
Abstract
Background:
Patients with lymphedema, especially those having genital lymphangiectasia, experience repeated cellulitis; however, the causative bacteria are not detected in most cases. In this study, we investigated the composition of genital bacterial flora in patients with lower limb lymphedema to appropriately treat or prevent repeated cellulitis in these patients.
Methods and Results:
We examined 47 women with lower limb lymphedema. The average age was 58.4 (range 36–80) years. We performed indocyanine green (ICG) lymphography to confirm the presence of genital lymphedema. For each patient, we swab the skin in the genital area. The swabs were applied to aerobic agar plates, incubated, and evaluated to assess bacterial colonization and resistance to antibiotics. We numbered the patients who held the antibiotic-resistant bacteria, especially methicillin-resistant Staphylococcus epidermidis, methicillin-resistant Staphylococcus aureus, and extended spectrum β-lactamase-producing Enterobacteriaceae. Among the 47 patients enrolled, 30 patients (63.8%) had a history of cellulitis accompanied by lymphedema and 31 patients (66.0%) had genital lymphedema diagnosed by ICG lymphography. Among 47 patients, 43 (91.5%) had at least one bacterial strain. Coryneform bacterial species were most commonly detected in 19 patients. Of 29 patients with a history of cellulitis, 9 had antibiotic-resistant bacteria (31.0%). In contrast, of 18 patients with no history of cellulitis, only 2 had antibiotic-resistant bacteria (11.1%) (p = 0.12).
Conclusions:
The percentage of patients with drug-resistant bacteria was higher among those with a history of cellulitis than among those without it.
Introduction
Lymphedema sometimes occurs after pelvic lymph node dissection for treatment of cancer, especially uterine or ovarian cancer. Lower limb lymphedema is commonly observed, and genital lymphedema is seldom referred, although genital lymphedema is found in 60.6% of patients with lower limb lymphedema. 1 In addition, genital lymphedema is sometimes mistaken for obesity, and imaging examinations, including indocyanine green (ICG) lymphography or lymphoscintigraphy, are essential in diagnosing genital lymphedema. Acquired lymphangiectasia may develop in patients with genital lymphedema, reducing the quality of life of these patients.2–4
Patients with lymphedema, especially those also having genital lymphangiectasia, experience repeated cellulitis. 2 Patients have sudden worsening of edema in the affected limbs and high fever; however, the causative bacteria are not detected in most cases. Resident microbiota in the skin, including Staphylococcus epidermidis and coagulase-negative staphylococci (CNS), are usually harmless to the human body. However, sometimes multidrug-resistant strains of CNS, Corynebacterium species, or Acinetobacter species induce group infection in immunocompromised patients in hospitals.5–7 In those patients, the immune system is impaired by abnormal trafficking of immunocompetent cells through lymphatic channels in lymphedematous limbs. 8 Genital bacterial flora may have a relationship with repeated cellulitis in patients with lymphedema.
In this study, we investigated the composition of genital bacterial flora in patients with lower limb lymphedema. The aim of this study was to elucidate the bacterial flora in lower limb lymphedema patients to establish the appropriate treatment or preventive method for repeated cellulitis in those patients.
Patients and Methods
We examined 47 women with lower limb lymphedema who were hospitalized between June 20 and September 7, 2019. The average age was 58.4 (range 36–80) years, and the average body mass index was 22.4 (range 16.8–28.2) kg/m2. The causative disease of lymphedema was uterine cancer in 33 patients, ovarian cancer in 11, and rectal cancer in 1. Two patients had primary lymphedema. For cancer treatment, 43 patients underwent lymph node dissection, 22 underwent chemotherapy, and 12 underwent radiotherapy. The average duration of lymphedema was 7.52 (range 1–32) years. Based on the classification of the International Society of Lymphology, 31 limbs were stage 1, 22 were stage 2a, 33 were stage 2b, and 8 were stage 3.
For ICG lymphography, we injected ICG (0.05–0.1 mL) into the bilateral first web spaces, including the proximal side of the external condyle and the lateral side of the distal thigh. Lymphatic flow was observed using an infrared camera (Photodynamic Eye; Hamamatsu Photonics, Shizuoka, Japan) at least 2 hours after the injection.9–11 We recorded the presence of dermal backflow into the genital area, which indicated abnormal lymphatic function or accumulation of lymphatic fluid (Fig. 1).
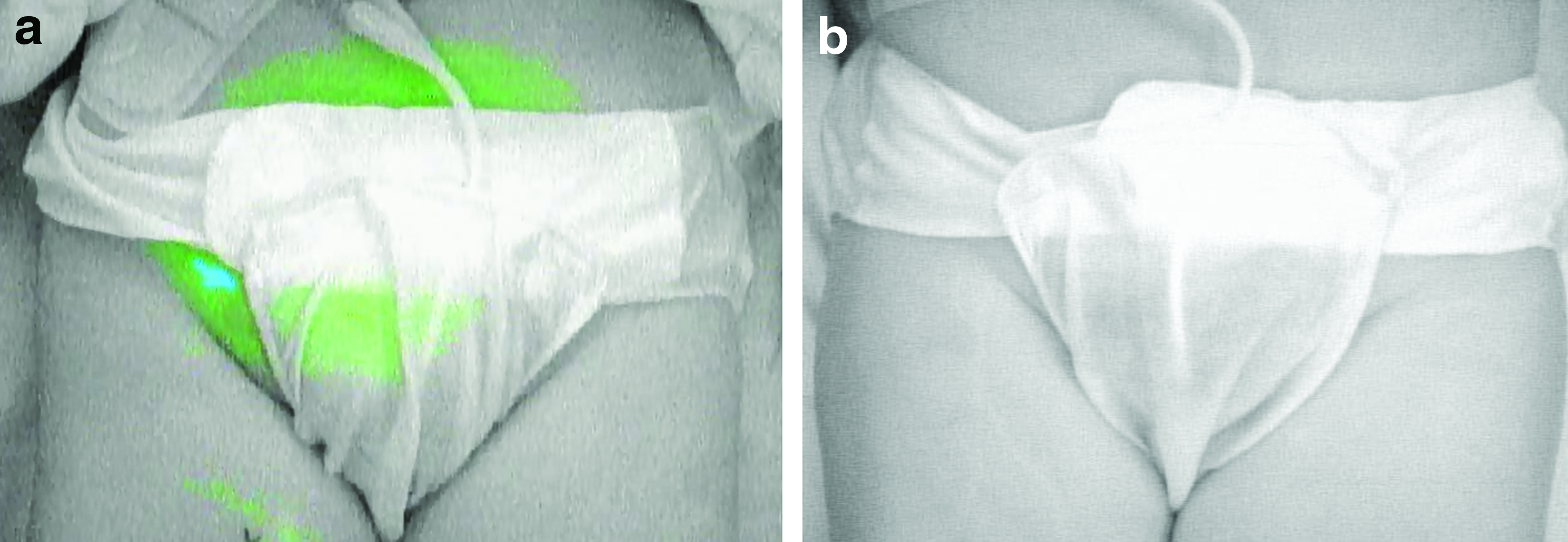
ICG lymphographic findings of the genital area.
For each patient, a single culture sample was obtained through a sterilized swab of the skin in the genital area. The swabs were applied to aerobic agar plates, incubated in an aerobic atmosphere at 35°C, and then evaluated to assess bacterial colonization and resistance to antibiotics by clinical microbiology. Bacterial strains and drug sensitivity were identified using the MicroScan WalkAway 40 (Beckman Coulter Science Japan, Tokyo, Japan). We numbered the patients who held the antibiotic-resistant bacteria, especially methicillin-resistant S. epidermidis, methicillin-resistant Staphylococcus aureus, and extended spectrum β-lactamase (ESBL)-producing Enterobacteriaceae, which often become problematic in the hospitals.
We also investigate the frequency of cellulitis in the patients with defining cellulitis as an inflammation in the affected limbs with >38.5°C fever.
Statistical analysis was performed using the χ2 test with a significance level of 0.05.
This study was approved by the institutional ethical committee, and written consent was obtained from each patient (approval no. H30-8).
Results
Among the 47 patients enrolled, 30 patients (63.8%) had a history of cellulitis accompanied by lymphedema. Thirty-one patients (66.0%) had genital lymphedema diagnosed by ICG lymphography, and four patients had genital acquired lymphangiectasia (Fig. 2). Among 31 patients with genital lymphedema, 20 patients (64.5%) had the history of cellulitis (Fig. 3). Two patients experienced cellulitis >20 times, 4 patients experienced 5–10 times, and 12 patients experienced 1–4 times (frequency was unknown in 3 patients). In most cases, genital region was involved in the cellulitis affected area. In contrast, among 16 patients without genital lymphedema, 9 patients (56.3%) had the history of cellulitis. Seven patients experienced cellulitis one to five times (frequency was unknown in two patients).

Clinical appearance of genital lymphedema and GAL. The purple spindle-shaped lines are the design for resection of GALs. GAL, genital acquired lymphangiectasia. Color images are available online.

Relationship between the presence or absence of genital lymphedema (horizontal axis) and the percentage of having the history of cellulitis (vertical axis).
Among 47 patients, 43 (91.5%) had at least one bacterial strain. Coryneform bacterial species were most commonly detected in 19 patients. Enterococcus faecalis, S. epidermidis, coagulase-negative Staphylococcus species, viridans streptococci, Escherichia coli, and S. aureus were also found (Table 1). Among patients without genital lymphedema, antibiotic-resistant bacteria (methicillin-resistant S. epidermidis) were detected in two patients (12.5%) (Table 2). Among patients with genital lymphedema, antibiotic-resistant bacteria, including ESBL-producing Enterobacteriaceae or methicillin-resistant S. aureus, were found in nine patients (29.0%). The percentage of patients harboring drug-resistant bacteria was high among patients with genital lymphedema, although the difference was not significant (p = 0.20).
List of Bacteria Stains Found in the Genital Area of Patients with Lower Limb Lymphedema
Coryneform bacterial species were found in most cases.
List of Antibiotic-Resistant Bacterial Strains Found in the Genital Area of Patients with Lower Limb Lymphedema
ESBL, extended spectrum β-lactamase.
Of four patients with genital acquired lymphangiectasia, three had a history of cellulitis and three had antibiotic-resistant bacteria.
Of 29 patients with a history of cellulitis, 9 had antibiotic-resistant bacteria (31.0%) (Fig. 4). In contrast, of 18 patients with no history of cellulitis, only 2 had antibiotic-resistant bacteria (11.1%). The difference was not significant (p = 0.12).

Relationship between the history of cellulitis (horizontal axis) and the percentage of patients with antibiotic-resistant bacteria (vertical axis). Patients with a history of cellulitis had a higher percentage of harboring antibiotic-resistant bacteria.
Discussion
In this study, we investigated the bacterial flora of the genital area in patients with lower limb lymphedema. This is the first report to reveal that 23.4% of patients with lower limb lymphedema had drug-resistant genital flora. The percentage of the population harboring drug-resistant bacteria was higher among patients with a history of cellulitis than among those without. Patients with lymphedema sometimes experienced repeated cellulitis and were prescribed antibiotics multiple times, possibly affecting the high percentage of patients with drug-resistant bacteria.
Causative bacteria are not usually detected in cellulitis accompanied with lymphedema, although blood culture is performed. Therefore, selecting appropriate antibiotics is difficult for such cases. Olszewski reported that administration of penicillin reduced the frequency of cellulitis in patients with lymphedema-affected limbs. 12 The results of this study indicate that approximately one quarter of patients with lymphedema harbor drug-resistant bacteria, and physicians should keep this under advisement when formulating treatment regimens. Moreover, it is important to practice standard precautions, including hand hygiene and glove use, to prevent group infection in hospitals.
Resident flora in the skin are usually harmless to the human body. However, lymphedema-affected limbs are immunodeficient because of a lack of adequate immunocyte transfer through the lymphatic vessels.8,13 This leads to frequent cellulitis or even angiosarcoma in the affected limbs. 13
Some patients with genital lymphedema also have genital acquired lymphangiectasia and experience increased cellulitis.1,2 This may be caused by thinning epidermis in the acquired lymphangiectasia, which is prone to injury, thus allowing bacterial infiltration into the edematous tissue. Sometimes, it occurs that the point of bacterial entry and the infection site is different, as seen in infectious endocarditis. Therefore, it is thought that most cases of cellulitis begin in the affected limb first, even when the patient has genital lymphedema. 14 In addition, increased lymphocyte populations present in the dermis around the acquired lymphangiectasia are proinflammatory. 2 Lymphaticovenous anastomosis can reduce the frequency of cellulitis by reducing the amount of lymphatic accumulation and lymphocyte stasis in the subcutaneous tissues.9,15–17
In conclusion, 23.4% of patients with lower limb lymphedema had drug-resistant bacteria in their genitals. The percentage of patients with drug-resistant bacteria was higher among those with a history of cellulitis than among those without it. Furthermore, the percentage was higher among patients with genital lymphedema than among those without it. We suggest that the frequency of prescribing antibiotics be reduced to avoid producing the drug-resistant bacteria, and prevention of cellulitis with complete decongestive therapy or reconstructive surgery should be recommended.
Footnotes
Author Disclosure Statement
No competing financial interests exist.