and those using plethysmography (and needle-wick measures of pressure), 53 reporting lymph flow under IPC pressures of over 80 mmHg in the LL. Studies from this review investigating IPC use in LL applied between 60 and 120 mmHg in poor-quality, low-level evidence.
Child versus adult dosage
Only one study in 1991 investigated IPC in children: a level III-3 low-quality study with a cohort of nine 33 with inconclusive outcomes of significance. This pediatric study used pressures and device settings in the same range as described for adults in this review, with no comment on the generalizability of dosage from adults to children. Interestingly, pneumatic compression was applied overnight, as in 2 of the 15 adult studies,30,36 perhaps a reflection of practice common to the era.
Clinical meaning
The one highly rated RCT 26 found a mean 1.9 cm (11.8%) decrease in the sum of UL circumferences (compared with 0.5 cm decrease in a control group with only skin care) but deemed it clinically not significant, having set a value of 25% limb reduction to be clinically meaningful. In contrast, later studies have established that to patients, a reduction of 5% limb volume 73 or 8% limb volume 42 can produce positive benefits to QOL, highlighting the importance of including a measure of the outcome from a patient's perspective rather than objective measures alone.
Based on the findings of these latter studies, a reduction of 11.8% would be deemed clinically significant, produced with a dosage of 60 mmHg over 2 hours. 26 As the highest level of evidence available, this dosage is worthy of note. The next greatest reduction of 6.8%–9.6% limb volume was produced with half the IPC duration and a mean pressure of 37.7 mmHg. 35 Both studies applied IPC daily, although device characteristics differ; further investigation of daily versus less frequent application may further elucidate optimal IPC frequency.
A recent device applying lighter pressures (mean 9–13 mmHg) and using short treatment duration (30–60 minutes) has been used daily in conjunction with maintenance CG use over the longer term in home-based studies. 39 Limb reduction and other health-related outcomes, as well as consumer adherence to and satisfaction with maintenance programs, have been significant with the use of this light pressure device.39,66 However, this device was developed with the aim of supporting self-care by the patient at home, replacing therapist visits for MLD, 74 and has considerably different characteristics from other IPC devices14,15 currently available: the sleeve through which pressure is applied is of stretchy not inelastic fabric; pressure distribution and cycle characteristics differ from “standard” IPCs. Dosage appears to be in preset “programs” according to body area, 63 limiting comparative assessments of dosage.
Potential confounders
Bed rest
Five studies applied IPC for 4–8 hours or even longer at a time, often with little break before reapplying,12,28,30,33,36 requiring participants to be immobilized, often bed-bound for up to 16 hours in 24 hours of 1 day. Results from these studies must be viewed with caution, as even short-term elevation has been shown to reduce edema in ULs 75 and elevation is encouraged as an adjunct to management.22,76–78
Body mass index
Body mass index (BMI) is now recognized as a factor in LE 79 ; reporting on BMI was absent from one long-term study even where the unaffected limb was noted to have changed in size. 34
Adverse events
Only one study reported comprehensively on adverse events from IPC, despite using devices with some of the lowest pressures (9–13 and 30 mmHg) and shortest treatment time (1 hour). 39 This perhaps highlights the generally poor reporting of adverse events in the remainder. Of the seven events reported by Fife et al., 39 five were deemed serious; however, a significantly greater reduction was reported with the advanced programmable device, with only one adverse event, than in those using the standard device program, who did not experience any reduction. This study is one of only two in this review to assess IPC in a home-based model; however, variations in other usual activities (exercise) introduced between-group differences. 39
Limitations of this systematic review
This systematic review included only studies in English. The number of different outcome measures across studies, as well as the generally low level of evidence of moderate quality, limits the comparisons and conclusions to be drawn.
Conclusion
There is limited low- to moderate-quality evidence for the application of 45–60 minutes of 30–60 mmHg using multicell, sequential IPC programs for the management of UL LE. Whether the addition of the root of the limb and adjacent truncal area to the limb is necessary requires further investigation. 38 Further research on IPC outcomes, utilizing the same application frequency, duration, and pressures, will provide comparative data to build a basis for optimal dosage. The inclusion of outcomes beyond limb volume and dimension, such as tonometry and bioimpedance, will allow control for potential confounding factors such as tissue hardness (stage of LE) and broaden understanding of the impact of IPC on skin condition and fluid flow, relevant to LE management. The inclusion of patient-centered outcomes such as burden of treatment versus symptom management will add optimal IPC use to dosage outcomes.
Footnotes
Acknowledgments
Rotary Health for provision of scholarship to Jane Phillips. Murdoch Children's Research Institute for hosting Jane Phillips as PhD candidate. Ms. Poh Chua, Librarian, Melbourne Childrens Network, for assistance with search strategy. Ms. Alice Bradley and Ms Robyn Paterson, Flinders University, for critical appraisal.
Author Disclosure Statement
No competing financial interests exist.