
Abstract
Background:
Gynecological cancer-related lymphedema (GCRL) is a devastating condition that adversely influences function, health, and quality of life. We conducted a randomized-controlled clinical study as well as in vitro experiments to investigate the efficacy and safety of far infrared radiation (FIR) to treat lymphedema in patients having previously undergone surgery for gynecological tumors.
Materials and Methods:
Seventy-four women with GCRL, cancer free for 5 years or more, were randomly allocated into two treatment groups: standard of care with bandage treatment and treatment with FIR plus bandage. Variations of fluid, circumference of lymphedematous limbs, serum tumor markers (cancer antigen 125 [CA125]), inguinal-pelvic lymph nodes, vagina, lungs, and adverse reactions were assessed after 1 year. In vitro experiments examined the effects on cell viability, proliferation, apoptosis, and the cell cycle of fibroblast, A2780, SKOV-3, HELA, and Ishikawa cells.
Results:
The FIR+bandage group showed significantly decreased tissue fluid and reduced limb circumference (p < 0.05) in comparison with the control group at 1 year. There was no increase of serum CA125 in both groups, and no recurrence of neoplasia or lymphadenopathy was detected. No adverse reactions were recorded. In addition, no changes were detected after FIR treatment for fibroblast, A2780, SKOV-3, HELA, and Ishikawa cells in cell viability, proliferation, apoptosis, and cell cycle.
Conclusion:
FIR can be used to treat patients with GCRL following gynecological cancer treatment. Following clinical and experimental studies, we confirm that FIR is an oncologically safe treatment for lymphedema in gynecological tumor patients.
Introduction
Patients affected by malignant gynecological tumors represent ∼17% of all female malignant tumors worldwide. 1 Lower limb lymphedema is a relatively common complication after gynecological tumor resection surgery with an incidence reported between 7% and 78%.1–3 The main cause is due to pelvic irradiation and lymph node dissection as part of disease management, resulting in loss of groin and pelvic lymph nodes, destruction of lymphatic networks and consequent lymph flow obstruction, and fibrotic tissue formation.1,3
Postoperative lymphedema after gynecological tumor excision can gradually aggravate and progress into chronic lymphedema. It is characterized by increased intracellular fluid, extracellular fluid, protein, lipid deposition, and fibrosis.4–6 Clinical symptoms include lower extremity swelling, deformity, heaviness, weakness, pain, decreased skin elasticity, limited joint activity, and is often accompanied by recurrent cellulitis and dermatolymphangitis (DLA). This can lead to a significant impairment of the patient's quality of life and psychological well-being.7,8
Far infrared radiation (FIR) treatment acts on tissues similarly to hyperthermia, through three main biological effects: radiation, vibration (or resonance), and a thermal effect.9–17 The advantages consist of promoting flow in the microcirculation flow and increasing collateral lymphatic reflux, consequently relieving lymphedema and heaviness.12,13 This procedure has been used for many years to treat lymphedema of the extremity, 12 showing a significant reduction of the circumference and tissue fluid of the affected limbs,16,18 releasing lymphedema and tissue fibrosis, 19 and decreasing the frequency of infections or DLA.20,21 However, the oncological safety of the FIR is not yet completely elucidated, and there is a theoretical potential activation of residual malignant cells. Therefore, this study aims to explore the efficacy and safety of FIR treatment for patients affected by gynecological cancer-related lymphedema (GCRL) by conducting a clinical study and in vitro cell experiments.
Materials and Methods
Clinical study
A randomized-controlled study was performed analyzing data of patients with lymphedema of lower extremities treated at the “Lymphatic Center” of the Ninth People's Hospital in Shanghai between January 2013 and January 2018. Seventy-four individuals were included with the following criteria: patients affected by GCRL for more than 1 year; patients who underwent gynecological cancer surgery 5 years prior or more; and patients able to receive FIR+bandage treatment or single bandage treatment and able to complete 1-year follow-up. Exclusion criteria for patients from the study were as follows: clinical or oncological evidence of cancer recurrence, gynecological cancer surgery within 5 years, important comorbidities such as hypertension, liver disease, coronary artery disease, cerebrovascular disease, peripheral arterial disease, recurrent episodes of DLA or thromboembolism, lymphedematous limbs too large to be placed in the curing cabin, and patients who could not be followed up after the treatment (Fig. 1).

CONSORT flow diagram showing that 86 individuals met the inclusion criteria. Of those, 11 were excluded and 1 withdrew. The remaining 74 cases were allocated into two groups: single bandage treatment and FIR+bandage treatment. FIR, far infrared radiation.
All patients were randomly allocated into two groups by a random draw. Group 1 consisted of patients who underwent a single bandage, while group 2 represented patients who underwent FIR+bandage treatment. Before treatment, each individual was randomly allocated a number between 1 and 74. Odd numbers included FIR+bandage treatment group. Even numbers represented the control group (single bandage).
The Ethics Committee of the Ninth People's Hospital of Shanghai approved the research study. All relevant regulations as well as the guidelines of the Declaration of Helsinki were followed accordingly. Written informed consent was obtained for all participants.
Bandage treatment
A trained specialist therapist performed a single elastic bandage (Paul Hartmann AG, Heidenheim, Germany) on the affected limbs for 4 weeks. Patients continued to wear bandage 24 hours a day. The patient was instructed to continue the bandaging for up to 1 year.
FIR therapy device
The FIR therapy machine was independently developed by the Ninth People's Hospital affiliated to Shanghai Jiao Tong University, School of Medicine, China.18,22 The far or thermal infrared had a wavelength between 6 and 14.0 μm.
FIR+bandage treatment
Patients of this group received FIR and bandage treatment. FIR thermotherapy was performed for 1 hour every day, at a temperature of 42°C, for 4 weeks. After each FIR session, the same specialist therapist performed a single elastic bandage on the affected limbs, which the patient would wear for the remaining 23 hours until the next FIR session. The patient was instructed to continue the bandaging for up to 1 year.
Data collection and evaluation
Patients were followed up for a year and measures were recorded before and after the treatment. Data included the following: (1) fluid of the affected limb, measured by a multiple frequency bioelectrical impedance analysis machine (Inbody 3.0; Biospace, Korea); (2) lymphedematous limb circumference, measured by taking five points with a standard measuring tape 18 ; (3) tumor marker cancer antigen 125 (CA125), a normal range for CA125 was considered 0–35 U/mL and positive (+) when CA125 > 35 U/mL; (4) transvaginal ultrasonography, a vaginal ultrasound examination was performed to assess the vagina, uterus, and appendages and considered positive (+) in case of suspecious lesion; (5) inguinal lymph node palpation and vagino-recto-abdominal examination, an accurate clinical inspection of inguinal lymph nodes and vaginal, uterus, cervix, uterus, rectal status was performed and atypical findings were considered positive (+); (6) chest X-ray: patients underwent chest X-ray to detect metastatic lesions of the lungs and the presence of a new nodule was recorded as positive (+), otherwise negative (−); (7) adverse reaction: any thermal injury, local infection, fever, and limb discomfort or pain were recorded as positive (+), otherwise negative (−).
In vitro study
Cell cultures
Epidermal fibroblasts of lower limb were extracted from healthy male donors after patient informed consent was obtained. Human ovary cancer cell lines A2780, SKOV-3, and HELA were obtained from the American Type Culture Collection (ATCC), as well as the human endometrial carcinoma cell line, Ishikawa cell. Cells were regularly maintained in Dulbecco's modified Eagle's medium supplemented with 10% fetal bovine serum, penicillin (100 U/mL), and streptomycin (100 mg/mL) at 37°C under 5% CO2.
Far infrared ray treatment
FIR treatment was performed using a device delivering FIR with variable wavelengths between 6.0 and 14.0 μm. The FIR treatment cell groups, including A2780, SKOV-3, HELA, and Ishikawa cell lines, were incubated in culture dishes, placed in a square box under an FIR device at a 30 cm irradiating distance. The temperature of the incubation chamber was maintained at around 37 ± 0.5°C and constantly monitored by a real-time temperature detector. In accordance with that in clinical trials, the irradiation time was set for 1 hour. Control cell groups were maintained in the same conditions but not exposed to FIR.
Cell viability and proliferation
A cell counting kit-8 (CCK-8) was used to screen cell viability and proliferation. Cells were incubated in 96-well plates with a density of 2 × 103 cells per well. The irradiated group was treated for 1 hour daily for 7 days (37 ± 0.5°C), while the unirradiated group was placed in the same condition, but not subjected to radiation.
Cell viability and proliferation capability were evaluated using CCK8 kits immediately after each daily FIR treatment. During the experiments, cells were incubated in 10 μL CCK-8 solution that was diluted in 100 μL cell culture medium, and the 96-well plates were constantly incubated for 3 hours. The absorbance was measured at a wavelength of 450 nm on a microplate reader. The experiment was replicated three times.
Fluorescence-activated cell sorting analysis of cell cycle
The FIR-irradiated groups were treated for 1 hour at 37 ± 0.5°C. After treatment, cells of FIR groups and control groups were collected and fixed in 70% ethanol, washed twice with previous ice-cold phosphate buffer saline (PBS) and resuspended in 500 μL PBS. Cell suspensions were incubated with RNase A (50 μg/mL) for 30 minutes at 37°C room temperature, sequentially stained with propidium iodide (50 μg/mL) for 1 hour, and then analyzed on a flow cytometer. Three independent experiments were performed.
Evaluation of apoptosis
The Annexin V-FITC/PI Apoptosis Detection Kit (BD Biosciences, San Jose, CA) was used following the manufacturer's instructions. Cells showing Annexin V+/PI− staining were considered early apoptotic cells, and those showing Annexin V+/PI+ staining were considered late apoptotic cells. After the staining, the number of apoptotic cells was detected and analyzed using a BD FACSCalibur flow cytometer and the CELL Quest software. The experiment was replicated three times.
Statistical analysis
Change in fluid value of lymphedematous limb and change in circumference of the affected limb were statistically analyzed using the Wilcoxon rank-sum (Mann–Whitney U) test. The outcome measures (tumor markers, ultrasonography test, palpation, X-ray, and adverse reactions) were statistically analyzed using the chi-square test. For the in vitro study, data are presented as mean ± standard deviation. All the experiments were replicated three times. Unpaired Student's t-tests were performed to evaluate the differences between FIR-irradiated groups and nonirradiated groups for all cell types. All data were analyzed using version 19.0 of the Statistical Package for Social Sciences (SPSS, Inc., Chicago, IL), with a p-value <0.05 being considered statistically significant.
Results
Clinical study results
A total of 74 cases of lower extremity GCRL were treated at our institution. Demographics and characteristics of each group are summarized in Table 1. One patient withdrew from the trial, therefore was excluded before the random allocation.
Patients' Characteristics
SD, standard deviation.
Change in fluid in affected extremity
The amount of fluid in the affected limb was 6.146 ± 1.020 kg in group 1 before treatment. One year later, it was reduced to 5.588 ± 0.979 kg, with a change in value of 0.558 ± 0.381 kg (p = 0.022). In group 2, the amount of fluid in the affected limb was 6.408 ± 1.292 kg before treatment. One year later, it was reduced to 5.605 ± 1.102 kg, with a change in value of 0.803 ± 0.615 kg (p < 0.001). The amount of fluid difference in group 2 was obviously higher than in group 1, with a p-value of 0.014 (Table 2), comparing the fluid variation between the two groups. That value suggested that FIR+bandage therapy alleviated lymphedema better than bandage single therapy.
Change in Values of Fluid and Circumference of Lymphedematous Limb
Change of circumference measures of affected extremity
In the group 1, the average circumference was decreased from 45.238 ± 3.973 cm to 44.053 ± 3.553 cm, with a change in value of 1.184 ± 1.523 cm (p < 0.001) after 1-year treatment. In the FIR+bandage group, the average circumference was reduced from 44.618 ± 3.812 cm to 42.808 ± 2.909 cm, with a change in value of 1.810 ± 1.829 cm (p < 0.001) after 1-year treatment. The circumference changes in group 2 were obviously higher than that in group 1, with a p-value of 0.015 (Table 2, Fig. 2). This result has demonstrated that the FIR+bandage treatment is more effective than a single bandage treatment to reduce the circumference.
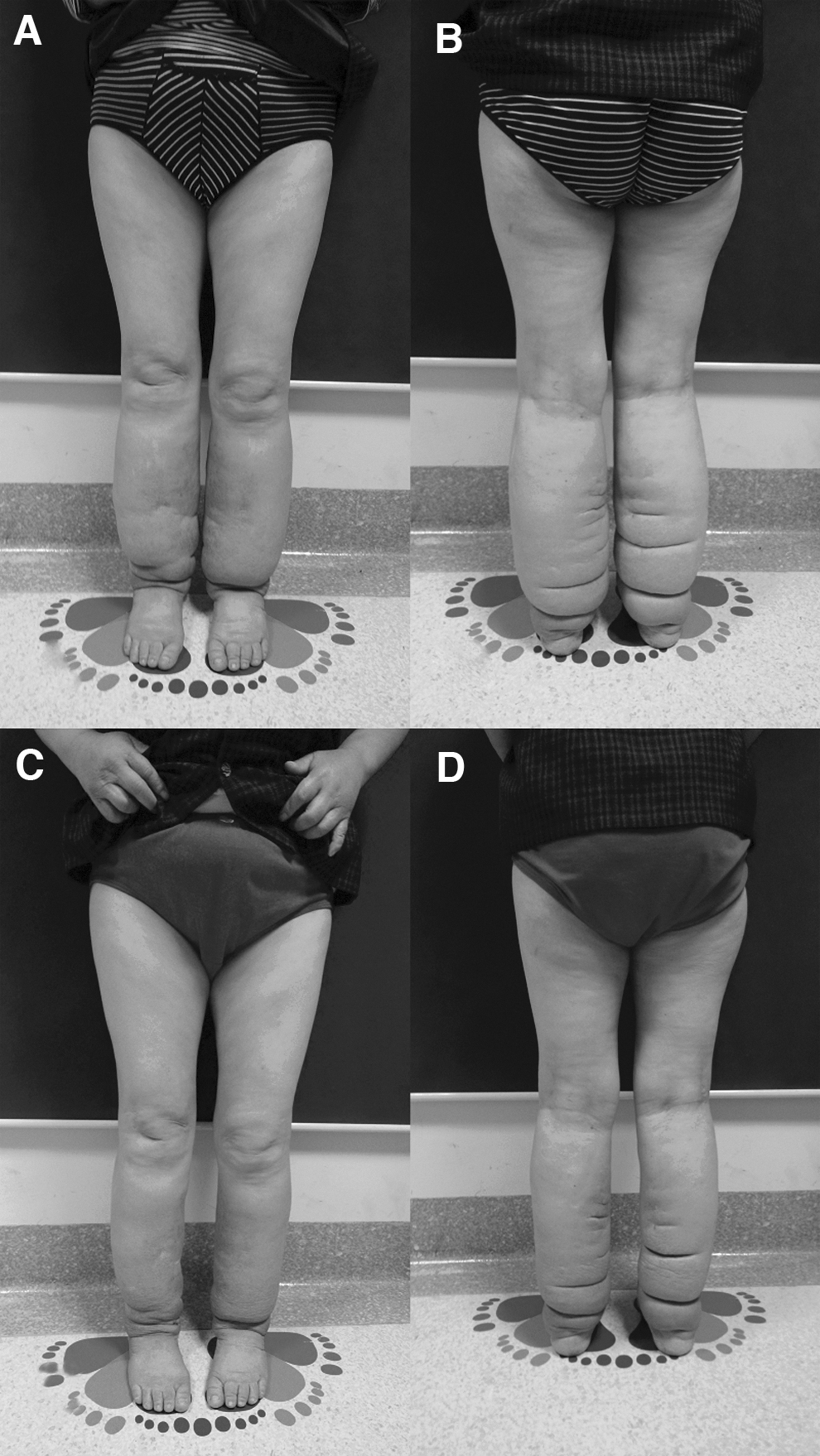
A patient with bilateral lymphedema treated with FIR and bandage.
Tumor marker CA125
After 1 year, there was no patient detected with abnormal values of CA125 in both groups 1 and 2. The change of CA125 in group 1 was similar to group 2 (p > 0.05) (Table 3).
Results of Clinical Studies
CA125, cancer antigen 125.
Transvaginal ultrasonography
One year later, the results showed that no patient was diagnosed with lymphadenopathy or newly enlarged nodules in both groups. The change of these items in group 1 was similar to group 2 (p > 0.05) (Table 3).
Inguinal lymph node examination and vagino-recto-abdominal examination
One year later, patients underwent inguinal-pelvic lymph node examination and vagino-recto-abdominal examination. The results showed that no patient was detected with lymphadenopathy or newly enlarged nodules in both groups. The changes in group 1 were similar to group 2 (p > 0.05) (Table 3).
Chest X-ray
One year following treatment, patient received a chest X-ray. The results showed that no patient was diagnosed with lymphadenopathy or newly enlarged nodules in both groups. The results of group 1 were comparable with the group 2 (p > 0.05) (Table 3).
Adverse reactions
Patients were followed up for eventual adverse reactions caused by FIR or bandage, such as rash, blisters, infection, fever, discomfort, or pain. There were no adverse events or side effects. There was no significant difference between the FIR+bandage group and single bandage group (p > 0.05) (Table 3).
Clinical cases
A 45-year-old woman underwent radical resection of a cervical cancer 7 years earlier. Three years later she developed severe (stage III) bilateral lower limb lymphedema. This patient followed the FIR and bandage protocol for 1 year. One year later, the fluid of the lower extremities decreased by 1.25 kg and the average circumference decreased by 3.14 cm. The results of tumor marker CA125, ultrasonography, chest X-ray did not show any cancer recurrence (Fig. 2).
A 51-year-old woman had a radical resection for endometrial cancer 6 years earlier. Two years later, she developed stage III left lower limb lymphedema. This individual followed for 1 year the FIR and bandage protocol. After a year, the fluid of the lower limb decreased by 0.71 kg and the average circumference reduced by 1.93 cm. The results of tumor marker CA125, ultrasonography, chest X-ray did not show any cancer recurrence (Fig. 3).

A patient with unilateral lymphedema treated with FIR and bandage.
In vitro study results
Cell viability and proliferation
We analyzed the effects of FIR on fibroblasts, A2780, SKOV-3, HELA, and Ishikawa cells. The CCK-8 assay was performed to examine the influence of FIR on cell viability and proliferation analyzed by cell growth curve. All cells displayed neither increasing nor reducing ability of cell viability or proliferation after the treatment of FIR once a day, lasting for a total of 7 days (Fig. 4A–E).

Cell viability and proliferation ability were determined in FIR groups and non-FIR treatment groups of fibroblasts
Cell cycle analysis
To investigate the influence of FIR on the cell cycle, we performed flow cytometry analysis. The percentage of cells in each phase of the cell cycle was determined promptly after the FIR treatment. The results indicated that no significant difference was detected between the FIR treatment group and non-FIR treatment group (Fig. 5A–J, Table 4).
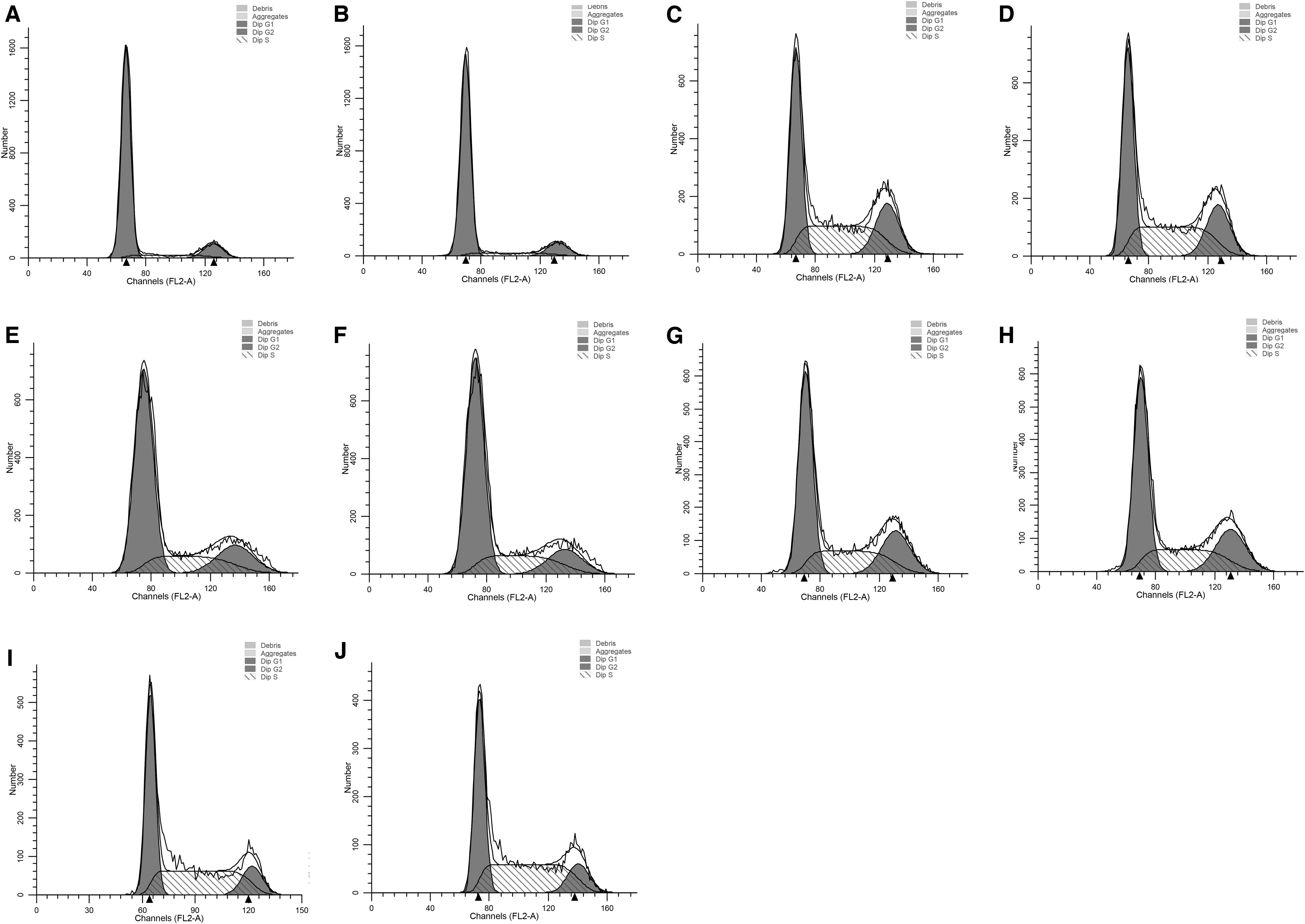
FACS analysis of cell cycle. No significant difference was detected between the FIR treatment group and non-FIR treatment group in human fibroblasts
Cell Cycle Analysis
Analysis of cell cycle in untreated and far infrared radiation-treated human fibroblasts, A2780, SKOV-3, HELA, and Ishikawa cells. Data show mean and SD of three independent experiments.
Evaluation of apoptosis
The influence of FIR treatment on cell apoptosis of fibroblasts, ovarian carcinoma cell lines, and endometrial carcinoma cell lines was determined by flow cytometry using the Annexin V-FITC/PI apoptosis kit. The results showed that the FIR treatment did not significantly alternate the living, early, or late apoptosis percentage of FIR-treated cells (Fig. 6).

Percentage of living, early, and late apoptotic human fibroblasts, A2780, SKOV-3, HELA, and Ishikawa cells unexposed or exposed to FIR treatments. Bar graphs show the compiled mean value ± SD of three independent experiments. The results did not show significant differences between non-FIR and FIR groups. SD, standard deviation.
Discussion
Infrared radiation is an invisible portion of the electromagnetic spectrum with wavelengths ranging from 0.75 to 100 μm (750–10,000 nm), frequencies ranging from 400 to 3 THz, and a photon energy range of 12.4 meV–1.7 eV. Infrared rays are further divided into the following: near infrared, medium infrared, and far infrared.14,16,22–24 FIR has a range of wavelength between 3 and 100 μm. FIR has three main biological effects: radiation, vibration (or resonance), and thermal effect 25 Radiation and resonance promote the oscillation of free ions, resulting in the denaturation of macromolecules such as proteins leading to an increase in the absorption of proteins in tissue frameworks. Thermal effects induce angiogenesis and promote microcirculation by expanding blood and lymphatic vessels, activating Langerhans cells and macrophages.12,20,26 Between the infrared radiation bands, only the FIR is able to transmit energy solely in the form of heat, which is perceived by the thermoreceptors of the human skin as radiant heat.16,27
In our previous study, 18 we found that FIR therapy is able to reduce the concentration of protein, hyaluronic acid, fibrosis, and immune-related cytokines, 19 and release the fibrosis of lymphedema tissue and inhibit the inflammation. 21 Bandage treatment has been shown to be a safe conservative treatment for lymphedema and is widely utilized to reduce the accumulation of lymph fluid. 28 In this study, when compared with bandage treatment, the FIR+bandage treatment showed a greater reduction in fluid (p = 0.014) and circumference (p = 0.015) (Table 2), which suggests that the use of FIR combined with bandage treatment can be more effective.
Previous studies mainly focused on assessing the effect of FIR as a valid volume reduction therapy for lymphedema.12,18 However, it remains unknown whether the FIR treatment influences gynecological tumor recurrence rates and increases its metastatic risk. Ishibashi et al. 29 conducted an in vitro investigation with five human cancer cell lines (A431, vulva; HSC3, tongue; Sa3, gingival; A549, lung; and MCF7, breast) to evaluate the effects of FIR. The overall opinion was that the FIR effect varied in these five cancer cell line types. The proliferation-suppressing effect of FIR, in some cancer cell lines, is regulated by the basal expression level of the heat shock protein (HSP) 70A. Therefore, FIR may be an effective medical treatment for some cancers expressing low levels of HSP70.
The current diagnosis of recurrence and metastatic gynecological tumors mainly includes biopsies of adjacent tissues, sentinel lymph nodes or distant suspicious loci, and blood and radiological investigations.30,31
CA125 has been found to be upregulated in gynecological cancer tissues and it serves as a predictor for gynecological cancer recurrence. 32 In our study, no patient in either treatment group demonstrated CA125 positivity (Table 3). We suggest that the FIR treatment is a safe and effective method for treating GCRL due to its unlikeliness to induce tumor recurrence or systematic metastases.
Transvaginal ultrasound, inguinal lymph node palpation, and vagino-recto-abdominal examination were used clinically to screen for cancer recurrence in tissues and regional lymph nodes.33,34 After 1 year of follow-up in our study, no patients were found to have a new pathology in the uterus or uterine adnexa, and no patients showed new evidence of lymphadenectasis (Table 3). This seems to further confirm the safety and reliability of FIR.
Chest X-ray is a simple and low-cost method widely used to screen for pulmonary metastasis caused by gynecological tumors. 35 No patients in our study were found to have suspicious lung nodules (Table 3), suggesting that FIR treatment did not promote lung metastasis.
During clinical follow-up, we monitored patients for eventual adverse reactions after FIR therapy. No patients reported side effects or discomfort of the treated limbs, indicating good tolerance to FIR treatment (Table 3).
In vitro studies were conducted into the potential effects of FIR on residual tumor cells in patients with GCRL, matching conditions that FIR was applied to various cell lines. Cell proliferation and the viability of fibroblasts, A2780, SKOV-3, HELA, and Ishikawa cell lines were examined and showed no significant differences between the treatment and control groups (p > 0.05) (Fig. 4A), indicating that FIR is unlikely to promote proliferation of cancer cells or increase the risk of recurrence.
Similarly, cell cycle tests were performed on all cell lines treated by FIR and control groups and demonstrated no difference in response (p > 0.05) (Fig. 4B, Table 4), indicating that FIR treatment did not impact on the cell cycle and further confirmation that cancer cells are unlikely to be activated.
Chen et al. reported that the FIR may slow down the apoptosis of keratinocytes. 23 However, in our study, the apoptosis of fibroblasts, A2780, SKOV-3, HELA, and Ishikawa cells was not affected after FIR (Fig. 4C). This suggests that FIR therapy neither promoted nor delayed apoptosis and can be considered a safe therapeutic treatment.
The limitation to this study is that all patients in the clinical group were more than 5 years postgynecological tumor resection, where any remaining gynecological tumor cells would be relatively stable and difficult to activate. However, it is still unclear whether FIR therapy is safe for patients within 5 years of their gynecological tumor resection. Although in vitro cell experiments indicated that FIR treatment would not activate gynecological tumor cell lines, it would still be necessary to further examine whether FIR could be safely applied to patients with GCRL within 5 years of tumor resection. Furthermore, additional studies are warranted to determine the value and efficacy of FIR associated with more intensive lymphedema management such as complete decongestive therapy.
Conclusion
FIR can be safely used and combined with bandage therapy to treat patients with lower limb lymphedema after a 5-year cancer-free period following gynecological cancer resection, with further studies needed to examine its earlier use. Our clinical and experimental studies found that FIR did not promote recurrence or metastasis of the gynecological cancer and was well tolerated with no adverse reactions or side effects.
Footnotes
Authors' Contributions
L.X., C.C., and F.N. conception and design of the work, and are major contributors in writing the article. N.F.L. and B.X. analysis and interpretion of data. A.A.M., D.L., and C.C.C. drafting of the work, review, and corrections. K.L. and Y.Z. participated actively in the execution of the study. All authors read and approved the final article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This article is funded by the National Natural Science Foundation of China (81772098), the Clinical research booster program (JYL027), the Shanghai Health Municipal Bureau foundation (20152227), the National Natural Science Foundation of China (81071569), and the National Natural Science Foundation of China (82000456).