
Abstract
Background:
Linforoll is a device composed of handpiece with roller and pressure sensor connected wireless to the computer displaying the pressure curve of the applied force. In a previous study, we proved it to regulate the applied force according to the hydromechanic conditions of the massaged tissues. Standardization of massage based on applied force was repeatable in the same patient; it decreased limb volume and provided evident increase in tissue elasticity.
Methods and Results:
In this study, we measured additional parameters useful for the understanding of tissue and fluid events and approval of the device for general practice. These were skin stiffness, subcutaneous tissue stiffness independent of skin, skin water concentration, changes in skin temperature, skin capillary blood flow, subcutaneous tissue fluid pressure, volume of the moved edema fluid, and visualization of movement on indocyanine green (ICG) lymphography. Measurements were done before and during the massage. The data were obtained from a group of 20 patients with obstructive lymphedema of lower limbs during the Linforoll massage. There was a lack of significant changes in skin stiffness, skin water concentration, skin surface temperature, and capillary blood flow, but evident increase in the subcutaneous tissue elasticity (tonometry) and lymphography-shown flow of the edema fluid.
Conclusions:
The skin tissue hydromechanic parameters remained normal proving lack of destructive changes under high massaging pressures.
The obtained data evidently show that not the skin but the subcutis accumulated edema fluid that can successfully be moved proximally under pressures of 80–120 mmHg.
Introduction
In the limb lymphedema, excess fluid should be evacuated to the sites where it can be absorbed. It should be moved either to the hypogastrium or arm/scapular regions along tissue channels. To propel the fluid external force, it is needed to generate in-tissue fluid pressure gradients. The manual lymphatic drainage of limb tissues with lymphedema is an effective therapeutic method; however, there is no knowledge on what happens to tissues and edema fluid during massage. The effects of massage depend on the therapist's manual technique, applied force, massaging regions, direction of the massaging movements, and duration. The basic disadvantage of the routine manual technique is lack of knowledge of the level of force applied to tissues and the generated solid tissue/edema fluid events under the skin. 1
This being so, the question arises whether the manual massage technique could be standardized by using a device with a known pressing area and continuously measuring the applied force while moving toward the root of the limb. Using such a device the physics of drainage would be repeatable and reproducible by others. Moreover, force could be adjusted to the stiffness of the massaged tissues that varies at different levels of the limb, as well as to the volume of soft tissues and accumulated edema fluid. Importantly, the unidirectional flow could be obtained with a manual device without backflow that is usually seen during the classic manual massage. In lymphedema, the main collecting trunks are obstructed and stagnant tissue fluid accumulates in spontaneously formed channels.2,3 Direction of flow of fluid during massage is crucial for a positive effect.
The device with a force measuring item was constructed by a group of engineers from Cizeta Medicali, Italy, under the name of Linforoll. 4 The rationale for such a construction was that this device should be effective in generating edema fluid pressure gradients, allowing fluid to move to the nonswollen parts of the extremity. To evaluate the effectiveness of Linforoll massaging, a number of edema fluid parameters should be measured. In the first clinical study of Linforoll, we measured tissue tonometry, limb circumference, and fluid flow. This device provided the possibilities of the following: (1) regulating the applied force according to the hydromechanic conditions of the massaged tissues; (2) standardization of massage repeatable in the same patient; (3) decrease of limb volume; and (4) evident increase in tissue elasticity. 4
In the present study, we measured more parameters useful for the understanding of tissue and fluid events and useful for approval of the device for general practice. They are stiffness of skin and subcutaneous tissue, skin water concentration, changes in skin temperature, skin capillary blood flow, subcutaneous tissue fluid pressure, volume of the moved subcutaneous fluid, and flow visualization on indocyanine green (ICG) lymphography during massage (Fig. 1). These parameters were obtained during Linforoll massage in a group of 20 patients with obstructive lymphedema of lower limbs. Lack of significant changes in skin stiffness, water concentration, surface skin temperature, and capillary blood flow, and evident increase in the subcutaneous tissue elasticity (tonometry) and lymphography-shown flow of the edema fluid provided clear evidence of no tissue damage but effective edema flow. The obtained data evidently show that not the skin but the subcutis accumulated edema fluid that can successfully be moved proximally under pressures of 80–120 mmHg.
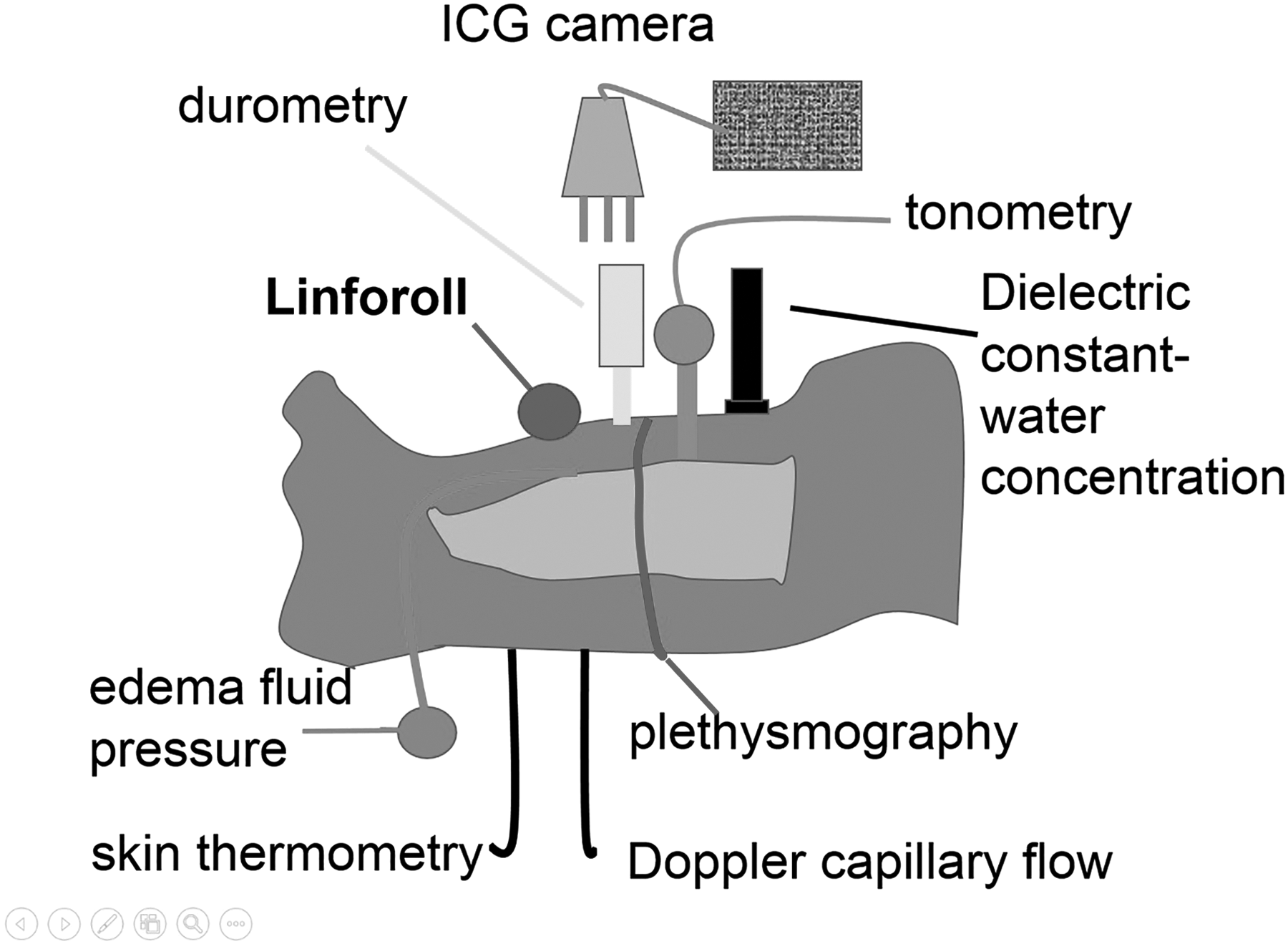
The scheme of clinical tests of tissue hydromechanics in lymphedema of the limb for evaluation of the effects of Linforoll massaging. Subcutaneously placed pressure sensor documents mobile fluid pressure located between dermis and muscular fascia. Dielectric constant measuring gives insight into skin water concentration at the depth of 2.5 mm. Durometer measures stiffness of skin and deep tonometer that of subcutis. Infrared thermometry and Doppler capillary flow are measured. Strain gauge plethysmography measures changes in circumference during fluid proximal movement. ICG fluorescence camera follows edema fluid movement. Changes of fluorescence level are shown. ICG, indocyanine green.
Materials and Methods
Patients
Lymphedema of lower limb. Study was carried out on 20 patients, ages 28–68, mean weight 72 kg (58–76), mean height of 168 cm (159–178), with diagnosis of lymphedema of one lower limb, stage II and III, and duration of 2–12 years. Cases with acute inflammation, chronic venous insufficiency, and systemic etiology of edema were excluded from the study.
The consent of patients was obtained and the study was approved by the Warsaw Medical University Ethics Committee.
Clinical staging
Staging was based on clinical evaluation: level of edema embracing limb from foot to groin and degree of skin keratosis and fibrosis. Briefly, in stage II, pitting edema affected foot and lower half of the calf, in stage III foot and calf were involved, with hard foot and ankle area skin.5,6
Lymphoscintigraphic staging
Evaluation of lymphatic pathways was done on lymphoscintigraphic images. In stage II, there was spread of tracer in foot and lower part of calf, interrupted outline of a single lymphatic and few small inguinal nodes with irregular outline. In stage III, no draining lymphatics were seen, with some inguinal nodes of irregular outline appearing after 2 hours.5,6 In stage II and III, edema has a pitting character, whereas in more advanced stages, fibrosis of skin requires additional compression force. The compression by Linforoll would be spent not only on fluid movement but also on deformation of hard skin. This would contrast with the aim of study to measure force necessary for deformation of the subcutaneous tissue.
Description of the device
Linforoll is a handpiece with a roller containing pressure sensor transmitting wireless the signal to the computer software program displaying on the screen the values of applied force during the whole rolling cycle (Fig. 2). It is calibrated from 0 to 150 mmHg. The number of cycles/time unit is recorded. Rolling at pressures of 40–150 mmHg is signaled by green light, whereas exceeding the top pressure lights up red light. 6 The pressing surface of the roll is 10 cm2.

Linforoll has a soft rubber roll of an area of 10 cm2 and an installed pressure sensor in the handle. Pressure can be read off on the computer screen. Applied force can be adjusted during rolling to tissue stiffness along the whole limb.
Limb massaging technique with Linforoll
The anterior aspect of the calf was massaged 20-times with a speed 6/min at pressure of 80–120 mmHg. The direction of rolling was based on the anatomical positioning of peripheral lymphatics running toward the knee. The rolling force was hand-adjusted between 80 and 120 mmHg, depending on the stiffness of tissues along the Linforoll truck. The resistance to rolling is felt during the procedure depending on the local tissue hardness and fluid accumulation. Applying different force at various limb levels enables fluid movement from the resistant with less force used at soft regions.
Skin tonometry (durometry)
Epidermis and dermis in the calves have a vertical dimension of 100–300 μm. In advanced-stage skin, structures become thicker, reaching 300–500 μm. Thus, a significant force should be applied to deform skin to move fluid. To estimate how much force to use the superficial tonometry, measuring skin stiffness becomes useful. We applied the recently developed skin durometer (Delfin Technologies Ltd., Kuopio, Finland). 7 This instrument utilizes a small measurement probe (diameter of 23 mm) that is briefly pressed on the skin at all anatomical sites, including curved region. The presence and severity of fibrosis are assessed by using a special three-dimensional computational finite element to analyze the biomechanical response of skin tissue to external force. It measures stiffness 1.25 mm deep. Values are expressed in Newtons (force 1 kg·m/s2, 1 N = 0.0981 kg).
Skin tissue dielectric constant: water concentration measurement
The device (Lymph Scanner; Delfin Technologies Ltd.) used consists of four open-ended coaxial probes intended to measure tissue water at effective depths from 0.5 to 5 mm. 8 When the probe is gently placed on the surface of skin, the measurement starts. After 5 seconds, the dielectric constant of the measurement site (i.e., the dimensionless tissue dielectric constant [TDC] value) can be read on the device display. The TDC values of the biological materials range typically between 20% and 50%, corresponding to the tissue water content of about 25%–60%. The measurement reading is reported as the percentage of water content. Measurements were taken at the same levels as those of tonometry.
Skin infrared thermography
Skin temperature (thermal radiation) measurements were performed using a high-resolution infrared (IR) camera (FLIR5; FLIR Systems AB, Danderyd, Sweden). The IR camera was placed ∼50 cm above the calf. The software Therma CAM Researcher Pro 2.10 from FLIR Systems AB was installed in a PC laptop and used to capture the IR images and for data postprocessing. 9
Skin laser Doppler velocimetry
The technique is based on the emission of a beam of laser light. The light is scattered and partly absorbed by the studied tissue. Light hitting moving blood cells undergoes a change in wavelength (Doppler shift), whereas light hitting static tissue is unchanged. The magnitude and frequency distribution of these changes in wavelength is presumed to be related to the number and velocity of blood cells. 10
Deep tissue tonometry
Tissue tonometry was performed at the same levels as those of girth measurements. A deep tissue tonometer was used. It was composed of a manometer (Wagner, Seattle, WA) connected to a 10-mm-long round-bottomed shape plunger of 1 cm2 surface area. It was pressed against tissues to a depth of 10 mm within 5 seconds. The applied force was read off on the manometer scale and expressed in g × 103/cm2. 11
Tissue fluid pressure measurement
The wick-in-needle technique was used as previously described. 12 Briefly, an 8-gauge injection needle with a polyethylene tubing (outside diameter 1.34 mm) containing glass-wool wick, protruding 5 mm from the tubing tip, was introduced under the skin at a depth of 5–10 mm. The needle was withdrawn, whereas the wick-in-tubing remained in situ. The outer part of tubing was fixed to the skin by adhesive tape. It was led out through an opening in the compression sleeve and then connected to the pressure transducer (Honeywell; Elblinger). Recording was done using a three-channel device, pressure range −20 to +150 mmHg (Telsoft, Warsaw, Poland), and LabVIEW software (National Instruments, Austin, TX). The data were collected using the Microsoft Excel program and were presented graphically on a pressure/timescale.
Continuous limb circumference measurement
Strain gauge plethysmography was used to measure circumference changes in the calf (Fig. 3). Briefly, a plethysmograph (type EC6; Hokanson, Bellevue, WA) in a recording vein mode was applied. Two mercury strain gauges were put around the limb at midcalf and below knee. Elongation of the gauge was read off on the recorder graph scale in mm of length and used as a factor for calculation of circumference increase. 4
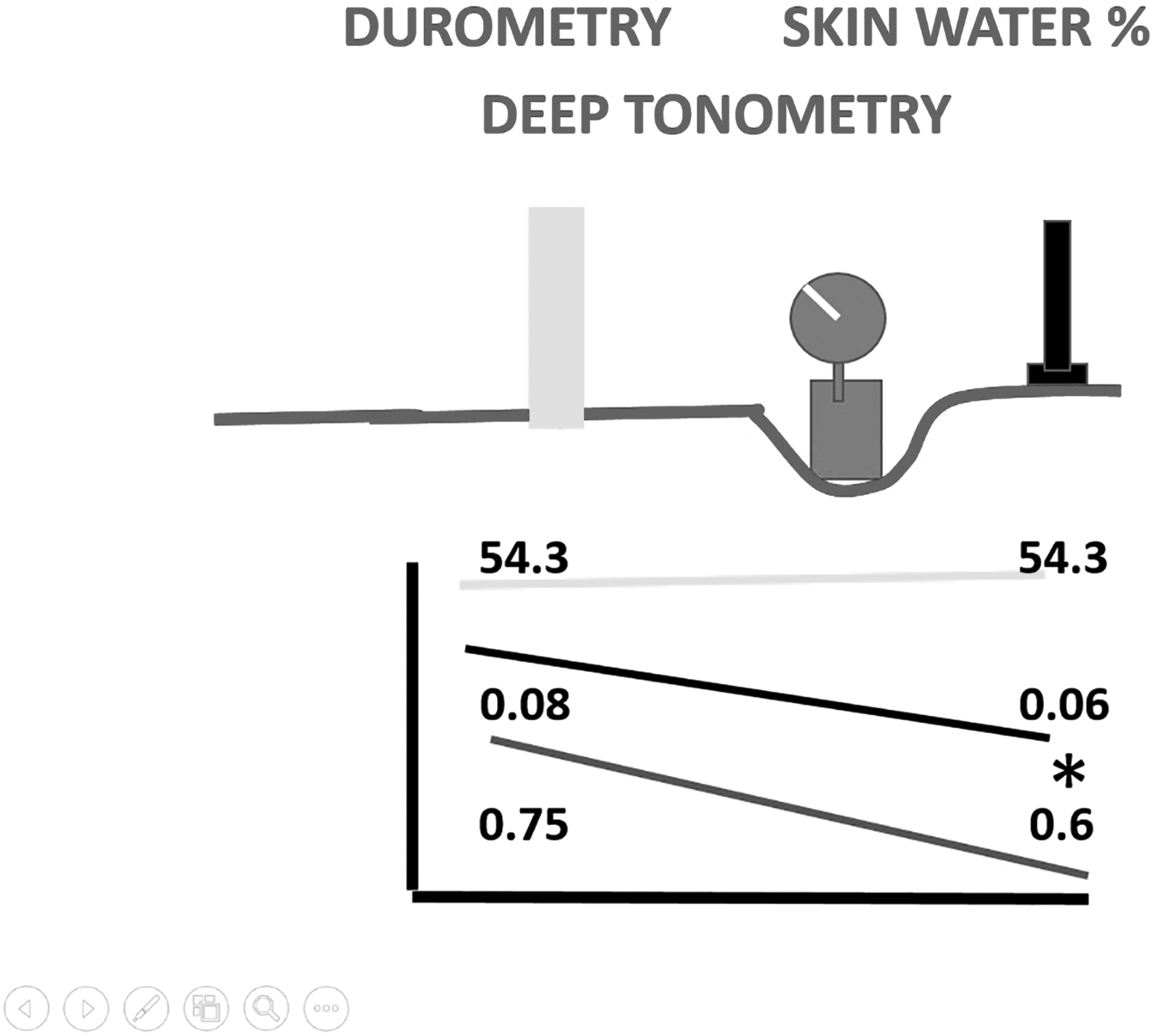
Results of dielectric constant (skin water concentration, %)—upper curve, skin stiffness (durometry, Newton)—midcurve, and subcutaneous tissue stiffness (deep tonometry, kg/cm2)—lower curve, after 20 Linforoll strokes in the midcalf. Note lack of changes in skin water concentration and durometry, but statistically significant decrease of subcutaneous tissue stiffness (*p < 0.05).
ICG near-infrared lymphangiography
The near-infrared (NIR) fluorescence imaging fills a unique need for simultaneous evaluating lymphatic architecture and function and edema fluid distribution. 10 ICG is a tricarbocyanine dye that is administered at a total dose <25 mg. ICG solutions can be excited between 760 and 785 nm and fluorescence imaged between 820 and 840 nm. A dose of 0.2 mL of 0.5% ICG (Pulsion, Munich, Germany) was injected subcutaneously into the second and fourth toe web or hand interdigital tissue. An ICG fluorescent lymphangiography system (Photodynamic Eye; Hamamatsu Photonics) was used. The charge-coupled device camera has a fixed focus ranging from 15 to 25 cm, which allows investigation of a 10 × 10 cm2 field with one image. Spread of dye in tissue spaces and areas of its distribution in subcutis was evaluated before and after compression. The level of fluorescence was measured using IC-CALC 2.0 software (Pulsion) and presented as a curve from the entire length of the limb. 13
Statistical evaluation
Skin durometry was expressed in Newtons, water concentration in %, surface temperature in degree (°C), and capillary perfusion/red cell velocity in mV. Subcutis tonometry data are shown in kg/cm2 and edema fluid fluorescence in %. For statistical evaluation of differences of the same patient before and after compression cycle, a double-tailed t-Student's test was applied with statistical significance at <0.05 level.
Results
Skin tonometry (durometry)
Skin durometry decreased on an average from 0.08 to 0.06 N (Newtons, force 1 kg·m/s2, 1 N = 0.0981 kg) (Fig. 3). The differences were not significant.
Skin water concentration
Skin water concentration remained at a level above 50% and did not change significantly after rolling (Fig. 3).
Skin infrared thermography
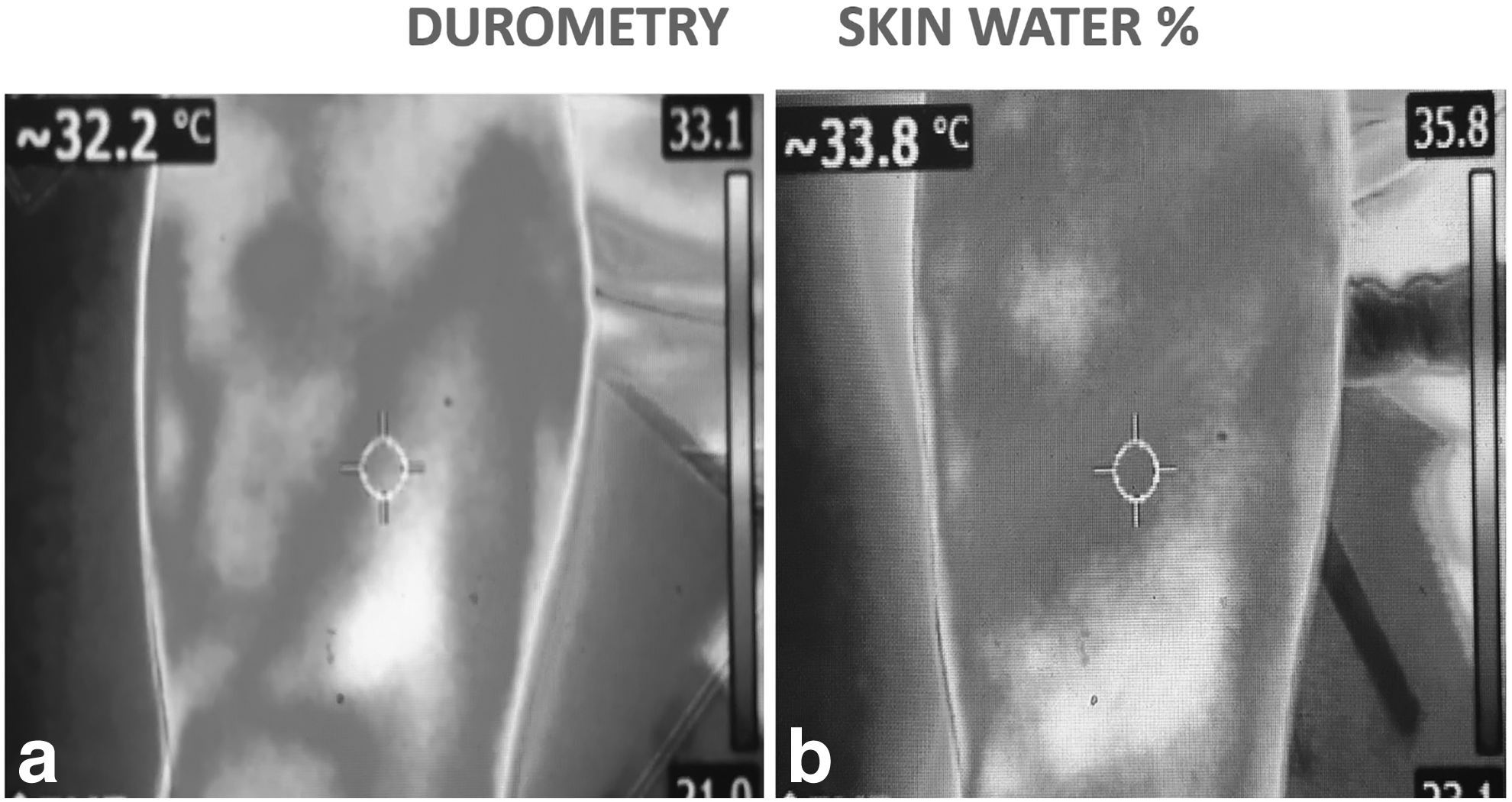
There was an average increase in surface temperature by 1°C. This was most likely caused by transfer of mechanical energy from the massaging Linforoll handle (Fig. 4a, b). No deep tissue temperature was recorded.
Skin infrared thermometry before
Skin capillary Doppler erythrocyte velocity
Midcalf skin capillary flow is low under rest and room temperature. It ranged before rolling between 1 and 10 mV, to decrease to zero after the procedure (Fig. 5). This difference was seen in all patients.

Point Doppler capillary flow measurement (in mV) after 20 Linforoll strokes in the midcalf. In all investigated cases, a decrease in the capillary flow was observed. This was the effect of rolling pressure on the dermal capillaries.
Skin and subcutaneous tissue tonometry
There was an evident decrease in the epifascial soft tissue stiffness from 1.1 ± 0.2 to 0.6 ± 0.2 kg/cm2 (p < 0.05) (Fig. 3). This result included a sum of skin and subcutis stiffnesses. Since the skin stiffness (durometry) did not change significantly, the entire stiffness decreasing effect of Linforoll should be attributed to the movement of fluid from the subcutis.
Tissue fluid pressures generated during rolling
Tissue fluid pressure under the rolling part depended on the force applied through the handpiece. It was in all cases 30%–50% lower than on the Linforoll screen (Fig. 6). The mean values were 46 ± 12 g × 103/cm2 compared with the applied in the roller of 80 mmHg.
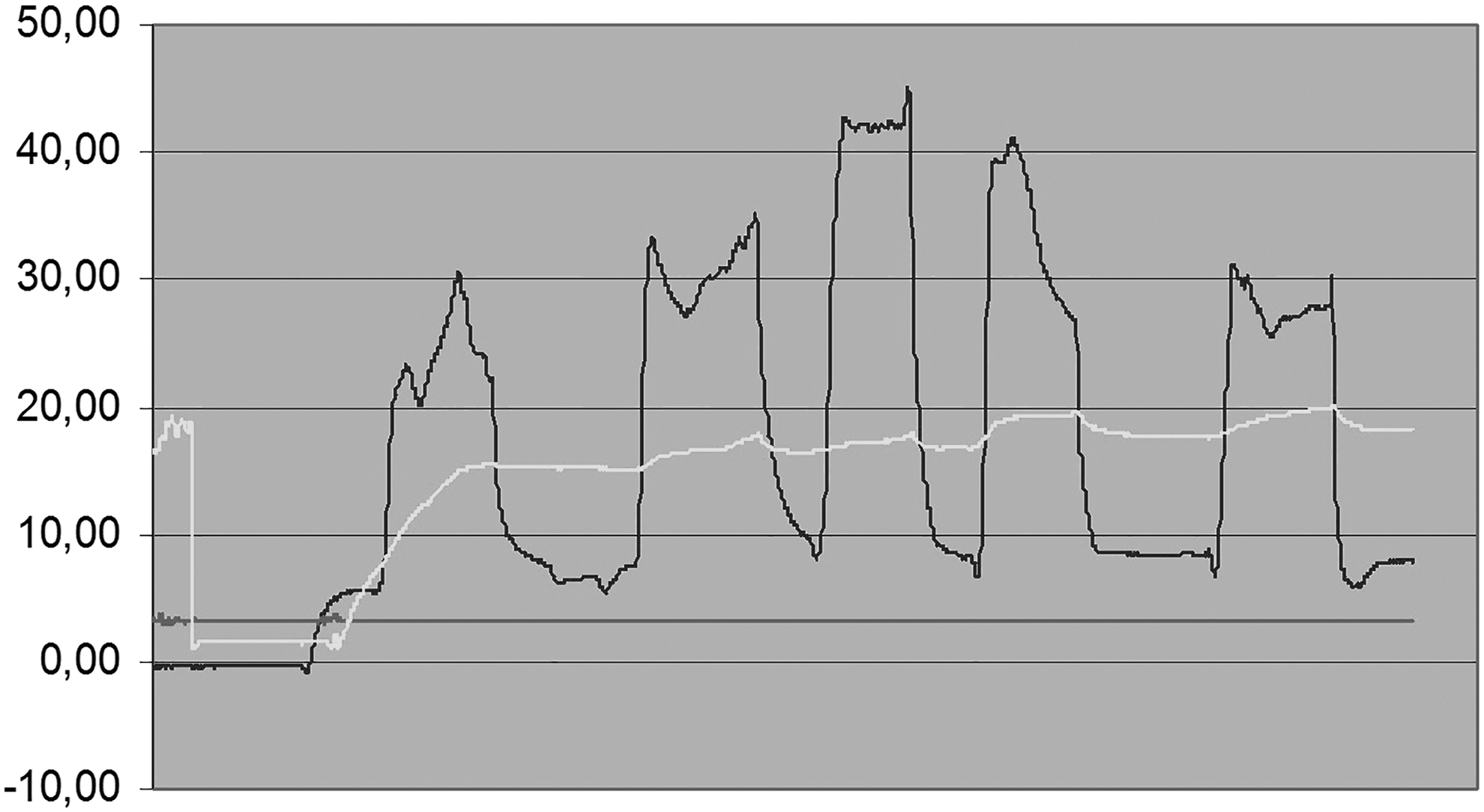
Subcutaneous tissue fluid pressures during rolling of the lymphedematous calf. Pressure on Linforoll handle ranged between 70 and 80 mmHg. Upper curve—tissue fluid pressure under the pressing roller, midline—pressure in the calf distal from the roller, lower curve—pressure in the proximal part of the calf 10 cm forward from the roller. Note that tissue fluid pressure is lower than in the pressing handle. Also, handle pressure is not transmitted to the calf proximal segments. This is due to the high tissue hydraulic resistance. High distal pressure (mid curve) points to retention of fluid in the nonmassaged regions despite relative emptying of the proximal tissues by the roller.
Continuous limb circumference measurement
A continuing process of accumulation of edema fluid proximally to the rolling device was observed (Fig. 7, adapted from Olszewski et al. 4 ).

Plethysmography of the calf during Linforoll massage. Two strain gauges placed on the calf recording increase in leg circumference. Lower curve above the ankle-roller approaching the gauge (rising curve arm) and passing it (falling curve). Sequential peaks are generated by repetition of rolling. Little edema fluid above the ankle results in lack of curve rise. Upper curve in the midcalf—rising curve as edema fluid is moved proximally toward the knee (adapted from Olszewski et al. 4 ).
ICG near-infrared lymphangiography
The ICG lymphangiography enables watching of the edema fluid flow during rolling (Fig. 8). The pre- and postrolling ICG pictures showed a decrease in fluorescence level in the massaged region (Fig. 9a, b). These changes could be followed along the calf axis (Fig. 10). The volume of fluid moved by each rolling from midcalf to below knee region ranged in our massage protocol between <1 and 3 mL. The effect of 20 consecutive rollings lasted while measured by a tonometer for at least 20 minutes. The ICG refilling of the rolled tissues from regions it was removed lasted for 15–20 minutes. Within this time period, elastic bandages were put on the limb.

The ICG imaging of calf tissues during rolling of Linforoll at 80 mmHg.

The ICG imaging of calf tissues

The ICG-stained edema fluid movement can be recorded with respect to the fluorescence level. Upper curve—before massaging and lower curve—after the standard procedure. Note evident decrease in the level of fluorescence along the calf axis.
Discussion
This study provided another portion of information on the Linforoll applied force (pressure) and generated tissue structure and tissue fluid pressures. In the present study, we measured additional parameters useful for the understanding of tissue and fluid events and useful for approval of the device for general practice. Lack of significant changes in skin stiffness, skin water concentration, surface skin temperature, and capillary blood flow, but evident increase in the subcutaneous tissue elasticity (tonometry) and lymphangiography-shown flow of edema fluid provided clear evidence of no tissue damage but effective edema fluid flow. The obtained data evidently show that not the skin but the subcutis accumulated edema fluid that can successfully be moved proximally under the pressures of 80–120 mmHg. This indicates that high rolling pressures are necessary to move fluid and are not harmful to the tissues.
Lack of changes in skin stiffness is not surprising as this is a 200–500-μm-thick structure with little extracellular water.
A slight increase in skin surface temperature is a consequence of force applied by force from Linforoll. We did not measure deep tissue temperature. There might have been some force transmitted to the subcutaneous tissue fiber network changed into heat and softened solid structures. However, that effect would be minute.
The observed decrease in skin capillary blood flow was expected. External force of more than 80 mmHg could slow down blood flow in the subdermal capillaries sensitive to external signals. It is known that massage causes at first an increase in capillary flow and an immediate fall when massage is stopped. The effect appears to be local and not centrally mediated and is related to the pressure used. 14 Treatment cools the skin for at least 15 minutes after a 45-minute massage. 15 This was also observed in our studies. The skin surface temperature went down for minutes after rolling.
Increase in deep tissue elasticity was an evident effect of Linforoll massaging. The mechanism of decreased stiffness of tissues is not clear. It may partly be due to evacuation of excess fluid and partly due to an increase in elastic and collagen fiber elasticity and slow recoil after pressing by Linforoll. Collagen bundles in the subcutis have some undulations or “crimping” when not under tensile loading. During massaging, crimping is taken out of the collagen. A new length of the collagen fiber structure is established that reflects the balance between the elastic recoil of the remaining intact collagen and the resistance of the intrinsic tissue water and glycosaminoglycans to compression. The presence of waviness or crimping in the normal collagen bundles represents a variable amount of slack. This slack must be taken out by a tensile force before any individual bundle of collagen is placed on stretch. 16 The increased softness of tissues was considered by patients as the most valuable effect.
The original externally applied force is dispersed throughout a region. Due to dissipation of the applied force in the solid structures of tissue as skin and fiber net structure of the subcutaneous tissue, the tissue fluid pressure under the moving roll turned out to be evidently lower than that at the Linforoll/skin interface. This confirmed the results of our previous studies on force dissipation using intermittent pneumatic compression.3,4
The most convincing proof of the efficacy of our Linforoll therapy was the plethysmographic recordings of edema fluid movement and the ICG lymphangiography pictures. The video showed real-time fluid distribution and fluid fluorescence flow along the limb. The level of fluorescence was quantified. Although the ICG lymphangiography shows patterns of fluid accumulation at the tissue depth of 15 mm, the decrease of fluorescence intensity may indicate there is also its decrease in deeper layers, as tissue fluid channels are an interconnected hydraulic network. 17 This is an important suggestion justifying usage of high Linforoll rolling pressure to move the subcutaneous fluid.
The proved advantages of Linforoll massaging observed in this study were evident effectiveness in moving stagnant edema fluid under high pressures encompassing the whole subcutaneous tissue (Fig. 11). Dermal tissue hydromechanic parameters remained normal proving lack of destructive changes under high massaging pressures.

The schematic presentation of the efficacy of Linforoll usage. Lack of statistically significant changes in skin water concentration, stiffness, temperature, and capillary flow, and an increase of elasticity of subcutis in deep tonometry, as well as visible fluid movement on fluorescent lymphography, indicate that high Linforoll pressure and deep compression to the muscular fascia are necessary and safe.
Taken together, the main problem in compression therapy is lack of knowledge of hydraulic events in the massaged tissue. The tissues stiffness depends on the fibrotic and fat tissue mass and mobile fluid volume. These parameters differ at different limb levels, being high above the ankle and lower in midcalf and above knee. Applied force should be adjusted to limb anatomy. To have insight into fluid movement, tonometry and direct visualization of fluid movement are necessary. Once known, they enable using effective force here and there and observe fluid flow during rolling. This is what Linforoll provides. The massaging techniques as manual, bandaging and pneumatic compression, do not give insight into tissue events, basing mainly on circumference changes.
Footnotes
Author Disclosure Statement
No competing financial interests exist.