
Abstract
Abstract
Background:
Mechanistic target of rapamycin (mTOR) inhibitors are being used off-label showing promising results in patients with vascular anomalies. Children with lymphatic malformations (LMs) involving the airway benefit from sirolimus therapy soon after birth, reducing the need of tracheostomy. Available information about efficacy and side effects in neonates remains poor. We present seven newborns with severe head and neck LM showing response to sirolimus with no significant toxicity.
Methods and Results:
We performed a retrospective review of neonates with head and neck LM who received sirolimus between January 2014 and May 2018 with upper airway involvement needing ventilatory support. We analyzed type of LM, involved anatomical area, symptoms and response to sirolimus, including dosage, blood levels, response, side effects, and complications. Seven neonates received primary treatment with sirolimus in the context of cervical LM. Sirolimus was started at the recommended dose of 0.8 mg/m2/12 h and adjusted to maintain blood levels between 4 and 12 ng/mL. Median follow-up was 32 months (4–43) with a median treatment duration of 12 months (3–43). One patient had complete resolution of the malformation, one had complete resolution of symptoms, and five had partial resolution of the malformation with significant improvement in their respiratory conditions. Two patients required additional subtotal surgical resection and one tracheostomy. Four patients remain under treatment. Toxicity was not observed.
Conclusions:
Sirolimus is a safe drug in neonates and can be considered the first therapeutical option in newborns at high risk of respiratory failure before sclerosis or surgery. Close follow-up is mandatory to identify side effects at long-term use.
Introduction
Sirolimus is a mechanistic target of rapamycin (mTOR) inhibitor that directly inhibits mTOR, blocking downstream protein synthesis of the PI3K/Akt/mTOR pathway and presenting antitumoral and antiangiogenic effect. 1 It has been mainly used to prevent organ rejection in kidney transplants as well as for coronary stents to prevent restenosis and for lymphangioleiomyomatosis. In addition, mTOR inhibitors are being used off-label and are showing promising results in the management of complex vascular anomalies. 2
Unfortunately, case reports and retrospective case series published in the literature have no standardization or criteria about dose, length of treatment, effectiveness, or toxicity in neonates. Furthermore patients and conditions are heterogeneous with optimal blood levels of sirolimus and treatment duration remaining under debate.2,3
The vast majority of vascular anomalies present in childhood, including the neonatal period, usually occur in the head and neck region. 4 Lymphatic malformations (LMs) involving the airway are difficult to manage, particularly in neonates who may need ventilator support. Current approach involves surgical excision, sclerotherapy, and even tracheostomy when extubation is not possible. These patients with LM involving the airway could benefit from sirolimus therapy soon after birth, but its use has been limited due to the potential toxicity risk in neonates. 5 Standard recommendations for sirolimus do not consider its use in newborns as pharmacodynamics parameters are not comparable to older children or adults. 6 Although clinical trials remain the gold standard for drug evaluation, children, especially neonates, have become “therapeutic orphans” of prescribed off-label drugs. 7 For that, there are no randomized studies in neonates, and information must be collected from series of cases.
In this study, we present our experience with sirolimus in neonates with head and neck LM.
Methods
Data collected
A retrospective review of neonates with LM who received treatment with sirolimus between January 2014 and May 2018 was performed. The variables analyzed included basic characteristics of patients, type of vascular anomaly, localization and symptoms, previous or later treatments, treatment with sirolimus, including dosage and blood levels, response, and complications.
Treatment
After diagnosis and evaluation by a multidisciplinary team, sirolimus treatment was proposed to reduce the need of ventilatory support. An informed consent signed by the parents was obtained. Therapy with sirolimus was initiated at the recommended dose of 0.8 mg/m2/12 h. Patients were followed up at neonatal ICU to assess evolution under therapy and appearance of any side effect.
Efficacy criteria were accepted as resolution of symptoms or reduction of size of the lesion, naked-eye or by imaging. Partial response was defined as improvement of symptoms and reduction of the lesion, but persistence of the anomaly. Complete response was defined as disappearance of symptoms and lesion, without visualization of the anomaly by imaging.
Data analysis
A descriptive analysis was performed expressing data in percentage from total and medians with their ranks. A literature review was also performed. Electronic databases (PubMed and Medline) were systematically searched for articles in English and Spanish languages referring to the use of systemic mTOR inhibitors in neonates with vascular anomalies, with the terms: “vascular anomalies,” “vascular malformations,” “mTOR inhibitors,” “Sirolimus,” “Rapamycin,” “neonates.”
Main Results
Patient characteristics
Seven neonates received treatment with sirolimus in the context of head and neck LM, three males (43%) and four females (57%). Five patients presented a common macrocystic LM, one patient a combined venous-LM, and the last one a microcystic LM in the context of a CLAPO syndrome (capillary malformation of the lower lip, lymphatic malformation of the face and neck, asymmetry of the face and limbs, and partial or generalized overgrowth).
All the malformations were located in the cervical region and floor of the mouth, with involvement of the upper airway in all of them (100%), tongue in four patients (57%) and mediastinum in two patients (28%). Intubation and mechanical ventilation were needed in three patients and unstable respiratory condition was noticed in four, needing noninvasive ventilation. Sirolimus was the first treatment in all of them.
Data on patient's characteristics are summarized in Table 1.
Patient's Characteristics
CLAPO, capillary malformation of the lower lip, lymphatic malformation of the face and neck, asymmetry of the face and limbs, and partial or generalized overgrowth.
Sirolimus treatment
The seven patients began therapy with sirolimus at the recommended dose of 0.8 mg/m2/12 h, starting at a median age of 15 days (1–32) and continued for 12 months (3–46). Therapeutic drug monitoring was performed in every patient with an accepted range between 4 and 12 ng/mL. Patients 3 and 4 had high levels at control (22 and >90 ng/mL, respectively) without secondary effects at that moment, but requiring dosage adjustments.
During the treatment, two patients had sporadic elevation of gamma-glutamyl transferase and one patient of triglycerides without need of dosage adjustment. There were no other side effects ascribed to sirolimus.
Sirolimus was withdrawn in three patients, one for complete resolution of the malformation, one for complete resolution of symptoms, and one needing surgical resection despite the reduction in size of the LM. Four patients remain under treatment at the present moment.
Outcome
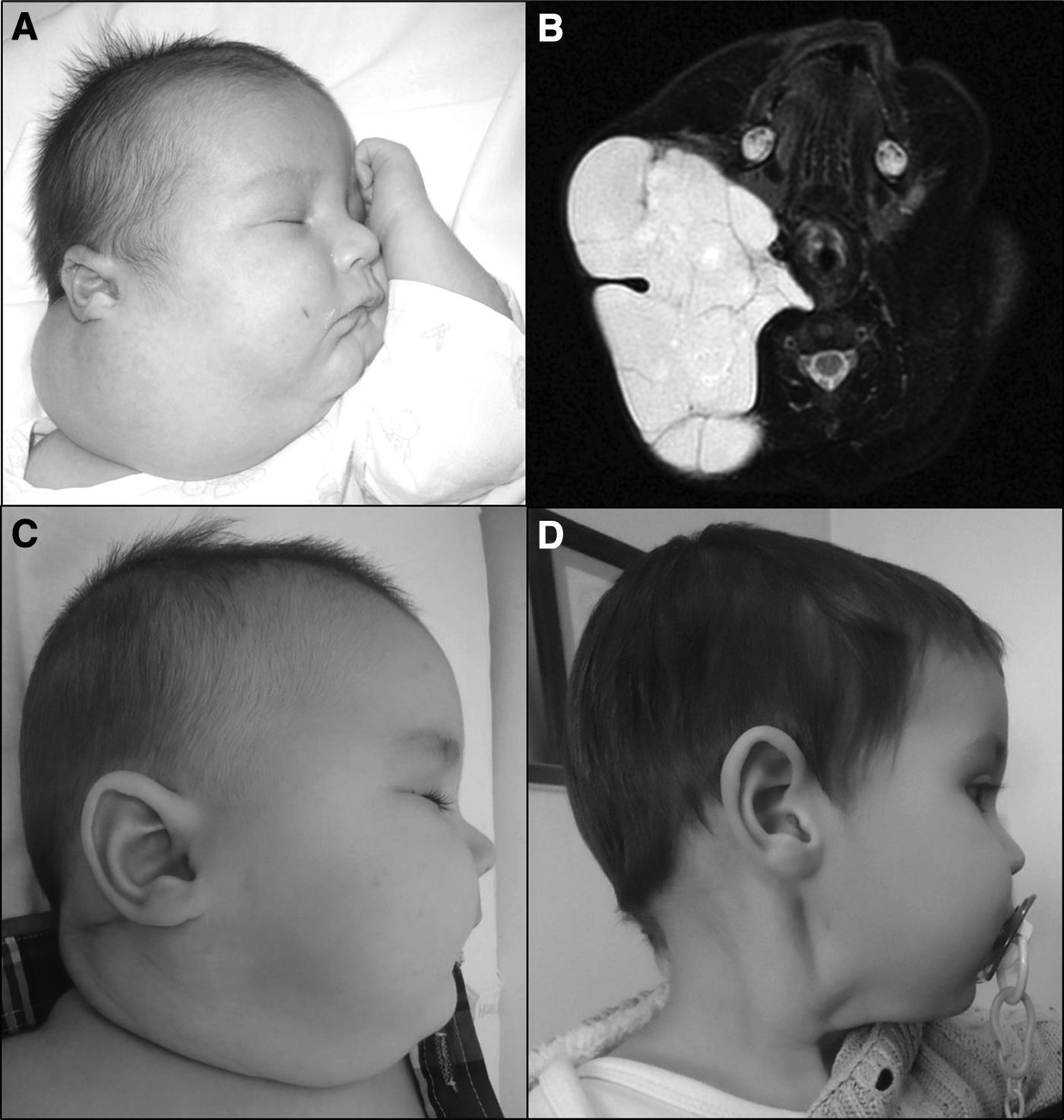
Median follow-up was 30 months (4–46) with a median duration of sirolimus treatment of 12 months (3–46). One patient had complete resolution of the malformation, one had complete resolution of symptoms, and five had partial resolution of the malformation with improvement of symptoms (Figs. 1 and 2). Patient 3 could wean off mechanical ventilation and presented reduction of the LM, but due to long hospitalization she had several respiratory infections and finally needed surgical resection and tracheostomy, although she continues under treatment with progressive reduction of the residual LM (Fig. 3). Patient 4 underwent partial surgical resection to improve symptoms, with interruption of sirolimus 2 weeks before and after the procedure. Patient 5 worsened with an episode of respiratory distress, after 5 months of treatment with partial response, and required surgical resection and radiofrequency of the tongue.
Patient 1 with large macrocystic cervicofacial LM and complete response to sirolimus.

Patient 4 with cervicofacial LM and partial response to sirolimus.

Patient 3 with massive cervicofacial LM and partial response to sirolimus.
Three of the five patients with partial resolution had at least one episode of lymphangitis due to intralesional bleeding during sirolimus treatment.
Data on patient's treatment and outcome are summarized in Table 2.
Patient's Treatment and Outcome
GGT, gamma-glutamyl transferase; LM, lymphatic malformation; TG, triglycerides.
Discussion
LMs involving upper airway are difficult to manage in symptomatic neonates needing ventilatory support, including intubation. Current therapies include surgical excision and tracheostomy if extubation is not possible. Unfortunately cranial nerve injury is a frequent complication after total or subtotal resection of massive LMs in newborns, and delayed surgical approaches are recommended when possible. Recent successful experiences with the use of sirolimus in older children lead us to consider its use in neonates in life-threatening conditions. 8
There are only a few case reports published in the literature about the use of sirolimus in neonates, mainly for hyperinsulinemic hypoglycemia with divergent outcomes. 9 In the limited group of neonates with vascular anomalies, small number of patients is the rule, with varied phenotypes, different location and extension, and simply too little information to perform a valid analysis and correlation. 5
Sirolimus dosage for vascular anomalies is commonly started at 0.8 mg/m2/12 h, based on dosage experience for prevention of graft rejection in kidney transplantation. Therapeutic range in kidney transplants recommends levels of 12 to 20 ng/mL for maintenance treatment, but for vascular anomalies, a range between 5 and 15 ng/mL is often considered sufficient. 5
However, in kidney transplantation sirolimus must maintain immunosuppression levels, but this is not necessary for vascular anomalies, in which lower doses may be enough to achieve therapeutic levels. This is similar for neonates and younger children, who will most probably need lower doses in the treatment of vascular anomalies. In fact, most authors of case reports of sirolimus in neonates start with a dose of 0.5 mg/m2/12 h, and sometimes it is reduced to even 0.2–0.3 mg/m2/12 h, while maintaining levels between 5 and 15 ng/mL. 10 Recent studies are stabilizing sirolimus doses for neonates and infants to achieve target concentration range between 5–10 and 10–15 ng/mL. In fact, in our Vascular Anomalies Unit, we now use the suggested doses by Adams et al. and start with 0.4 mg/m2/12 h before 1 month of age, increasing every month to achieve target levels between 10 and 15 ng/mL. 5
Still, we do not know which are the optimal doses and levels for each patient, and it will likely depend on the phenotype of the LM, the extension, the age of the patient, and the symptoms. We try to maintain sirolimus at standard dose and recommended target levels (10–15 ng/mL) during at least 6 months or even a year if there is improvement; and after that, we start tapering until achieving the minimal effective dose for each patient, meaning that patient remains asymptomatic at the possible lowest dose to reduce to the maximum side effects.
In contrast to the so-called rapalogs (Everolimus, Temsirolimus, and Deferolimus), sirolimus has a poor oral bioavailability due to an extensive intestinal and hepatic first pass metabolism by cytochrome P450 (CYP) 3A4. Sirolimus is mainly distributed by red blood cells and has a large volume of distribution, being eliminated via fecal/biliary pathways with a half-life of 62 hours. This long half-life allows for convenient once-daily dosing, but a loading dose is recommended to achieve target drug concentrations rapidly.11,12 These pharmacodynamics make mandatory sirolimus monitoring, even more in neonates, in which the drug-metabolizing enzyme systems are in constant development and are still poorly understood. 13
Regarding acute side effects, most of them are dose dependent and improve with dose-reduction or disappear after a few weeks from withdrawal. Most reported side effects are susceptibility to infections, impairment of wound healing, stomatitis, hypertension, hyperglycemia, dyslipemia with hypertriglyceridemia and hypercholesterolemia, and bone marrow suppression with anemia and thrombocytopenia. 14 Majority of published studies reveal a low incidence of side effects with sirolimus use, as well as in our own experience. No patient needed dose adjustment or withdrawal due to side effects.
One worrisome although infrequent side effect is Pneumocystis carinii pneumonia (PCP), reported in patients who underwent solid organ transplant and two patients with vascular anomalies treated with sirolimus. 15 This is why some authors recommend Pneumocystis prophylaxis with sulfamethoxazole-trimethoprim, while on sirolimus. None of our patient received prophylaxis and none presented with PCP. Probably higher levels of sirolimus or other concomitant medications such as corticosteroids can be a risk factor for PCP. We believe that selected patients may benefit from Pneumocystis prophylaxis while on sirolimus. There are patients who will be able to completely withdrawing sirolimus, but some patients may need a small dose for many years if not for life.
Since sirolimus treatment in vascular anomalies is very recent, long-term toxicity must be assessed from kidney transplant patients. The most common adverse effects include pneumonitis, bone marrow suppression (anemia, leukopenia, and thrombocytopenia), hyperlipidemia, new-onset diabetes, metabolic syndrome, infertility, and susceptibility to infections. 16
New-onset diabetes has become a concern in kidney recipients due to its high incidence. Acute treatment with sirolimus enhances insulin sensitivity by inhibition of the mTOR complex 1 (mTORC-1), while its chronic use produces insulin resistance by the disruption of mTORC-2 leading to hyperglycemia. 17
Other long-term issue is future subfertility or infertility in male patients treated with sirolimus. Some studies have observed lower testosterone levels, reduction in total sperm count, and decreased fathered rate in patients who received sirolimus compared to patients with sirolimus-free regimen. 18 Fortunately, these fertility effects have proved to be reversible after tapering or stopping sirolimus treatment.
Furthermore, there are several reports on transplanted women who gave birth after receiving sirolimus during the whole pregnancy and so far, all the babies have been healthy and without congenital malformations, which is a relevant data showing safety about its use in neonates. 19 In animal studies, it has been associated with increased fetal mortality, decreased fetal weights, and delayed ossification of skeletal structure, but no teratogenicity was noted. 20 Future malignancies and developmental issues have not been proved associated to long-term sirolimus therapy.
Although sirolimus has shown a beneficial effect in the management of LM in our group of neonates, without noticeable side effects, some patients may need associated treatments, such as surgical resection or sclerotherapy to improve symptoms. Multidisciplinary management remains the key for LM patients.
Conclusion
Sirolimus efficacy in the management of complex vascular anomalies has been widely reported, and it is now considered as a first therapeutical option or as a rescue treatment after surgery or endovascular procedures failure. Considering our experience and the reported data in medical literature, sirolimus is a safe drug in neonates. Despite the lack of information regarding eventual side effects at long-term use, after proven evidence of its benefits in newborns with LM at high risk of tracheostomy or death, sirolimus has to be considered as the first therapeutical option in this group of patients.
Footnotes
Author Disclosure Statement
No competing financial interests exist.