
Abstract
Background:
Knowledge of functional parameters that can be used for evaluation of upper extremity lymphatic function is limited. This study aims to evaluate near-infrared fluorescence (NIRF) imaging for evaluation of lymphatic function in the human arm.
Methods and Results:
Ten healthy male volunteers (age 25.7 ± 1.3 years) were included and examined at two occasions. The lymphatic functional frequency and velocity were examined at baseline, during hyperthermia and after exercise. In addition, the maximum pressure generated by contraction of the lymphatic vessels was estimated. The mean contraction frequency was found to be 0.9 ± 0.4/min, and the mean velocity of the propulsions was 1.1 ± 0.3 cm/s. The average maximal pressure generated by the contraction of the lymphatic vessels was 59 ± 12 mmHg. No significant difference in frequency, velocity, or pumping pressure was found between the two visits (p > 0.05). Local hyperthermia increased contraction frequency significantly, whereas exercise decreased frequency and increased propulsion velocity.
Conclusions:
The functional lymphatic parameters evaluated by NIRF imaging showed good repeatability with no significant difference between visits. Future examinations should be conducted with standardization of temperature and exercise, as these parameters were shown to alter lymphatic function.
Introduction
During the past decade, primary and secondary diseases of the lymphatic system have seen a marked rise in interest. Every year an estimated 1.4 million women are diagnosed with breast cancer worldwide. 1 Depending on the treatment received, the risk of acquiring lymphedema as a complication spans from 5.6% among the patients who undergo treatment with sentinel lymph node biopsy to 19.9% among patients who undergo treatment with axillary lymph node dissection. 2 Unfortunately, the treatment options for lymphedema are limited3–7 as research in the field has been neglected owing primarily to difficulties in methods of examination and lack of basic knowledge.
Near-infrared fluorescence (NIRF) imaging was introduced in 2007, enabling noninvasive visualization of the lymphatic vasculature in vivo.8–10 Owing to its high resolution, the technique allows for a detailed anatomical imaging and functional examinations of frequency, velocity, and generation of pressure during the contractions of the superficial lymphatic vessels. The examinations can be conducted under normal circumstances and under exposure to external factors, such as exercise, heat, or pharmacological mediators.11–18
However, to create a better foundation for a possible future treatment of upper extremity lymphedema, a basic knowledge concerning anatomy and function of the superficial lymphatic vessels is required. In addition, a validation of the NIRF imaging technique when applied to the upper extremities is still pending. Thus, the aim of this study was to examine basic values and the inter- and intraindividual variation of lymphatic frequency, velocity, and pumping pressure in the upper extremities when assessed by NIRF imaging.
Materials and Methods
Subjects
Ten healthy young males were enrolled for examination of anatomy and function of upper extremity superficial lymphatic vessels at two occasions. The average age was 25.7 ± 1.3 years and the average body mass index was 23.2 ± 1.6 kg/m2 at the time of examination. All subjects underwent an identical 5-hour protocol, with a 2-week interval between examinations. The two appointments were scheduled at the same time of day to eliminate any diurnal changes. All sequences were recorded of the same segment of lymphatic vasculature to increase comparability.
Experimental setup
The experimental setting was standardized by examining all subjects in supine position using an examination room with a fixed room temperature of 25°C ± 1°C. Upon commensal of the protocol, subjects spent the first 15 minutes in a bed acclimatizing to position and temperature.
NIRF imaging
Indocyanine green (ICG; Nomeco, Denmark) was dissolved in sterile water and then diluted with isotonic saline. Approximately 0.1 mL was injected intradermally with a 31G needle (Wiotech, Denmark), equivalent to a dose of 30 μg ICG per injection site. All participants received a total of six intradermal ICG injections, covering three injections on each arm. Injections were given dorsally between the second and third and between the fourth and fifth proximal phalanges, and palmarly on the central part of the wrist. After uptake, the ICG was excited by a custom-designed 785 nm 450 mW laser (PowerTechnology, Arkansas), with a 780–28 nm band-pass filter. The emission was collected by an electron-multiplier charged coupled device camera (C9100-13 Hamamatsu, Japan), fitted with a Navitar lens (25 mm f0.95) and 835–15 nm band-pass filters. Image capture rate was set to 3/s, and gain was set to 610–1200.
Functional parameters and external interventions
During the 5-hour protocol, functional parameters of the vessels were estimated and the effect of different interventions was studied.
Average frequency and velocity
The average frequency and velocity of the lymphatic propulsions (Fig. 1) were calculated during a 6-minute baseline sequence recorded of each arm.

Chronological sequence of a superficial upper extremity lymphatic vessel. Time from start indicated in seconds. Lymphatic propulsion marked by an arrow.
Changes over time
To examine any possible fluctuations in the lymphatic function during the 5-hour protocol, the frequency and velocity were examined at ∼40, 80, 150, and 180 minutes after injection.
Pumping pressure
The pumping pressure was estimated by placing a pressure cuff around the arm, and then inflating it to 70 mmHg. After inflation, the pressure was lowered with 5 mmHg every 5 minutes until the pressure generated by the contracting lymphatic vessels allowed the lymphatic fluid to pass under the cuff and fill the empty vessel proximal to the cuff. A minimum of two propulsions within 10 minutes were mandatory for confirmation (Fig. 2).
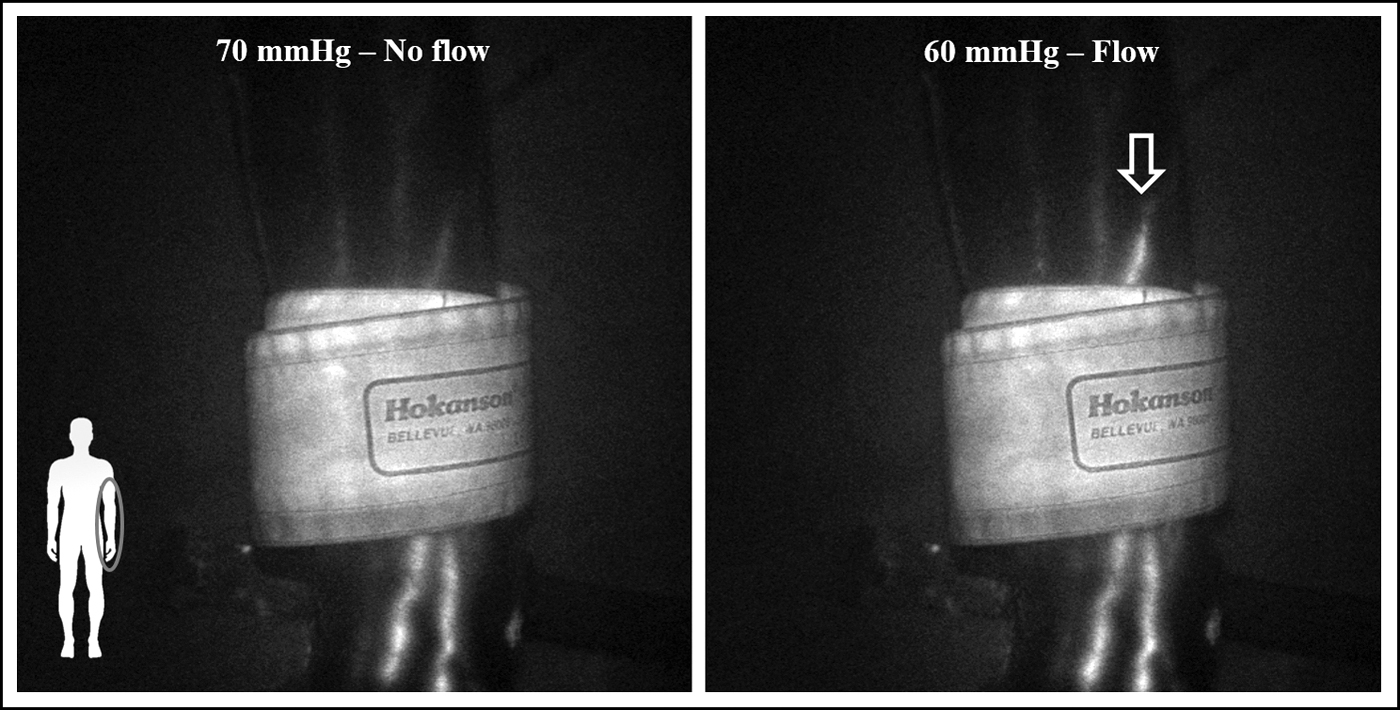
Illustration of pumping pressure measurement. Lymphatic propulsion proximal of the cuff marked by an arrow.
Exercise
The impact of exercise on lymphatic function was studied by instructing the subject to use a handgrip for 2 minutes, with a contraction frequency of one contraction per second, before recording of a 6-minute sequence.
Hyperthermia
The impact of hyperthermia on lymphatic function was studied by placing the arm of the subject in 40°C temperate water for 5 minutes, before recording of a 6-minute sequence.
Data analysis and statistics
All sequences were analyzed for frequency and velocity of the lymphatic packages in a custom-written LabVIEW program (National Instruments, TX). Before analysis, all sequences were blinded. Analysis was done by measuring the intensity of emission in various regions of interest (ROIs), consequently placed over the most distal part of the lymphatic vessels visible in the sequence. The passing of one package of lymphatic fluid, or one contraction, was defined as an increase, a peak, in the measured intensity in the ROI. The frequency of passing lymphatic packages per minute was estimated for all visible lymphatic vessels, and an average was calculated. Accordingly, the velocity of the packages was calculated by estimating the time spent, by the lymphatic package, traveling between two ROIs placed on a linear vessel with a minimum of 5 cm distance between. Lymphatic packages pausing or stopping halfway were excluded.
All data were tested for normality and presented as mean ± standard deviation. Using GraphPad Prism 5, data were tested for significance in difference with either paired Student's t-test (data with two samples) or one-way analysis of variance with Bonferroni's post-test (data with three or more samples). Significance level was set to 0.05 in all tests.
Interobserver variation was tested using the intraclass correlation coefficient (ICC) calculated using STATA with a two-way mixed model for absolute difference between two measurements. The ICC was presented with 95% confidence interval. 19
Ethical approval
Written informed consent was obtained from all participants. The study was approved by The Central Denmark Region Committees on Health Research Ethics (1-10-72-99-17) and was conducted in accordance with the Helsinki declaration.
Results
Overall, 140 sequences were recorded, covering 511 lymphatic vessels analyzed for frequency. Velocity was calculated for lymphatic packages in 237 of these vessels, the remaining vessels were excluded due to either absence of activity, a distinctly tortuous anatomy, or due to either pauses or full stops in the movement of the lymphatic packages. On average, 3.7 ± 1.4 lymphatic vessels were analyzed on each arm, the density of vessels ranging from 2 to 7 per arm. The anatomy of these superficial lymphatic vessels was found to be diverse and with great interindividual variation concerning number of vessels and the course of these. The 2-week interval did not alter the vessels visible for examination (Supplementary Fig. S1).
Functionally, the lymphatic vessels contracted with an average frequency of 0.9 ± 0.4/min at baseline, and the packages traveled with an average velocity of 1.1 ± 0.3 cm/s. The average frequency was 0.9 ± 0.4/min at the first visit and 0.9 ± 0.4/min at the second visit. The average velocity was 1.1 ± 0.3 cm/s at the first visit and 1.0 ± 0.3 cm/s at the second visit (Fig. 3). There was no significant difference between the frequency and the velocity at the two visits p > 0.05.

Baseline frequency at first (n = 10) and second visit (n = 10)
There was no difference in the frequency at 40 and 80 minutes after injection, frequency being 0.9 ± 0.4/min and 0.8 ± 0.4/min, respectively. However, after 150 minutes, the frequency significantly decreased by ∼30% to 0.6 ± 0.4/min, p < 0.05. This decrease persisted through to the last estimation at 180 minutes, 0.6 ± 0.3/min. The velocity of the lymphatic packages was unaltered throughout the entire protocol, with velocities of 1.1 ± 0.3 cm/s, 1.0 ± 0.2 cm/s, 1.0 ± 0.2 cm/s, and 0.9 ± 0.3 cm/s, respectively (Fig. 4).
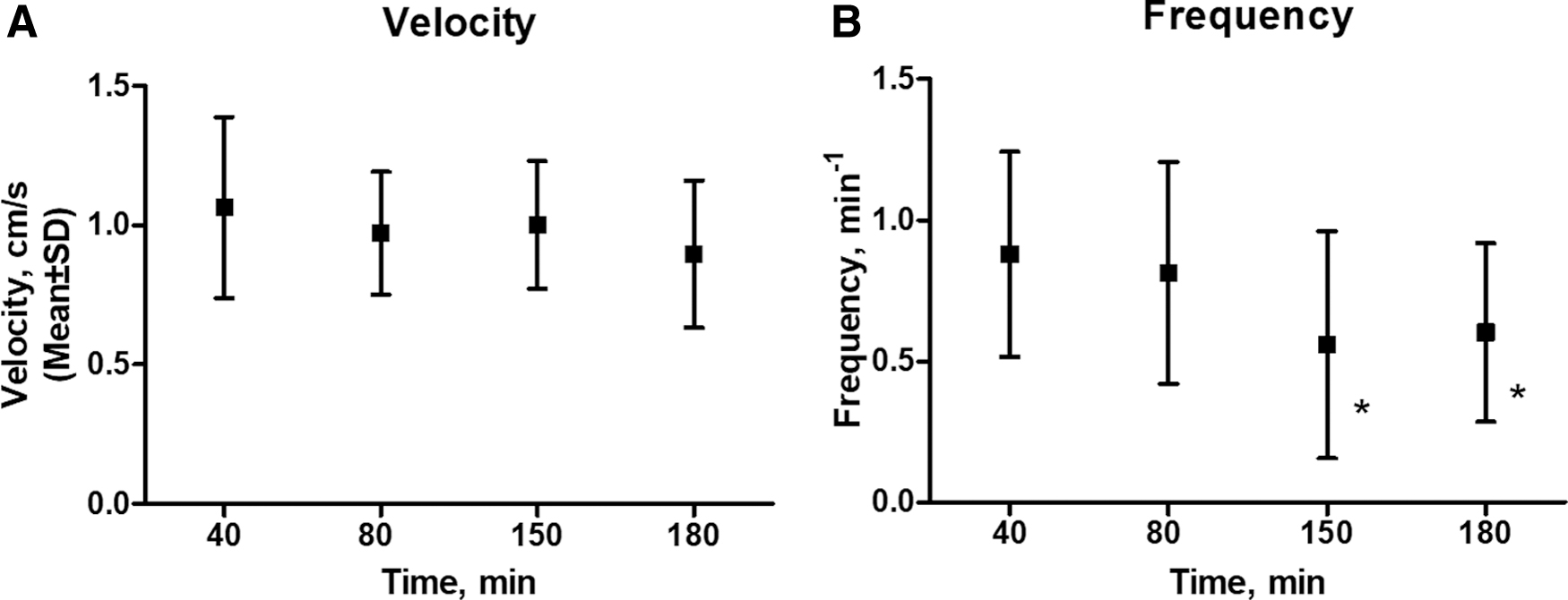
Frequency over time after injection, n = 20
The average maximal pressure generated by contractions of the lymphatic vessels was 59 ± 12 mmHg (Fig. 5). There was no significant difference in the pumping pressure at the two visits p > 0.05.
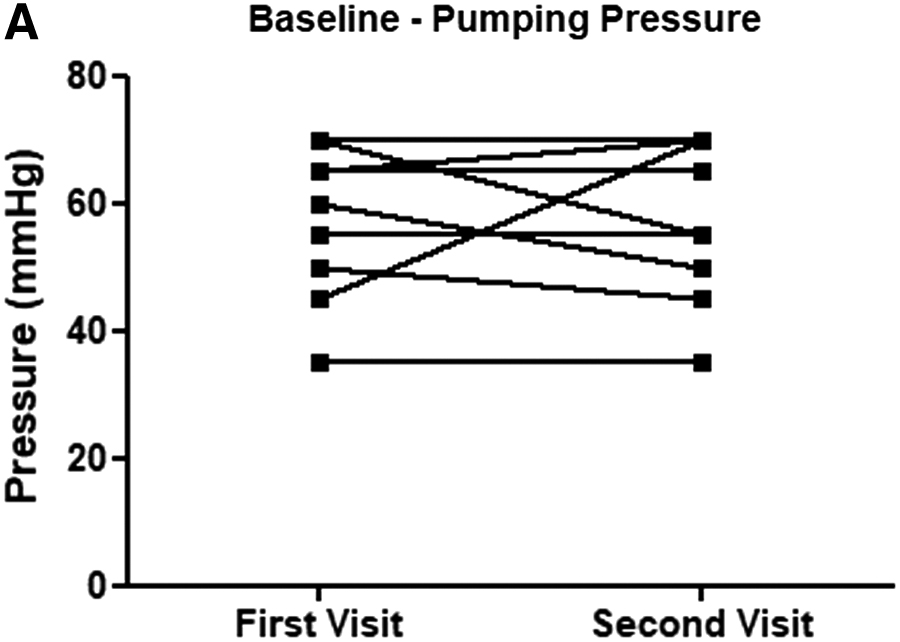
Baseline pumping pressure at first visit (n = 10) and second visit (n = 10)
Interventions
After 2 minutes of handgrip exercise, the frequency significantly decreased from 1.1 ± 0.3/min to 0.9 ± 0.4/min, p < 0.05. Contrarily the velocity of the lymphatic packages significantly increased after exercise, with a velocity of 1.0 ± 0.3 cm/s before and 1.2 ± 0.3 cm/s after, p < 0.05 (Fig. 6).
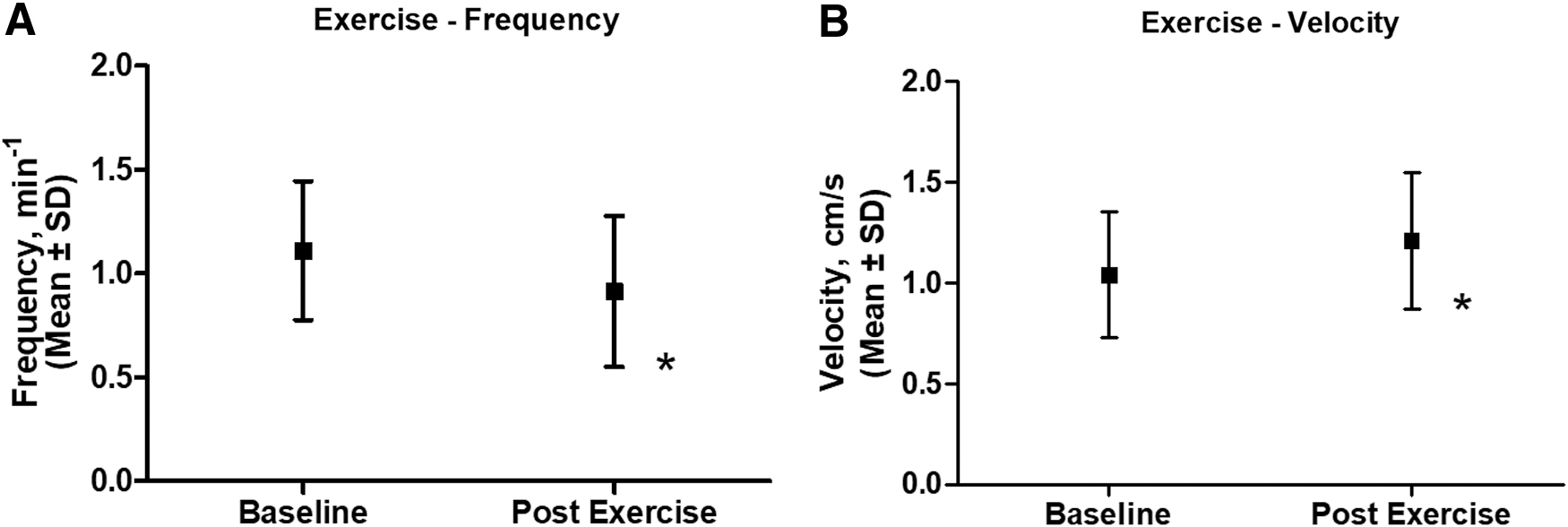
Frequency before (n = 20) and after exercise (n = 20)
After 5 minutes placement in 40°C water, the hyperthermia of the lower arm significantly increased the frequency of the lymphatic vessels from 1.1 ± 0.3/min to 1.5 ± 0.5/min, p < 0.05; however, the velocity of the lymphatic packages stayed unaltered at 1.0 ± 0.3 cm/s before and 1.1 ± 0.4 cm/s after (Fig. 7).
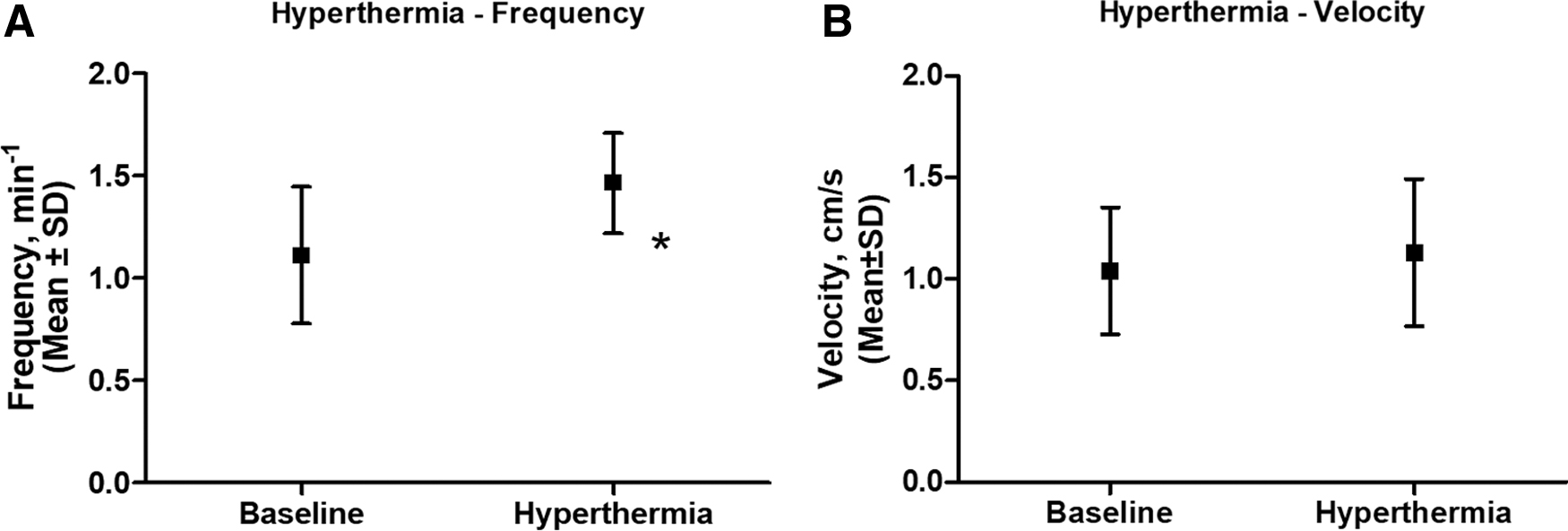
Frequency before (n = 20) and during hyperthermia (n = 20)
Interobserver variability
When looking at the interobserver variability of the lymphatic parameters, we found an ICC of 0.97 (0.92–0.99) when analyzing the sequences of pumping pressure, and an ICC of 0.94 (0.85–0.98) when analyzing frequency. The calculations for these two parameters consisted of 20 pairs of observations. The estimation and calculation of velocity had an ICC of 0.87 (0.62–0.96). The analysis of velocity consisted of 15 pairs of observations.
Discussion
The aim of this study was to examine the repeatability of functional parameters of the upper extremity superficial lymphatic vessels when examined by NIRF imaging. We demonstrated that the technique is a reliable and easily applicable alternative when examining both lymphatic anatomy and function. The three injections on each arm allowed for visualization and examination throughout the 5-hour protocol, with dye being taken up by the collecting lymphatic vessels almost immediately after injection.
Repeatability and changes with time
The 2-week interval between sequences did not markedly affect the vessels visualized. Thus, the same vessels were distinguishable and repeatedly visualized at the two examinations (Supplementary Fig. S1). When comparing the vessel anatomy with that found by Lee et al., 20 there was a high degree of similarity. However, the current use of multiple injection sites seem to have made a greater number of vessels vissible.
When looking at frequency, velocity, and pumping pressure, the 2 weeks between examinations did not alter the value of these functional parameters. This correlates with the results of Groenlund et al. 17 who similarly on the lower extremities found good repeatability of the parameters.
When looking at the frequency at 40, 80, 150, and 180 minutes after injection, there was a significant drop in frequency at 150 and 180 minutes after injection compared with 40 and 80 minutes after. This is in contradiction to results previously obtained of lymphatic function of the superficial lymphatic vessels on the lower extremities, where no decrease in frequency was observed during the 4-hour protocol. 17 The initial increase in frequency in the upper extremities might be due to a greater relative impact of the injected ICG on the amount of fluid being available for the lymphatic vessels. Thus, resulting in an initial increase in frequency, followed by a decrease at 150 minutes when the injected fluid had been removed.
Interobserver variability
The relatively high values of ICC for all functional parameters underline the low variation in estimates between observers. It proves the lymphatic propulsion to be distinguishable and estimation of function to be rather unambiguous when sequences are analyzed as previously described.
Functional parameters
The frequency of 0.9 ± 0.4/min and velocity of 1.1 ± 0.3 cm/s found in this study are in accordance with values found by previous studies of frequency and velocity of human lymphatic vessels. Rasmussen et al. found a contraction frequency of 1.3 ± 1.2/min and a velocity of 0.8 ± 0.4 cm/s when examining both arms of 12 healthy subjects with an average age of 38.2 ± 11.0 years. 14 Similarly, Groenlund et al. found an average frequency of 0.6 ± 0.1/min and a velocity of 1.5 ± 0.2 cm/s when examining the lower extremities of 10 healthy young males. 17
In this study, the pressure generated by the contraction of the superficial lymphatic vessels was estimated to be 59 ± 12 mmHg. However, the study merits one main limitation. Thus, in 3 out of 10 examinations, the lymphatic vessels examined were able to contract and move the lymphatic fluid under the cuff at the starting pressure of 70 mmHg. Accordingly, the result may represent an underestimation, as the lymphatic vessels may have been capable of generating an even higher pressure, had the study design provided the possibility. A similar study by Belgrado et al. estimated the mean lymphatic occlusion pressure of the upper limb to be 86 ± 4 mmHg when examining 30 healthy subjects using NIRF imaging. 18 Belgrado et al. practiced a fill and flush technique to ensure a large amount of fluid in the lymphatic vessels distal to the cuff. Thus, the higher pumping pressure found might be due to a greater amount of fluid and wall tension, as this is known to influence lymphatic vessel function. 21 Using a similar protocol as this study, Groenlund et al. found a pumping pressure of 57 ± 9 mmHg when examining the lower extremity pumping pressure of 10 healthy young males. 17 Finally, in an ex vivo study by Telinius et al., human mesenteric lymphatic vessels were found able to generate tensions equivalent to a pressure of 47 ± 5 mmHg while mounted in a myograph. 21
Interventions: hyperthermia and exercise
Hyperthermia and exercise have previously been shown to result in changes in frequency and velocity and lymph flow of the lymphatic vessels. 22 When examined on the upper extremity, the 2 minutes of exercise reduced the frequency significantly with ∼18% and the velocity of the lymphatic packages significantly increased by 16%. This is in coherence with what has previously shown by Groenlund et al. 17 when examining the impact of exercise on the lower extremities. Here the frequency was found to decrease by 12% immediately after exercise, although the tendency was nonsignificant. However, 10 minutes after exercise, the frequency significantly decreased by 49%. The same study found the velocity of the lymphatic packages to significantly increase by 46% immediately after exercise. After hyperthermia, the frequency of the lymphatic vessels significantly increased by 32%, and the velocity was unaltered. This increase of lymphatic frequency is markedly smaller compared with the 135% found by Groenlund et al. 17 Although the relative changes seem to vary between protocols and between the upper and lower extremities, the basic physiological response seems to be the same.
Implications and perspective
We have confirmed that NIRF imaging can be applied to examine the anatomy and function of the superficial lymphatic vessels in vivo. The technique produces high-quality images and can be easily applied, with little inconvenience for the examined subjects. The functional parameters of frequency, velocity, and pumping pressure showed no variation over a 2-week period. The lymphatic propulsions were distinguishable and the results showed very low interobserver variation. Thus, frequency, velocity, and pumping pressure may in the future be used to evaluate function of lymphatic vessels in health and disease. Possible future examinations of patients suffering from lymphedema may be improved by increasing the starting pressure of the measurement to possibly as high as 100 mmHg in line with the results of Belgrado et al. 18 Finally, examinations should be conducted with standardization of temperature and exercise, as these parameters were shown to alter the lymphatic function.
Footnotes
Acknowledgments
The authors thank the participants for volunteering their time.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The Danish Cancer Society and Agnes Niebuhr Andersons Foundation are acknowledged for their generous financial support of this project. B.K. was the recipient of a scholarship from The Danish Cancer Society.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.