
Abstract
Background:
Treatment for patients with comorbid lymphedema and varicose veins is controversial. Surgical options for these patients are limited. The study was aimed to investigate the validity of combined lymphovenous anastomosis (LVA) and great saphenous vein stripping (GSVS) for comorbid lymphedema and varicose veins.
Methods:
Thirteen patients were involved in the study, and the detail was 21 edematous lower limbs (with coexisting varicose veins and lymphedema; the varicose vein and lymphedema [VL] group) who underwent combined GSVS and LVA therapy. Fifteen patients (with 30 edematous lower limbs and lymphedema only; the lymphedema [L] group) who underwent LVA only were included as a control group. GSVS was performed before LVA in the VL group.
Results:
No significant differences were seen between the groups at baseline. There were no cases indocyanine green (ICG) lymphography pattern deteriorated after GSVS. No significant difference was seen in lymphatic detection rate; 129.71% ± 58.27% (67%–333%) in the VL group and 122.27% ± 39.47% (50%–250%) in the L group (p = 0.59 > 0.05), respective lymphatic diameters 0.66 ± 0.13 (0.45–0.9) mm and 0.75 ± 0.17 (0.45–1.0) mm (p = 0.07 > 0.05), and respective lymphedema improvement rate 12.17% ± 7.35% (0%–27.4%) and 12.65% ± 7.43% (3.7%–22.3%) (p = 0.86 > 0.05).
Discussion:
In this study, stripping surgery does not cause lymphatic impairment, at least to the extent that would impede the success of an LVA procedure. Comorbid varicose veins and lymphedema can be treated surgically by a combination of LVA and GSVS.
Introduction
The exact prevalence of coexisting varicose veins and lymphedema is unknown; however, according to expert opinion and our anecdotal experience, this comorbidity is common. 1 Treatment for patients with comorbid lymphedema and varicose veins is controversial.2–9 Surgical options for these patients are limited, and decongestive physiotherapy is still recommended. 1 However, it has been also reported that surgical treatment of varicose veins has the possibility to normalize lymphatic function, 10 although there is still some reluctance to perform this surgery in patients with lymphedematous comorbidity.2,7–9 Moreover, lymphovenous anastomosis (LVA) is now becoming popular alternatives. 11
This study was aimed to investigate the status of the lymphatics after varicose vein stripping by intraoperative observation under a microscope and the effect of combined LVA and great saphenous vein stripping (GSVS) for comorbid lymphedema and varicose veins.
Methods
The study involved 13 patients (with 21 edematous lower limbs with coexisting varicose veins and lymphedema; the varicose vein and lymphedema [VL] group) who underwent combined GSVS and LVA therapy at our institution between May 2017 and December 2018. Fifteen patients (with 30 edematous lower limbs and lymphedema only; the lymphedema [L] group) who underwent LVA only during the study period were included as a control group to compare the impact of GSVS on the lymphatic vessels. GSVS was performed before LVA in the VL group. Inclusion criteria were no history of a major invasive procedure to treat pelvic cancer and the lower limbs, including radiation therapy, deep vein thrombosis, venous obstruction, renal failure, liver cirrhosis, heart failure, hypoproteinemia, thyroid dermopathy, other endocrine cause of edema, or drug-induced edema; International Society of Lymphology (ISL) stage I–II 12 ; body mass index (BMI) <35; edema onset after the age of 25 years to exclude congenital lymphovenous malformation; and edema refractory to compression therapy using elastic stockings. There were no cases of generalized lymphedema, venous, and/or arterial malformation. No patients had a family history of lymphedema. All the patients have the ability of ambulatory without the need for auxiliary aid or support.
The study protocol was approved by our institutional review board (approval number: E-1413). The study was conducted in accordance with the declaration of Helsinki and the STROBE guidelines (http://www.strobe-statement.org/). All study participants provided written informed consent.
Indocyanine green lymphography procedure
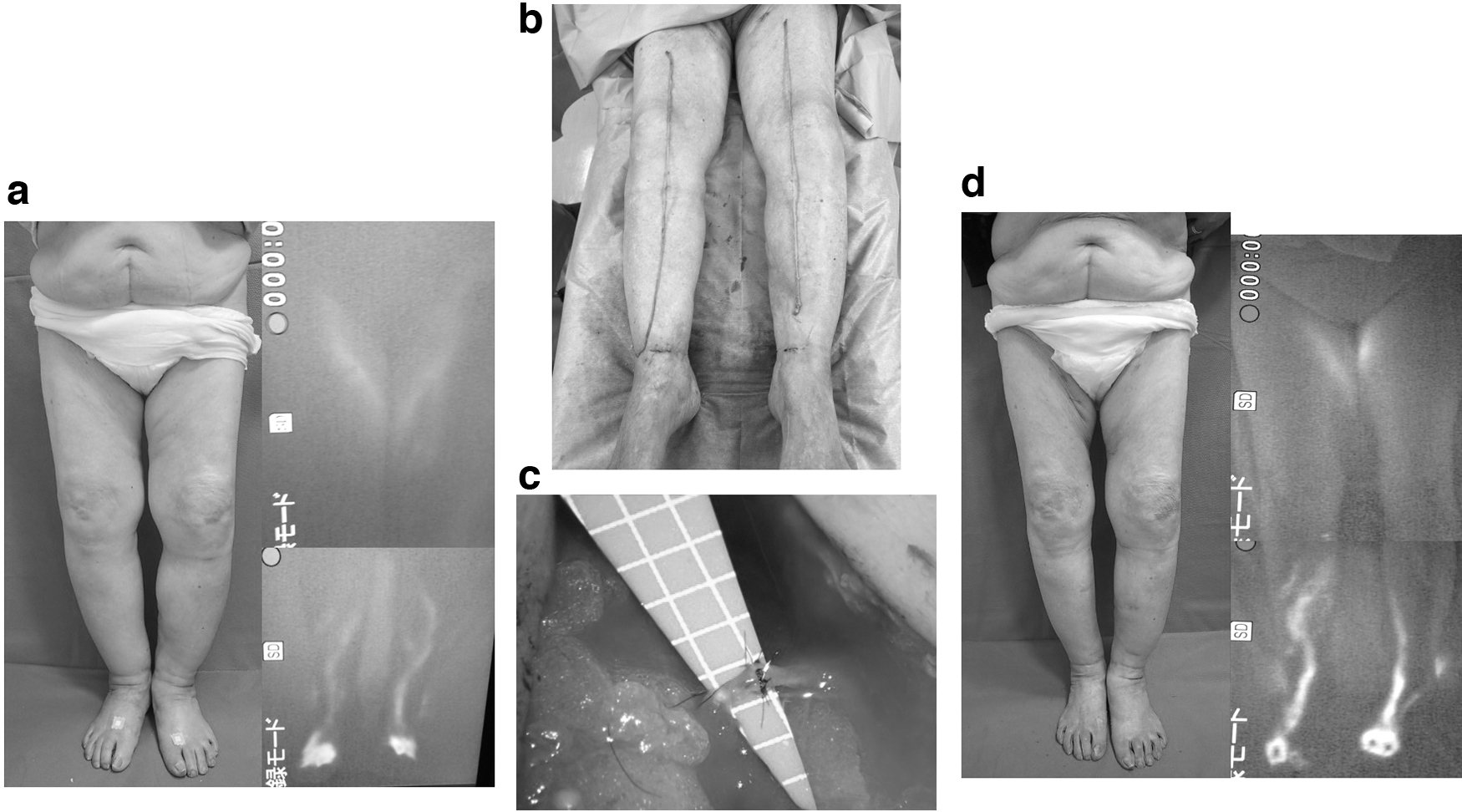
Indocyanine green (ICG) lymphography was performed preoperatively to confirm the diagnosis and severity of lymphedema and to determine the transit time as follows. First, 0.2 mL ICG (Diagnogreen 0.25%; Daiichi Sankyo, Tokyo, Japan) was injected subcutaneously into the lateral side of the Achilles tendon and the first web space of the foot each lower extremity. Circumferential ICG images were then observed using a Photodynamic Eye® system (Hamamatsu Photonics K.K., Hamamatsu, Japan). Next, transit time was measured by taking the time for the dye to reach the inguinal lymph nodes to investigate lymphatic function.13,14 Lymphatic function was judged as impaired if ICG could not reach the groin within 1 hour in spite of acceleration of lymphatic flow by placing the patient in the supine position and instructing them to perform skeletal muscle movements and the patients were categorized as lymphedema. 15 To investigate the severity of lymphedema, ICG images in the plateau phase were recorded (i.e., 12–18 hours after injection) (Fig. 1a). Two plastic surgeons working independently reviewed all ICG lymphography images. The lymphography patterns were then categorized according to clinical characteristics and patients' demographic.
Color Doppler ultrasonography
To diagnose varicose veins, duplex ultrasonography was performed using a 7.5-MHz transducer (Noblus™; Hitachi Aloca, Tokyo, Japan) in the standing position. The saphenous venous system, including varicose tracts and its junctions, was identified and checked for nonsaphenous reflux. Reflux was defined as a reverse flow for >0.5 second after a provocation maneuver. Patients with deep vein thrombosis or reflux in the deep vein (superficial femoral or popliteal) were excluded.
The varicose veins were graded according to the revised Clinical-Etiology-Anatomy-Pathophysiology (CEAP) classification. 16
Treatment
Great saphenous vein stripping
All GSVS procedures were performed under spinal anesthesia (Fig. 1b). The tributaries at the saphenofemoral junction were ligated and divided and the great saphenous vein was dissected. GSVS was then performed after performing tumescent local anesthesia for minimizing bleeding. No sclerotherapy was performed perioperatively. To prevent postoperative hemorrhage, compression for 1 night was performed. Compression therapy was resumed immediately after GSVS. Approximately 2–6 months were allowed for the effect of stripping, such as hardening of soft tissue, to resolve completely before LVA was performed in the VL group.
LVA procedure
After the ICG lymphography results became available, LVA was performed along the course of the great saphenous vein based on our experience when no enhancement or a dermal backflow (DB) pattern were seen by ICG lymphography; or LVA was performed exactly where a linear pattern was seen. All LVAs were performed under local anesthesia. After making several 1–5-cm skin incisions, subcutaneous tissue was dissected in search for suitable lymphatic vessels and the subcutaneous veins for anastomosis. After identifying suitable lymphatic vessels and veins, the anastomosis was performed in an end-to-side or end-to-end manner with 11-0 or 12-0 microsutures (Fig. 1c). Compression was resumed 1 week after LVA surgery in the same manner as that before LVA.
Demographic and clinical characteristics
The demographic and clinical characteristics compared were as follows: age at LVA (years), age at onset of lymphedema (years), duration of edema (years), BMI, sex ratio, lower extremity lymphedema (LEL) index before treatment, 17 ISL score, 12 ICG lymphography pattern, number of incisions, number of detected lymphatics, lymphatic detection rate (%), diameter of lymphatics (mm), classification of the types of collecting lymphatic vessels, and the macroscopic anatomical findings (NECST classification: Normal type, Ectasis type, Contraction type, and Sclerosis type), which has been described elsewhere, 18 and the improvement rate of lymphedema.
LEL index
The LEL index of the limb was calculated before and after the LVA. Circumferential length was measured at five locations (foot, ankle, 10 cm below the knee, knee, and 10 cm above the knee) in the supine position. Next, the sum of the squares of each circumferential length was calculated. The sum was divided by the BMI, which was the LEL index. 17 Tape measurements were performed by a nurse not involved in the research and randomly assigned to patients to reduce the measurement bias.
Diameter of lymphatics
The diameter of each identified lymphatic vessel was measured using a Crownjun Microscale (Kono Seisakusyo Co., Ltd., Ichikawa, Japan) during the LVA procedure. Mean values for lymphatic vessel diameter in each lower limb were calculated.
Lymphatic detection rate
The numbers of lymphatic vessels detected and the numbers of skin incisions required during the LVA procedure in each lower limb were recorded. The number of lymphatics detected was normalized by the number of skin incisions for each lower limb to calculate the detection rate as follows: [(number of detected lymphatics)/(number of skin incisions)] × 100.
Lymphedema improvement rate
Differences in the LEL index between, before, and after surgery were normalized by the preoperative score for each case to calculate improvement rate as follows: ([preoperative LEL index] − [postoperative LEL index])/(preoperative LEL index) × 100.
Sclerosis and fibrosis of lymphatic vessels
We categorized the macroscopic findings observed under the operating microscope using the NECST classification, 18 recorded the numbers of lymphatics in each grade category for each limb, and compared the findings between the groups (Table 1).
Classification of Types of Collecting Lymphatic Vessels and Macroscopic Anatomical Findings
NECST, Normal, Ectasis, Contraction, and Sclerosis Type.
Statistical analysis
Data are shown as the mean and standard deviation (range) or number (percentage) as appropriate. Differences in age, age at onset, duration of edema, BMI, LEL index before treatment, number of incisions, number of detected lymphatics, lymphatic detection rate, diameter of lymphatic vessels, and lymphedema improvement rate were compared by the Student's t-test. The sex ratio, ICG lymphography patterns, ISL staging, and distribution of NECST grades were compared between the groups using the chi-square for independence test. All statistical analyses were performed by Statcel 4 software (OMS Publishing, Inc., Tokyo, Japan). A p-value <0.05 was considered statistically significant.
Results
All surgical procedures were performed uneventfully. There were no complications, such as delayed wound healing, lymphorrhea, or saphenous nerve palsy (Fig. 1d). Clinical status was graded in the VL group using the revised CEAP classification 16 ; 17 of the 21 lower limbs were assessed as class 3 and 4 as class 4a (Table 2).
Clinical Status in the Varicose Vein and Lymphedema Group Graded Using the Revised Clinical-Etiology-Anatomy-Pathophysiology Classification
CEAP, Clinical-Etiology-Anatomy-Pathophysiology; VL group, the varicose vein and lymphedema group.
Based on the ISL scoring system, 16 legs in the VL group had stage I lymphedema and 5 had stage II, whereas 22 legs in the L group had stage I lymphedema and 8 had stage II (p = 0.82 > 0.05). No significant between-group difference was seen in the ISL scores.
No significant differences were seen in the following parameters between the VL group and the L group at baseline: mean age at the time of LVA (77.70 ± 8.08 [range 58–90] years vs. 75.4 ± 9.25 [59–95] years, respectively, p = 0.49 > 0.05); mean age at onset of edema (75.23 ± 8.18 [55–88] years vs. 72.13 ± 10.21 [58–93] years, p = 0.39 > 0.05); duration of edema (2.69 ± 1.60 [1–5] years vs. 3.27 ± 3.03 [1–10] years, p = 0.55 > 0.05); BMI (24.47 ± 2.1 [21.52–28.95] vs. 26.84 ± 4.01 [21.63–34.22], p = 0.07 > 0.05); LEL index before treatment (220.08 ± 33.31 [156–266] vs. 214.87 ± 25.22 [177–254], p = 0.64 > 0.05); and sex distribution (10 women and 3 men vs. 8 women and 7 men, p = 0.19 > 0.05; Table 3).
Demographic and Clinical Characteristics at Baseline
Data are shown as the mean and standard deviation (range) or number (percentage) as appropriate.
BMI, body mass index; ISL, International Society of Lymphology; L group, the lymphedema group; LEL, lower extremity lymphedema; LVA, lymphovenous anastomosis.
There was no significant difference between the VL group and the L group in the number of skin incisions (3.36 ± 1.09 [1–6] vs. 3.3 ± 1.18 [2–6], respectively, p = 0.84 > 0.05) or in the number of lymphatics detected (4.29 ± 1.93 [1–10] vs. 3.97 ± 1.79 [2–9], p = 0.55 > 0.05) during the LVA procedure. All detected lymphatics were anastomosed with veins. The number of detected lymphatics was the same as the number of established LVAs. Therefore, the ratio of established LVA to the number of skin incisions was equal to the detection rate of lymphatics. The lymphatic detection rate was 129.71% ± 58.27% (67%–333%) in the VL group and 122.27% ± 39.47% (50%–250%) in the L group (p = 0.59 > 0.05); and respective lymphatic diameters were 0.66 ± 0.13 (0.45–0.9) mm and 0.75 ± 0.17 (0.45–1.0) mm (p = 0.07 > 0.05; Table 4).
The Investigation Results During Lymphovenous Anastomosis Procedures
The data are shown as the mean and standard deviation (range).
No significant difference was seen in the improvement rate of lymphedema after LVA between the VL group (12.17% ± 7.35% [0%–27.4%]) and L group (12.65% ± 7.43% [3.7%–22.3%], p = 0.86 > 0.05; Fig. 2).
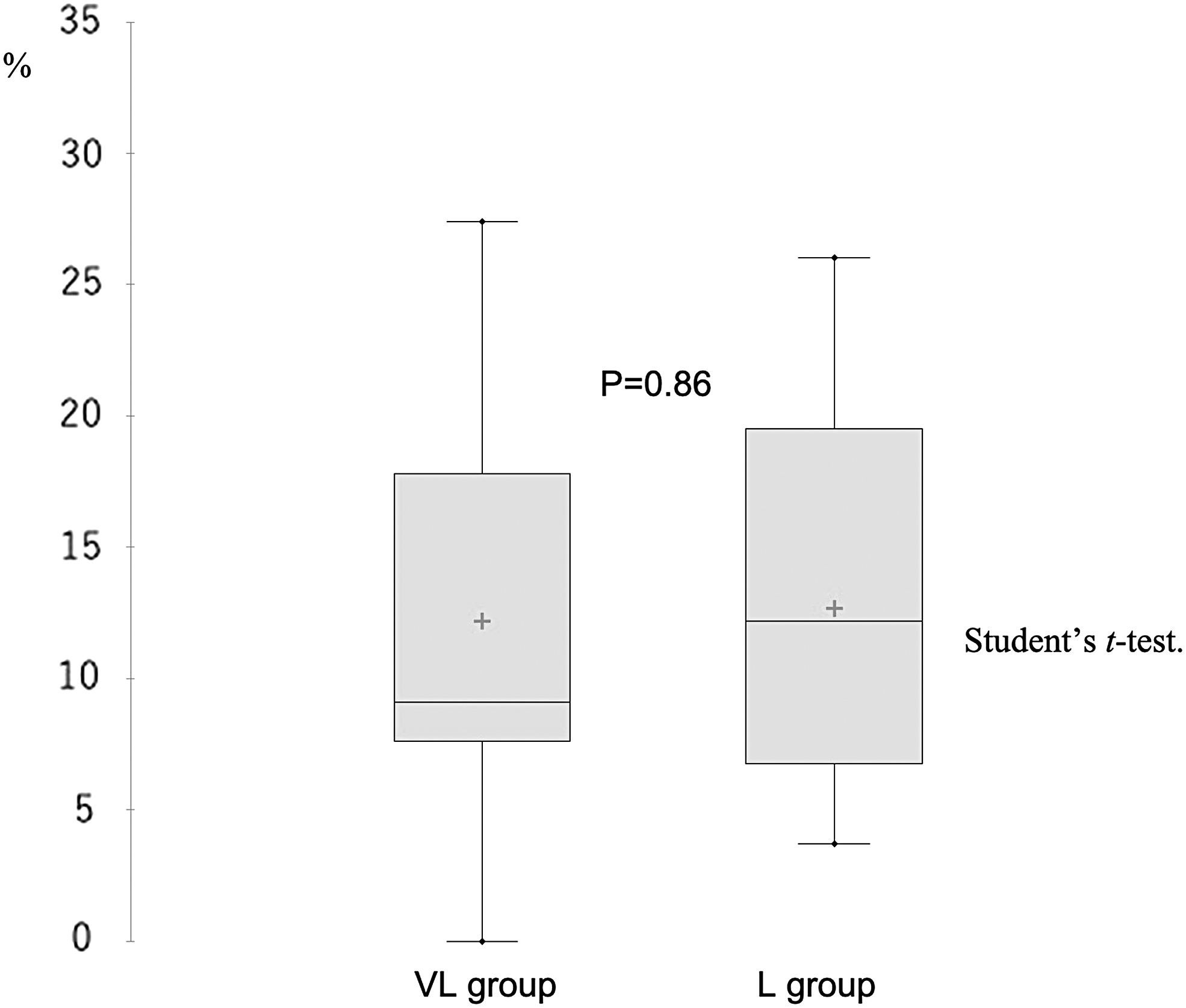
Comparison of the lymphedema improvement rate between the two groups. There was no significant difference in the lymphedema improvement rate after LVA between the VL group (12.17% ± 7.35% [0%–27.4%]) and L group (12.65% ± 7.43% [3.7%–22.3%]), p = 0.86 > 0.05. L group, the lymphedema group; VL group, the varicose vein and lymphedema group.
The ICG pattern was interpreted as linear, DB, or low enhancement (LE). The pattern was regarded as linear when seen in a linear manner from the foot to the superficial inguinal region (Fig. 3). The LE pattern was that enhancement was observed only around the foot with no pattern in the proximal part (Fig. 3). The pattern was deemed to be DB when diffuse pattern was seen in the proximal portion to the ankle (Fig. 3). No difference was seen between the two independent observers in the ICG patterns categorization.

Linear: the superficial lymphatic vessels were seen to be arranged in a linear manner from the injection site to the superficial inguinal lymph nodes. LE: the pattern observed only in the distal portion of the lower extremity around the ankle joint with no enhancement in the proximal part or DB pattern observed. DB: the pattern deterioration was visible in the enhanced lymphatics. DB, dermal backflow; LE, low enhancement.
The linear pattern was seen in 18 legs, the LE pattern in 1 leg, and the DB pattern in 2 legs in the VL group. There were no cases in which the DB pattern appeared or deteriorated after GSVS. All 30 legs in the L group were categorized as showing the linear pattern. No significant between-group difference was seen in the ICG lymphography pattern ratio (p = 0.10 > 0.05; Fig. 4).
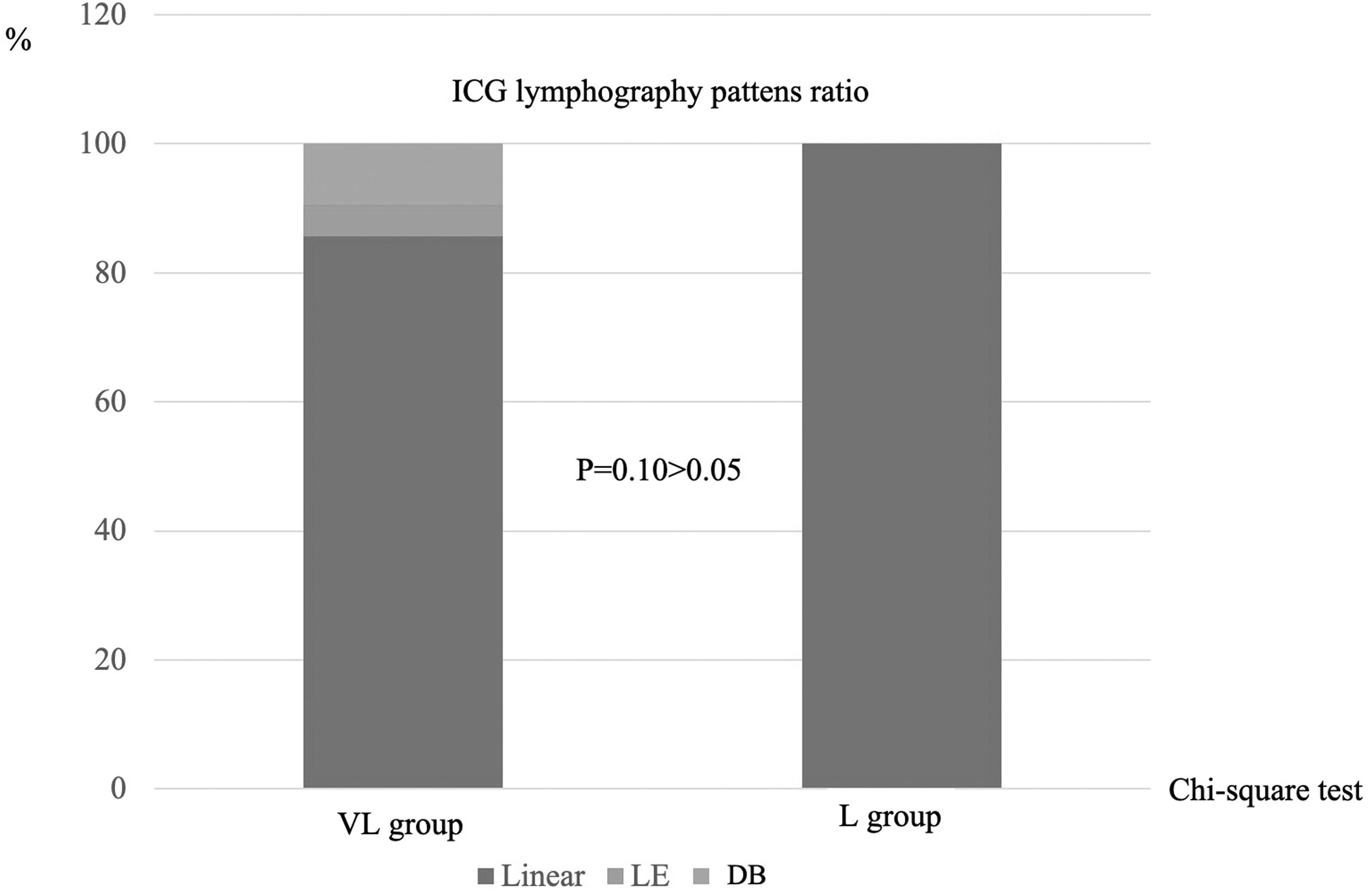
ICG lymphography pattern ratio. VL group: the linear pattern; 18 legs, the LE pattern; 1 leg, the DB pattern; 2 legs. L group: the linear pattern; all the 30 legs. There was no significant difference in ICG lymphography patters ratio between groups, p = 0.10 > 0.05.
Based on the NECST classification, 90 lymphatic vessels were detected in the VL group; 33 (36.7%) were classified as normal, 51 (56.7%) as ectasia, and 6 (6.6%) as contraction. A total of 119 lymphatics were detected in the L group, 20 (16.8%) of which were classified as normal, 80 (67.2%) as ectasia, and 19 (16.0%) as contraction. There were no sclerosis-type lymphatics in either group. A significant between-group difference was seen in the distribution (p = 0.001 < 0.01; Fig. 5).
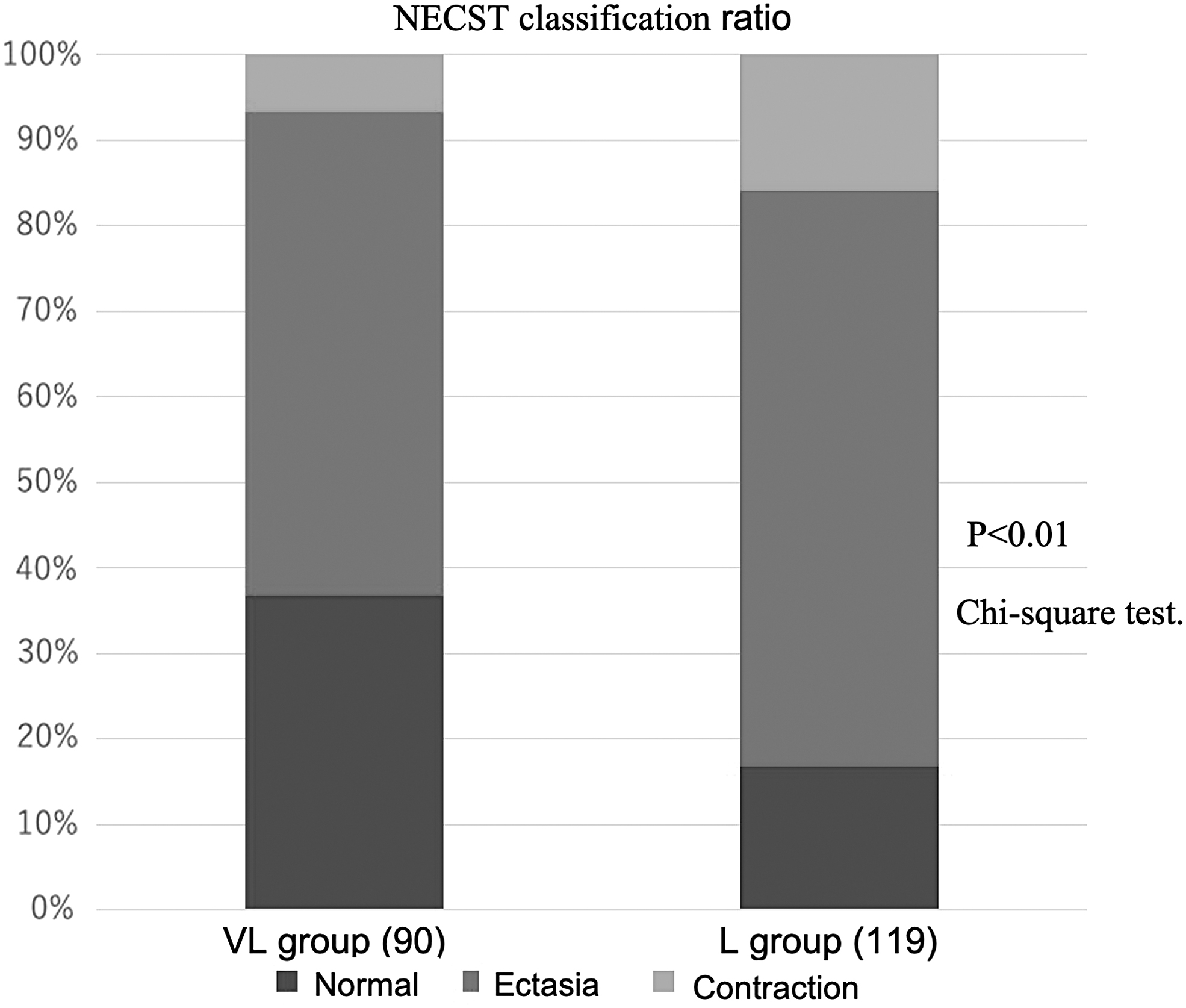
VL group, 90 lymphatics were detected. Normal; 33(36.7%) lymphatic, ectasia; 51 (56.7%) lymphatics, contraction; 6 (6.6%) lymphatics. L group, 119 lymphatics were detected. Normal; 20 (16.8%) lymphatics, ectasia; 80 (67.2%) lymphatics, contraction; 19 (16.0%) lymphatics. There was a significant difference in the distribution, p = 0.001 < 0.01. NECST, Normal, Ectasis, Contraction, and Sclerosis Type.
Discussion
The two groups were enrolled by the same inclusion criteria with no significant between-group differences at baseline, so the severity of lymphedema in the groups could be assumed to be similar. Consequently, the L group was regarded suitable as a control group against which to compare the impact of GSVS on lymphatics and the results of combined treatment of LVA and GSVS.
GSVS is still frequently used treatment for great saphenous vein incompetence. 19 However, there is some concern about the invasiveness of stripping and some to lymphatic-related complications have been reported,3–7 although the risk of long-lasting sequelae is low.2,7–9 Therefore, there is some reluctance to perform stripping in patients with lymphedema. However, in this study, we found no significant difference in the ICG lymphography pattern ratio, deterioration of lymphography pattern, lymphatic detection rate, number of lymphatics detected, or rate of establishment of LVA between the VL group and L group. Therefore, it appears that stripping surgery does not cause lymphatic impairment, at least to the extent that would impede the success of an LVA procedure. We found that the improvement rate was the same in the two groups, indicating that comorbid varicose veins and lymphedema can be treated surgically by a combination of LVA and GSVS.
Furthermore, although the patient profiles and severity of lymphedema were very similar in the two groups, the lymphatic status in the VL group was significantly better than that in the L group according to the NECST classification findings during LVA. This finding indicates that varicose vein stripping has the potential to reduce the burden of lymphedema in patients with coexisting lymphedema and varicose veins.
The association between pathogenesis of lymphatic impairment and chronic venous dysfunction is still uncertain.20,21 A more profound investigation on the phlebolymphology is necessary. Phlebolymphedema is an insufficient status involving a mixture of venous and lymphatic impairment. 22 The flow of lymph can be tripled by venous hypertension caused by venous dysfunction, and its concentration of fibrinogen can be doubled, thereby which leads to increasing fibrinogen net transport across the interstitial space by 600%. 23 However, the fibrinolytic activity of lymph does not change significantly. Therefore, the deposition of fibrin in the tissues is increased significantly under phlebolymphedema condition. The deposition of fibrin around the capillaries leads to blocking of oxygen diffusion. Furthermore, the blocking of oxygen diffusion leads to tissue fibrosis that is manifests as lipodermatosclerosis and necrosis, that is, a venous ulcer. 23 The phlebolymphedema condition induces degeneration of adipocytes at that site, which leads to inflammation of the vein. 22 Excessive production of fibrous matter is caused by this inflammation, which in turn leads to hyperplasia of fibrous tissue, and reduces the elasticity of the vein.24,25 Therefore, venous insufficiency might contribute to lymphatic deterioration. 26 Furthermore, apoptosis of the cells of the lymphatic vasculature has been thought to be caused by sustained inflammation. There is a close relationship between the venous functions and lymphatic systems, and if the function of one declines, the other will also be deteriorated. Therefore, a vicious cycle occurs between lymphatic impairment and venous dysfunction. Venous treatment, including stripping surgery, may be useful for cutting off the vicious cycle between lymphatic impairment and venous dysfunction.
In this series, varicose vein stripping was performed before LVA because we thought it would be difficult to perform stripping surgeries for varicose veins without damaging established LVA. Furthermore, venous insufficiency is a progressive disease, 27 so radical surgical treatment 28 is suitable for the combined treatment of lymphedema and varicose veins.
This study has some limitations. Although it may have been preferable to include a control group that consisted of patients with coexisting lymphedema and varicose veins in whom only LVA was performed, we did not have a surgical option for varicose veins after establishing LVA. Therefore, the control group consisted of patients with lymphedema only. Another limitation of this study is that functional changes were not investigated, such as internal pressure in the lymphatic and venous systems. In addition, lacking information of lymphatic status before GSVS may be another study limitation, because venous insufficiency itself causes inflammation and affect lymphatics nearby.22–26 Other limitations are the small number of cases and short investigation period. Future studies should include larger numbers of cases and longer follow-up durations.
Conclusion
Stripping surgery does not cause lymphatic impairment, at least to the extent that would impede the success of an LVA procedure. Comorbid varicose veins and lymphedema can be treated surgically by a combination of LVA and GSVS.
Footnotes
Authors' Contributions
Conception, design, and statistical analysis by S.Yo., I.K., H.M., and S.Ya. Analysis and interpretation, critical revision and final approval of the article by S.Yo., I.K., H.I., T.U., A.S., Y.F., S.N., K.Y., H.M., and S.Ya. Data collection by S.Yo., I.K., H.I., T.U., A.S., Y.F., S.N., and K.Y. Writing of the article by S.Yo.
Author Disclosure Statement
None of the authors have financial interest in any of the products, devices, or drugs mentioned in this article.
Funding Information
No funding was received for this article.