
Abstract
Background:
The skin's condition is altered in lymphedema patients, and evaluating this change is important. Some noninvasive methods for evaluating skin condition have been reported, especially in upper limb lymphedema. However, evaluating the skin in lower limb lymphedema remains challenging and is often limited to palpation. We aimed to develop a noninvasive skin evaluation method for lower limb lymphedema patients.
Methods and Results:
Twenty-five lower limb lymphedema patients were included. Skin induration and elasticity were measured using Indentometer® IDM 400 and Cutometer® MPA580. The relationship between the properties of skin from the healthy forearm and thigh, those of the affected thigh, and age was analyzed. Predicted skin induration age (IA) and elasticity age (EA) were calculated from the forearm, whereas actual values were calculated from the thigh, and the differences (ΔIA and ΔEA) were assessed. Patients were classified according to the International Society of Lymphology clinical staging system, and the differences in ΔIA and ΔEA were analyzed among the three groups (healthy, stage I/IIa, and stage IIb/III). Skin biopsy was performed in five unilateral lower limb lymphedema patients, and the dermal elastic fiber area was determined using microscopy with Elastica van Gieson staining. ΔEA significantly increased with disease progression, but ΔIA did not change significantly. Microscopy revealed elastic fiber filamentous changes, with decreased elastic fiber areas in lymphedema-affected skin.
Conclusion:
To our knowledge, this is the first report to evaluate lower limb skin elasticity in lymphedema quantitatively and noninvasively. ΔEA is useful for evaluating skin condition progression in lymphedema patients.
Introduction
Lymphedema occurs due to the insufficiency of lymph transport, causing swelling and cellulitis, and significantly lowering quality of life (QOL). 1 Over 14 million patients worldwide suffer from the advanced form of leg lymphedema, known as elephantiasis.2,3 Dysfunction of lymph transport is caused by various pathological conditions, such as hypoplasia of lymphatic vessels, cancer surgery, radiation therapy, trauma, or lymphatic filariasis.4–6 Lymph stasis due to the insufficiency of lymphatic transport produces an accumulation of lymphatic fluid, which contains proteins and cellular metabolites such as glycosaminoglycans,7–9 and causes chronic inflammation. Chronic inflammation often causes tissue fibrosis. 10 In lymphedema patients, skin induration increases with fibrosis, and skin elasticity decreases with the fragmentation and degeneration of elastic fibers due to chronic inflamation.11,12
Various methods have been developed to evaluate the progression or staging of lymphedema, of which the most commonly used is the International Society of Lymphology (ISL) clinical staging system. 13 Circumferential measurements, the water displacement method, or infrared optoelectronic limb volumetry are performed to evaluate limb edema.14–16 Lymphatic scintigraphy, 17 indocyanine green (ICG) fluorescence lymphography,18,19 or magnetic resonance lymphography 20 are often performed to evaluate lymphatic circulation. However, the skin condition in lymphedema patients is often evaluated only by palpation.
Evaluating the skin condition in lymphedema patients precisely, quantitatively, and noninvasively is challenging. Recently, some noninvasive evaluation methods, such as durometry or skin elastometry, have been suggested for the evaluation of skin diseases.21,22 However, a standard method for evaluation of the skin condition in lower limb lymphedema has yet to be established. We hypothesized that both durometry and skin elastometry would be useful. Therefore, this study aimed to develop a noninvasive and precise method for evaluating the skin in lower limb lymphedema patients.
Materials and Methods
This study consisted of two parts. The first part evaluated skin induration and elasticity. In the second part, skin tissue samples were obtained from patients with lymphedema and the elastic fibers in the lymphedema skin were evaluated histologically using microscopy.
Patients
From September 2016 to September 2018, 25 lymphedema patients were enrolled. Before the beginning of this study, all patients were diagnosed with primary or secondary lymphedema of the lower limb with both lymphatic scintigraphy 17 and ICG fluorescence lymphography 18 at the Division of Vascular Surgery, Hamamatsu University School of Medicine. The exclusion criteria were as follows: upper limb lymphedema; collagen disease; or lower limb disease other than lymphedema such as deep vein thrombosis, stasis dermatitis, atherosclerosis, or cellulitis. Unilateral lymphedema was only diagnosed when the lymphatic fluid transport was normal and no findings of dermal backflow in the contralateral limb were observed on lymphoscintigraphy 17 and ICG lymphography.18,19
Data on each patient's demographics (age, sex), body mass index (BMI), etiology of lymphedema (primary or secondary), and side of lymphedema (unilateral or bilateral) were recorded. Age and BMI are shown as average and standard deviation (SD). Clinical lymphedema staging was performed according to the ISL staging system. 23 In the 25 lymphedema patients, the 50 lower limbs were divided into three groups: healthy, ISL stage I or IIa (stage I/IIa), and ISL stage IIb or III (stage IIb/III) groups.
Skin biopsies were performed on five patients using a 5-mm dermal punch (Dermapunch; Maruho, Osaka, Japan) on both thighs under local anesthesia. The skin samples comprised the epidermis, dermis, and upper subcutaneous layers. The samples were immersed in 10% neutral buffered formalin for at least 24 hours for microscopy.
Evaluation of skin induration and elasticity
Temperature was maintained at 25°C during the measurements. Skin induration was evaluated by the Indentometer® IDM 400 (Courage+Khazaka Electronic GmbH, Cologne, Germany) (Fig. 1A). After placing the probe on the skin, the device measures how much the pin-shaped indentometer probe displaces the skin. The penetration depth is measured, ranging from 0 to 3 mm. The harder the skin, the less deep the displacement by the probe.
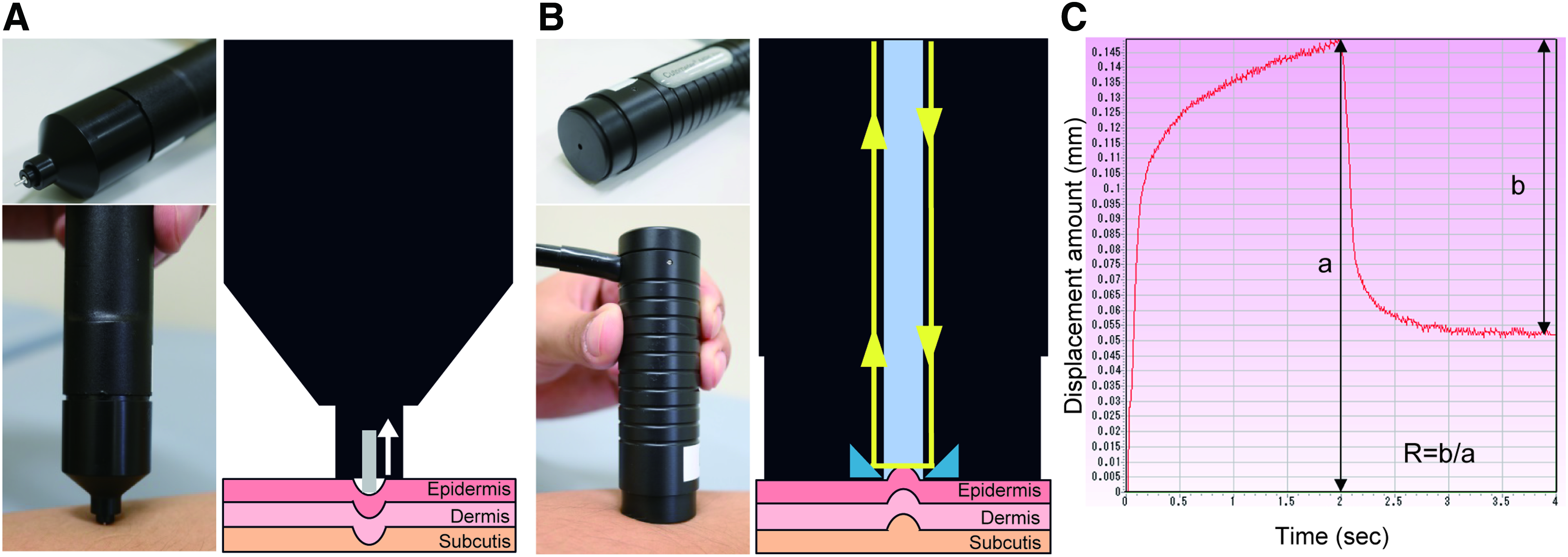
Measurement principle of Indentometer and Cutometer.
Skin elasticity was measured using the Cutometer® MPA580 (Courage+Khazaka Electronic GmbH) (Fig. 1B). 22 Negative air pressure is created for 2 seconds in the device, and the skin is drawn into the probe from 0 to 2 seconds and released again from 2 to 4 seconds. Inside the probe, the penetration depth is determined by a noncontact optical measuring system. The light intensity varies due to the penetration depth of the skin. The ability to return into its original position is presented as curves (Fig. 1C). From these curves, the penetration depths at 2 seconds (“a” in Fig. 1C) and at 4 seconds (“b” in Fig. 1C) are obtained. The Cutometer R value is calculated (R = b/a), which represents the skin elasticity. 24 The less elastic the skin, the lower the R value.
Each probe was placed on the skin of the forearm or thigh at four points: anterior, posterior, medial, and lateral. The average Indentometer or Cutometer values at four points in the thigh and eight points in the bilateral forearms were calculated.
Calculation of skin induration and elasticity age
Skin induration and elasticity are influenced by aging.22,25 To evaluate the effects of lymphedema on skin condition, it is necessary to eliminate the influence of age. We calculated the predicted and actual induration or elasticity age and then calculated the difference between them.
First, scatter plots were obtained between the Indentometer values of the forearms (I-fo) and healthy thighs (hI-th) (Fig. 2A) and the Cutometer R values of the forearms (C-fo) and healthy thighs (hC-th) (Fig. 2B). From these scatter plots, the following approximation equations were obtained:
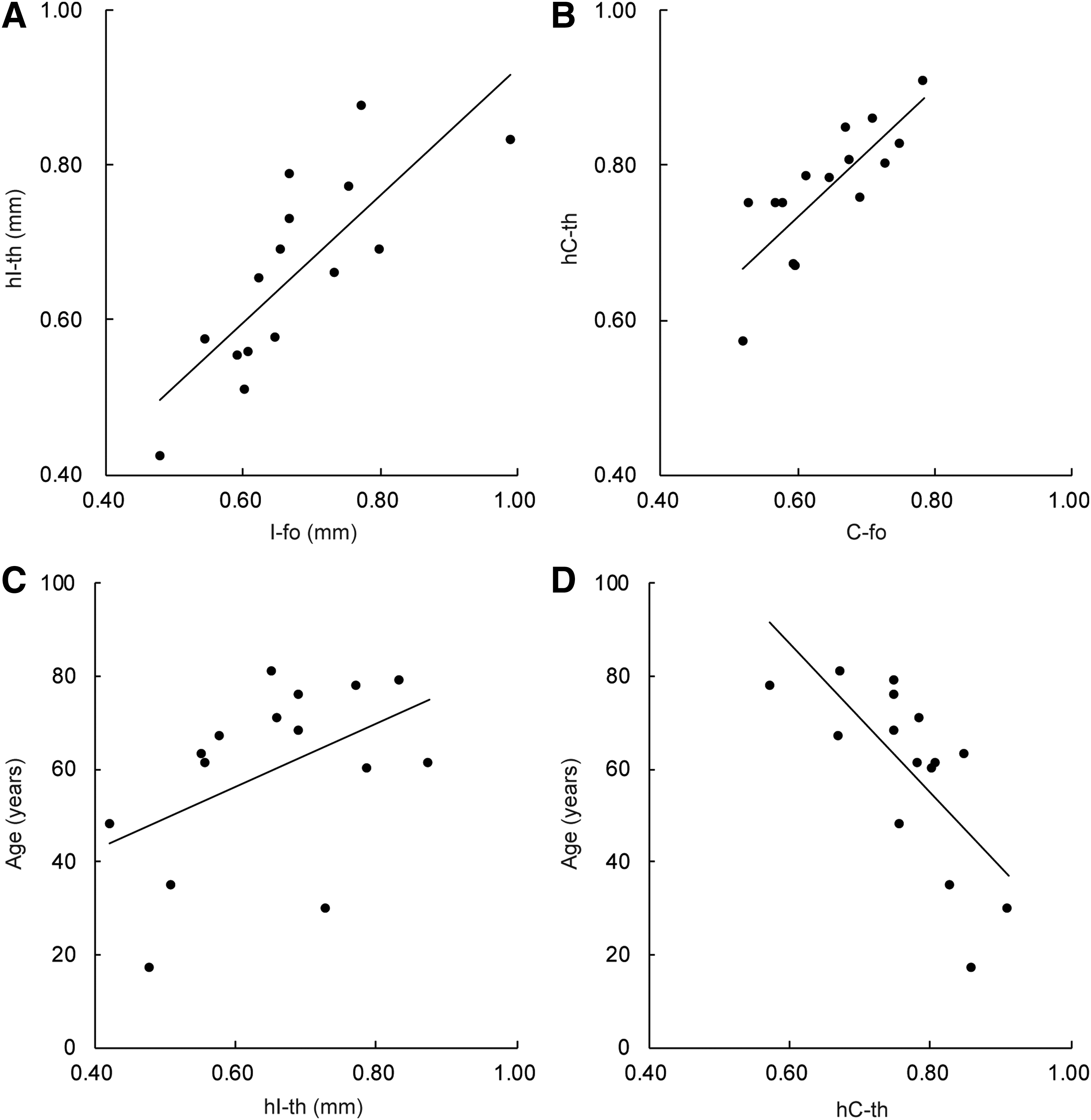
Relationships between the Indentometer or cutometer value and age.
Using these approximation equations, the predicted Indentometer and Cutometer R values of the thigh (pI-th and pC-th, respectively) in lymphedema-affected limbs were calculated from values of I-fo and C-fo.
Second, scatter plots of hI-th and age (Fig. 2C), and hC-th and age (Fig. 2D) were obtained in healthy limbs. From these scatter plots, the following approximation equations were obtained:
Using these approximation equations and predicted values (pI-th and pC-th), the predicted skin induration age (pIA) and predicted skin elasticity age (pEA) were calculated.
The actual Indentometer values (aI-th) and Cutometer R parameters of the thigh (aC-th) in lymphedema-affected limbs were measured, and the actual skin induration age (a-IA) and skin elasticity age (a-EA) were calculated using the above-mentioned approximation equations, as follows:
Third, the differences between actual and predicted skin induration age (ΔIA) and elastic age (ΔEA) were calculated.
ΔIA and ΔEA represent the effect of lymphedema after excluding the influence of age.22,26 The values of a-Ith, ΔIA, a-Cth, and ΔEA are shown as median and interquartile range. The calculation method is summarized in Figure 3.
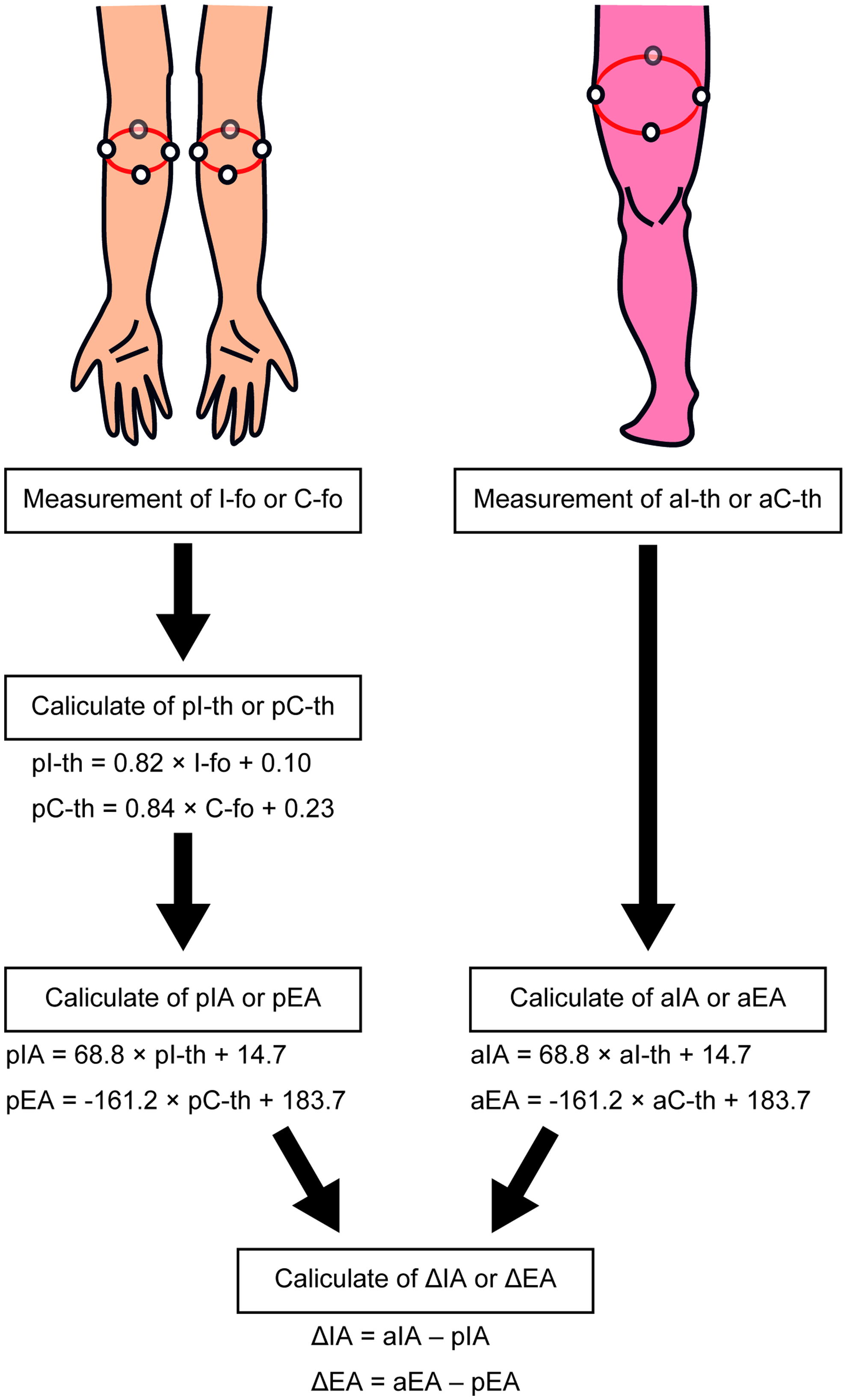
Schema of the Indentometer or Cutometer value calculation process. Calculation of predicted skin induration age (pIA) or elasticity age (pEA) at the thigh is shown on the left side and that of actual skin induration age (aIA) or elasticity age (aEA) is shown on the right side. Finally, the difference in skin induration age (ΔIA) or elasticity age (ΔEA) was calculated. Color images are available online.
Histopathological examination
Skin biopsies were obtained from both thighs of five patients. Fixed skin samples were embedded in paraffin, cut into 4-μm sections, and mounted onto Matsunami Adhesive Silane-coated slides (Matsunami, Osaka, Japan). The sections were deparaffinized in xylene, rehydrated in graded ethanol solutions, and subjected to routine Elastica van Gieson (EVG) staining using standard procedures.
Computerized image analysis for quantifying the area occupied by elastic fibers 27 was performed by light microscopy (Eclipse 80i; Nikon Instruments, Inc., Melville, NY) with a microscopic camera system (DS-U2; Nikon Instruments, Inc.). Ten view fields in the dermis and upper subcutaneous layers were randomly selected for each sample under high magnification ( × 400). The epidermis was not part of the selected view fields. The elastic fiber area was determined automatically using a computerized image analysis system (Lumina Vision version 3.0; Mitani Corp., Tokyo, Japan). Each view field area contained 33,627 μm2, and the area fractions of elastic fibers were calculated and represented as mean and SD.
Statistical analyses
The correlations of each scatter plot, between I-fo and h-Ith, C-fo and hC-th, h-Ith and age, and hC-th and age, were evaluated using Spearman's correlation coefficient analysis. A correlation was defined as high when r > 0.7 or r < −0.7 and low when r > 0.4 or r < −0.4. The differences in aI-th, ΔIA, aC-th, and ΔEA values among each group (healthy, stage I/IIa, and stage IIb/III groups) were assessed using the Kruskal–Wallis test and post hoc multiple comparisons. In the five patients who underwent a skin biopsy, normality was assessed by the Shapiro–Wilk normality tests, and statistical differences in area fractions of elastic fibers and EA between healthy and lymphedema limbs were analyzed by a paired t-test (two-sided). Statistical significance was defined as a p-value of <0.05. All statistical analyses were performed using SPSS 25.0 for Windows (SPSS, Inc., Chicago, IL).
Study approval
All procedures were approved by the Hamamatsu University School of Medicine Ethics Committee of Clinical Research (Approval Nos. 16-054 and R14-033) and were in accordance with the Helsinki Declaration of 1975 as revised in 2008. This study is registered with UMIN Clinical Trials Registry (ID: 000032413). Written informed consent from each patient was obtained before the study. Written informed consent for the use of the skin samples was also obtained from each patient before skin biopsy.
Results
Patients and limbs
Twenty-five lymphedema patients were enrolled in this study (Table 1). The 50 upper limbs were all classified as healthy and the 50 lower limbs were staged according to the ISL clinical staging system: 15 as healthy, 14 as stage I, 13 as stage IIa, 6 as stage IIb, and 2 as stage III. There were no stage 0 patients in this study. These were then classified into three groups: 15 as healthy, 27 as stage I/IIa, and 8 as stage IIb/III.
Patient Characteristics
BMI, body mass index.
Correlations between Indentometer or Cutometer R values and age
Scatter plots were obtained between I-fo and hI-th (Fig. 2A), C-fo and hC-th (Fig. 2B), hI-th and age (Fig. 2C), and hC-th and age (Fig. 2D) according to the measurements of the healthy forearms and thighs. A highly significant correlation was observed in comparisons between I-fo and hI-th (r = 0.793), C-fo and hC-th (r = 0.797), and hC-th and age (r = −0.710). A less significant correlation was observed in comparisons between hI-th and age (r = 0.481).
Comparison of skin induration and elasticity in each group
The aI-th was 0.66 (0.56–0.75) in the healthy group, 0.68 (0.62–0.74) in the stage I/IIa group, and 0.75 (0.72–0.79) in the stage IIb/III group, with no significant difference among the groups (p = 0.152, Fig. 4A). aC-th tended to decrease with the progression of the lymphedema stage [healthy: 0.78 (0.75–0.82), stage I/IIa: 0.76 (0.68–0.79), stage IIb/III: 0.69 (0.66–0.71)], and a significant difference was observed (p = 0.028) (post hoc, healthy and stage IIb/III, p = 0.023, Fig. 4B).

Comparison of values of Indentometer or Cutometer among lymphedema patients. Comparison of
The ΔIA was −2.87 years (−4.61 to 3.66 years) in the healthy group, 0.17 years (−4.50 to 3.03 years) in the stage I/IIa group, and 6.53 years (2.46–8.54 years) in the stage IIb/III group, with no significant difference among the groups (p = 0.073, Fig. 4C). ΔEA tended to increase with the progression of lymphedema [healthy: −1.69 years (−5.89 to 7.56), stage I/IIa: 5.13 years (1.20 to 14.77), stage IIb/III: 15.14 years (6.95 to 22.48)], and a significant difference was observed among the groups (p = 0.012) (post hoc, healthy and stage IIb/III, p = 0.011, Fig. 4D).
Histological evaluation of elastic fibers in lymphedema skin
Skin samples were obtained from five patients with unilateral leg lymphedema staged as IIa or IIb (mean age: 74.8 ± 6.6 years, disease duration: 22.4 ± 6.6 years). EVG staining revealed a decrease in elastic fibers in the dermis and upper layer of the subcutaneous tissues of lymphedema-affected limbs (Fig. 5A). The area fraction of elastic fibers was 6.2% ± 2.0% in the healthy group and 4.9% ± 1.3% in the lymphedema group, demonstrating a significant difference (p = 0.028, Fig. 5B, C). The average EA in the five patients was 69.0 ± 17.5 in the healthy limb and 80.5 ± 12.4 in the lymphedema-affected limb, which was a significant difference (p = 0.019).

Histological evaluation of elastic fibers in lymphedema patients.
Conclusions
We developed a method for evaluating the condition of lower limb skin in lymphedema patients using the Cutometer. The ΔEA increases about 5 years in stage I or IIa and over 10 years in stage IIb or III lymphedema patients. Calculation of ΔEA is useful as a novel, objective, quantitative measurement of skin condition in lymphedema patients.
Following the dysfunction of lymph transport, edema and skin condition changes are observed in lymphedema-affected limbs. These changes influence patients' QOL. Therefore, it is necessary to evaluate the clinical symptoms, lymphatic circulation, limb edema, and skin condition in the staging of lymphedema progression. Several methods have been developed for the evaluation of lymphedema patients in the diagnosis, treatment assessment, or follow-up stages. 13 These include measurement of limb volume by water displacement or perimetry, oil contrast lymphography, lymphatic scintigraphy, 17 ICG fluorescence lymphography, 18 magnetic resonance lymphography, 20 ultrasonography, and clinical staging scales. 13 However, methods of skin condition evaluation in lymphedema patients are still lacking.
Recently, some noninvasive evaluation methods for skin condition have been reported, such as the Cutometer for skin elasticity,28–30 the durometer or tissue compliance measurement for skin fibrosis,21,31 the Corneometer for skin hydration, 30 and impedance spectroscopy for edema. 32 The usefulness of the Cutometer has been reported in patients with scleroderma and breast cancer-related upper limb lymphedema.28–30 Killaars et al. reported a significant difference in skin elasticity between the skin of the lymphedema-affected upper limb compared with the healthy contralateral upper limb. 30 However, it is difficult to evaluate skin elasticity in patients with lower limb lymphedema using this approach. Since lower limb lymphedema is often congenital or related to pelvic cancer surgery, it is common for lower limb lymphedema to develop bilaterally. 5 Therefore, comparing legs as an approach to evaluating skin condition is difficult in patients with lower limb lymphedema. Moreover, given the influence of aging and skin region on skin elasticity,22,33 developing an evaluation method that is not influenced by age and is appropriate for bilateral lower limb lymphedema is crucial.
We hypothesized that measuring skin elasticity at the thigh for the lower limb lymphedema patients, since secondary lower limb lymphedema usually develops from the thigh to more distal regions, 19 and hC-th was most correlated with C-fo and age compared with other regions (calf or ankle) in our study (data not shown), would be clinically useful. We found a significant correlation in Cutometer R values between the normal forearm and normal thigh, and between age and the normal thigh. A significant increase in ΔEA was found with lymphedema progression. All patients with primary lymphedema in this study showed involvement of the thigh. Therefore, we believe that evaluation of the thigh was reasonable in this particular patient population. However, unlike secondary lower limb lymphedema, primary lower limb lymphedema does not necessarily develop from the thigh. Therefore, our method might not be applicable to the evaluation of skin condition in patients with primary lymphedema without involvement of the thigh.
In lymphedema-affected skin, fragmentation and degeneration of elastic fibers are observed.11,12,34 Changes of the elastic fibers to filamentous components are typical findings in lymphedema-affected skin. 11 Similar to previous studies,35,36 elastic fibers were observed to have changed to filamentous tissue in the skin of lymphedema patients in this study. Tropoelastin and microfibrils are the main structural components of elastic fibres.35,36 Regular arrangements of microfibrils and deposition of tropoelastin to the microfibril bundles are needed for the synthesis of these fibres. 36 In lymphedema-affected skin, the arrangement of the extracellular matrix becomes irregular, 11 which may influence the synthesis of elastic fibers. However, the pathophysiology of fragmentation and degeneration of elastic fibers remains unclear.
Pathological increase of collagen fibers is also observed, and transforming growth factor B1 (TGFB1) plays a central role in this pathological increase involved in skin fibrosis.37,38 Moreover, TGFB1 plays an important role in the degeneration of elastic fibers with the upregulation of matrix metalloproteinases-2 and -9 39 in the pathogenesis of Marfan syndrome.40,41 Increased TGFB1 may also influence the fragmentation and degeneration of elastic fibers in lymphedema-affected skin. Further investigation is needed to elucidate the pathophysiology of fragmentation and degeneration of elastic fibers in lymphedema patients.
Skin fibrosis has been observed in lymphedema-affected skin. 5 However, the usefulness of the Indentometer for skin evaluation in lower limb lymphedema was not observed in this study. The measurement principle of Indentometer resembles that of a durometer or a tissue compliance meter, and the usefulness of both in the evaluation of skin induration21,31 and muscle stiffness in the calf has been previously reported. 42 However, Moloney et al. reported that quantifying fibrosis with the tissue compliance meter was difficult and that there is no preferred methodology for the evaluation of neck skin fibrosis. 43 The usefulness of a durometer or tissue compliance meter in the evaluation of skin induration is controversial.
The harder the skin, the lower the Indentometer value is; therefore, we hypothesized that aI-th would decrease with disease progression. However, the opposite result was obtained in our study (i.e., there was a trend for aI-th to increase with the progression of lymphedema). Skin induration is often observed in the crus in lymphedema patients, and the ISL stage is often classified as IIb or III in the presence of crural skin induration. However, there was a lower correlation between I-fo and Indentometer values in the crus, and it is difficult to calculate skin induration age in the crus (data not shown). Therefore, aI-th may not be representative of skin induration in lymphedema patients. Further studies are needed to develop a noninvasive evaluation method for skin fibrosis in lymphedema patients.
Recently, several new therapies for lymphedema have been developed. Previously, complex decongestive therapy consisting of skin care, manual lymphatic drainage, compression bandages, or stockings was the only treatment available. The recent development of surgical treatments, 44 such as lymphatic venous anastomoses, lymph node transplantation, 45 or liposuction, has been remarkable. 13 However, the usefulness of these new therapies is controversial. Calculation of ΔEA can be useful as a novel, objective, quantitative marker of treatment effectiveness.
This study has some limitations. First, the sample size was small and was mainly composed of female patients with stage I/IIa secondary lymphedema. Second, skin biopsy was performed only in stage IIa or IIb lymphedema patients, and it was difficult to obtain informed consent for biopsies. Third, the Indentometer and Cutometer measurements were only performed in Japanese persons; consequently, the data are only representative of Japanese patients.
In summary, we developed a skin elasticity evaluation method for lower limb lymphedema patients using a Cutometer. Our findings revealed an increase in ΔEA with lymphedema progression. Calculation of ΔEA might be useful for the evaluation of skin condition progression in lymphedema patients. Further studies with larger sample sizes may help improve the accuracy of ΔEA calculation.
Footnotes
Acknowledgment
This work was supported by JSPS KAKENHI (grant number 15K21052, awarded to M.S.).
Author Disclosure Statement
No competing financial interests exist.