
Abstract
Highlighted Articles
Rodriguez-Laguna, L., et al. (2019). “Somatic activating mutations in PIK3CA cause generalized lymphatic anomaly.” J Exp Med 216(2): 407–418.
Generalized lymphatic anomaly (GLA) is a vascular disorder characterized by diffuse or multifocal lymphatic malformations (LMs). The etiology of GLA is poorly understood. We identified four distinct somatic PIK3CA variants (Glu542Lys, Gln546Lys, His1047Arg, and His1047Leu) in tissue samples from five out of nine patients with GLA. These same PIK3CA variants occur in PIK3CA-related overgrowth spectrum and cause hyperactivation of the PI3K-AKT-mTOR pathway. We found that the mTOR inhibitor, rapamycin, prevented lymphatic hyperplasia and dysfunction in mice that expressed an active form of PIK3CA (His1047Arg) in their lymphatics. We also found that rapamycin reduced pain in patients with GLA. In conclusion, we report that somatic activating PIK3CA mutations can cause GLA, and we provide preclinical and clinical evidence to support the use of rapamycin for the treatment of this disabling and deadly disease.
This manuscript summarizes the challenges in what can be a devastating clinical condition, Generalized Lymphatic Anomaly (GLA), a multifocal lymphatic disorder. Although patients with GLA have previously been reported to respond to m-Tor inhibitor therapy, this is the first documentation of an underlying causative somatic activating mutation in the PIK3CA pathway in this disorder. These mutations (in 4 mutations were identified in the tissue samples from 5/9 patients) have been identified in other patients whose diseases fall into the rubric of PROS (PIK3CA-related overgrowth spectrum). The authors of this highlighted manuscript are to be complimented on the 1) thorough review of this disease, 2) investigation of the clinical specimens (lymphatic malformation tissue as well as lymphatic endothelial cells from those samples), confirming the mutation is postzygotic/somatic (i.e., the mutation was present in affected tissue, not blood samples of the patients), and 3) convincing data provided by developing and analyzing an model representing and ameliorating the lymphatic dysfunction. A mouse model harboring the PIK3CA H1047R mutation recapitulated the lymphatic function seen in bones and many developed chylous effusions (see Figure below). Pre-treatment at day P43–P70 with Rapamycin (which is clinically beneficial in affected patients) prevented the lymphatic dysplasia in PIK3CA H1047R mice, and Rapamycin treatment partially restored lymphatic dysfunction in diseased PIK3CA H1047R mice.
Rodriguez-Laguna, L., et al. “Somatic activating mutations in PIK3CA cause generalized lymphatic anomaly.” 2019. J Exp Med 216(2): 407–418.
Basic Science
Amamizu, H., et al. (2019). “Cardiac Lymphatic Dysfunction Causes Drug-Eluting Stent-Induced Coronary Hyperconstricting Responses in Pigs In Vivo.” Arterioscler Thromb Vasc Biol: ATVBAHA119312396. [EPub Feb 28]
Objective- We have previously demonstrated that coronary adventitial inflammation plays important roles in the pathogenesis of coronary vasomotion abnormalities, including drug-eluting stent (DES)-induced coronary hyperconstricting responses. Importantly, the adventitia also harbors lymphatic vessels, which may prevent inflammation by transporting extravasated fluid and inflammatory cells. We thus aimed to examine the roles of coronary adventitial lymphatic vessels in the pathogenesis of DES-induced coronary hyperconstricting responses in a porcine model in vivo. Approach and Results- We performed 2 experimental studies. In protocol 1, 15 pigs were divided into 3 groups with or without DES and with bare metal stent. Nonstented sites 20 mm apart from stent implantation also were examined. In the protocol 2, 12 pigs were divided into 2 groups with or without lymphatic vessels ligation followed by DES implantation at 2 weeks later (n = 6 each). We performed coronary angiography 4 weeks after DES implantation, followed by immunohistological analysis. In protocol 1, the number and the caliber of lymphatic vessels were greater at only the DES edges after 4 more weeks. In protocol 2, coronary hyperconstricting responses were further enhanced in the lymphatic vessels ligation group associated with adventitial inflammation, Rho-kinase activation, and less adventitial lymphatic vessels formation. Importantly, there were significant correlations among these inflammation-related changes and enhanced coronary vasoconstricting responses. Conclusions- These results provide evidence that cardiac lymphatic vessel dysfunction plays important roles in the pathogenesis of coronary vasoconstrictive responses in pigs in vivo.
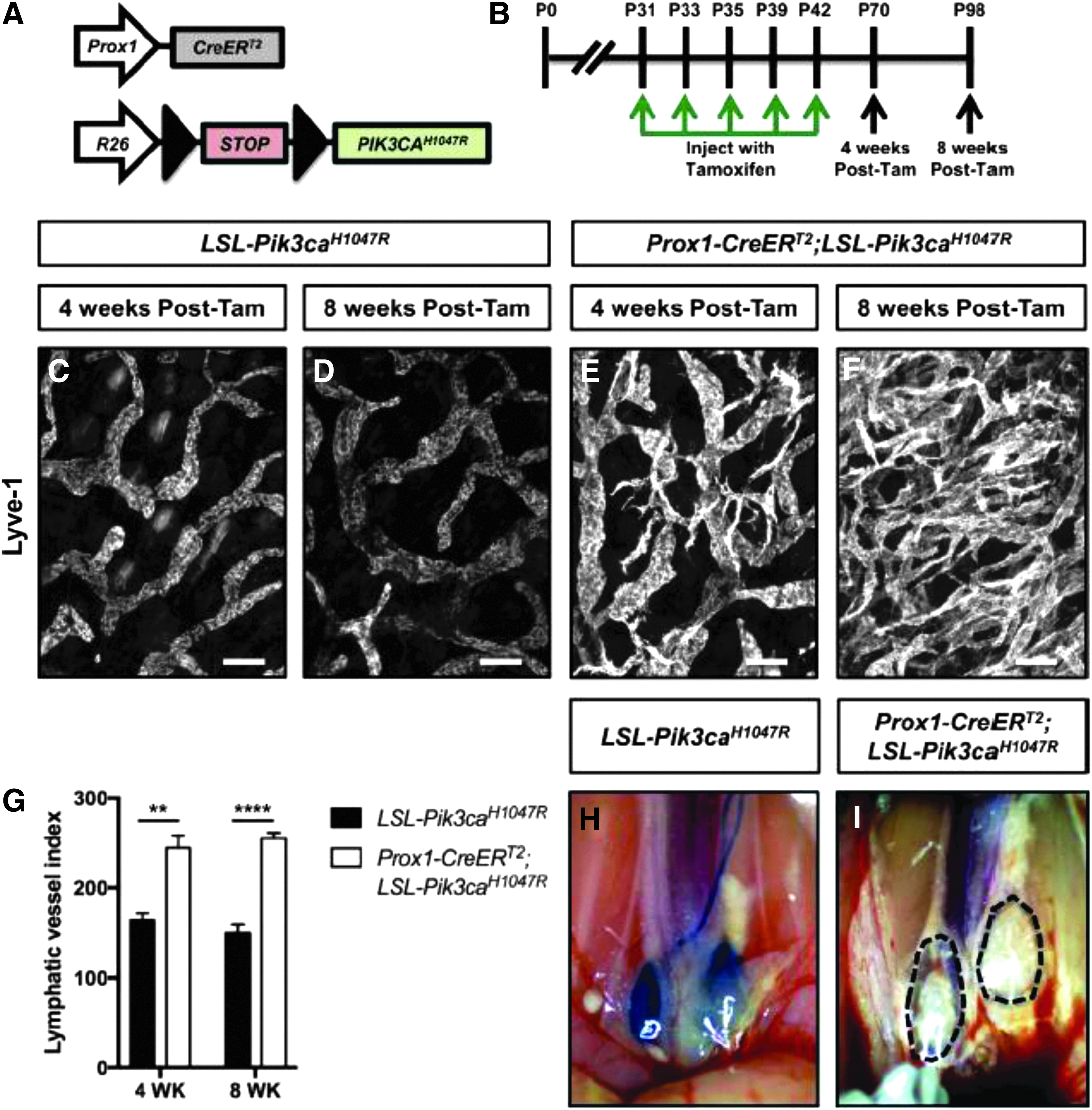
Expression of Pik3caH1047R in LECs causes lymphatic hyperplasia and dysfunction.
Bota, M., et al. (2019). “Combined effect of propranolol, vincristine and bevacizumab on HUVECs and BJ cells.” Exp Ther Med 17(1): 307–315.
Infantile hemangioma is one of the most common benign tumors affecting children, with ∼10–15% requiring medical treatment. These tumors consist of endothelial cells and stromal components, including fibroblasts, pericytes and mast cells. Effects of propranolol treatment in combination with bevacizumab or vincristine on cell growth were compared in the current study using human umbilical vein endothelial cells (HUVECs) and BJ human normal fibroblasts (BJs) to determine potential synergic effects in vitro. Inhibition of cell growth was investigated using MTT assays and cytotoxicity of the drugs in various combinations was expressed as half inhibitory concentration (IC50). Apoptosis was investigated using flow cytometry, with Alexa Fluor 488 and propidium iodide. Propranolol inhibited BJ and HUVEC growth in a dose-dependent manner, with increased response observed in BJs (IC50, 148,32 microg/ml; standard error logIC50, 0.07). Treatment with vincristine induced the strongest growth inhibition in HUVECs (IC50, 17,89 microg/ml; standard error log IC50, 0.07) and BJs (IC50, 24,81 microg/ml; standard error log IC50, 0.08) compared with propranolol (HUVEC IC50, 81,94 microg/ml; standard error log IC50, 0.06; BJ-IC50, 148,32 microg/ml; standard error logIC50, 0.07) or bevacizumab (HUVEC IC50 96,91 microg/ml; standard error log IC50, 0.06; BJ IC50, 182,70 microg/ml; standard error log IC50, 0.09) alone. Bevacizumab was the weakest cytotoxic agent. Combination treatment of vincristine with bevacizumab induced the highest levels of apoptosis in HUVECs compared with all other treatments and triple-drug therapy induced the levels of apoptosis in BJs. Single treatment with vincristine, propranolol or bevacizumab induced apoptosis in BJs and HUVECs. In BJs, triple treatment exhibited the greatest influence on apoptosis, compared with single and dual treatments and in HUVECs, vincristine and bevacizumab combination treatment induced apoptosis to the highest level. The present study offers novel perspectives in drug repurposing studies for the three drugs, particularly in diseases where the pathogenesis is based on healthy endothelial cell proliferation, including hemangiomas.
Cho, H., et al. (2019). “YAP and TAZ Negatively Regulate Prox1 During Developmental and Pathologic Lymphangiogenesis.” Circ Res 124(2): 225–242.
RATIONALE: The Hippo pathway governs cellular differentiation, morphogenesis, and homeostasis, but how it regulates these processes in lymphatic vessels is unknown. OBJECTIVE: We aimed to reveal the role of the final effectors of the Hippo pathway, YAP (Yes-associated protein) and TAZ (transcriptional coactivator with PDZ-binding motif), in lymphatic endothelial cell (LEC) differentiation, morphogenesis, and homeostasis. METHODS AND RESULTS: During mouse embryonic development, LEC-specific depletion of Yap/Taz disturbed both plexus patterning and valve initiation with upregulated Prox1 (prospero homeobox 1). Conversely, LEC-specific YAP/TAZ hyperactivation impaired lymphatic specification and restricted lymphatic sprouting with profoundly downregulated Prox1. Notably, lymphatic YAP/TAZ depletion or hyperactivation aggravated or attenuated pathological lymphangiogenesis in mouse cornea. Mechanistically, VEGF (vascular endothelial growth factor)-C activated canonical Hippo signaling pathway in LECs. Indeed, repression of PROX1 transcription by YAP/TAZ hyperactivation was mediated by recruitment of NuRD (nucleosome remodeling and histone deacetylase) complex and endogenous binding activity of TEAD (TEA domain family members) to the PROX1 promoter. Furthermore, YAP/TAZ hyperactivation enhanced MYC signaling and inhibited CDKN1C, leading to cell cycle dysregulation and aberrant proliferation. CONCLUSIONS: We find that YAP and TAZ play promoting roles in remodeling lymphatic plexus patterning and postnatal lymphatic valve maintenance by negatively regulating Prox1 expression. We further show that YAP and TAZ act as plastic regulators of lymphatic identity and define the Hippo signaling-mediated PROX1 transcriptional programing as a novel dynamic checkpoint underlying LEC plasticity and pathophysiology.
Cho, H., et al. (2019). “Long noncoding RNA ANRIL regulates endothelial cell activities associated with coronary artery disease by up-regulating CLIP1, EZR, and LYVE1 genes.” J Biol Chem. [EPub Jan 17]
Coronary artery disease (CAD) is the leading cause of death worldwide. Long noncoding RNAs (lncRNAs) are a class of noncoding transcripts of >200 nucleotides and are increasingly recognized as playing functional roles in physiology and disease. ANRIL is a lncRNA gene mapped to the chromosome 9p21 genetic locus for CAD identified by the first series of genome-wide association studies (GWAS). However, ANRIL's role in CAD and the underlying molecular mechanism are unknown. Here, we show that the major ANRIL transcript in endothelial cells (ECs) is DQ485454 with a much higher expression level in ECs than in THP-1 monocytes. Of note, DQ485454 expression was down-regulated in CAD coronary arteries compared with non-CAD arteries. DQ485454 overexpression significantly reduced monocyte adhesion to ECs, transendothelial monocyte migration (TEM), and EC migration, which are critical cellular processes involved in CAD initiation, whereas siRNA-mediated ANRIL knockdown (KD) had the opposite effect. Microarray and follow-up quantitative RT-PCR analyses revealed that the ANRIL KD down-regulated expression of AHNAK2, CLIP1, CXCL11, ENC1, EZR, LYVE1, WASL, and TNFSF10 genes, and up-regulated TMEM100 and TMEM106B genes. Mechanistic studies disclosed that overexpression of CLIP1, EZR, and LYVE1 reversed the effects of ANRIL KD on monocyte adhesion to ECs, TEM, and EC migration. These findings indicate that ANRIL regulates EC functions directly related to CAD, supporting the hypothesis that ANRIL is involved in CAD pathogenesis at the 9p21 genetic locus and identifying a molecular mechanism underlying lncRNA-mediated regulation of EC function and CAD development.
Choi, D., et al. (2019). “Piezo1 incorporates mechanical force signals to genetic program that governs lymphatic valve development and maintenance.” JCI Insight. [EPub Jan 24]
The lymphatic system plays crucial roles in tissue homeostasis, lipid absorption and immune cell trafficking. While lymphatic valves ensure unidirectional lymph flows, the flow itself controls lymphatic valve formation. Here, we demonstrate that a mechanically activated ion channel Piezo1 senses oscillating shear stress (OSS), and incorporates the signal into the genetic program controlling lymphatic valve development and maintenance. Time-controlled deletion of Piezo1 using a pan-endothelial Cre driver (Cdh5(PAC)-CreERT2) or lymphatic-specific Cre driver (Prox1-CreERT2) equally inhibited lymphatic valve formation in newborn mouse. Furthermore, Piezo1 deletion in adult lymphatics caused substantial lymphatic valve degeneration. Piezo1 knockdown in cultured lymphatic endothelial cells (LECs) largely abrogated the OSS-induced upregulation of the lymphatic valve-signature genes. Conversely, ectopic Piezo1 overexpression upregulated the lymphatic valve genes in the absence of OSS. Remarkably, activation of Piezo1 using a chemical agonist Yoda1 not only accelerated lymphatic valve formation in animals, but also triggered upregulation of some lymphatic valve genes in cultured LECs without exposure to OSS. In summary, our studies together demonstrate that Piezo1 is the force sensor in the mechanotransduction pathway controlling lymphatic valve development and maintenance, and Piezo1 activation is a potential novel therapeutic strategy for congenital and surgery-associated lymphedema.
Cordeiro, A. S., et al. (2019). “Engineering polymeric nanocapsules for an efficient drainage and biodistribution in the lymphatic system.” J Drug Target: 1–52.
Polymer-based nanocarriers have shown potential for enhancing the immunological response of antigens. However, the key drivers for this response have not been fully elucidated. The objective of this work was to evaluate the influence of particle size (approximately 100 vs. 200 nm) and surface composition of polymeric nanocapsules (chitosan, polyarginine and carboxymethyl-beta-glucan) on their ability to target specific immune cells in the lymphatics. For this purpose, we used a powerful imaging technique, two-photon intravital microscopy, which minimizes tissue damage in the visualization of biological processes at cellular/subcellular levels. As expected, particle size was critical in the distribution and lymph node accumulation of all nanocapsules. Chitosan particles with a mean size below 100 nm accumulated significantly more in the popliteal lymph node than those with a larger size. Additionally, a comparative analysis of 100 nm nanocapsules with different polymeric shells indicated that cationic nanocapsules (chitosan and polyarginine) show higher accumulation in the popliteal lymph node than the anionic ones (carboxymethyl-beta-glucan). In contrast, these anionic nanocapsules showed significant accumulation in the lumbar lymph node. In conclusion, tuning the physicochemical properties and composition of the nanocapsules allows the modulation of their lymphatic uptake and biodistribution, which may have important implications in the immune response.
Dando, S. J., et al. (2018). “Regional and functional heterogeneity of antigen presenting cells in the mouse brain and meninges.” Glia. [EPub Dec 26]
The central nervous system (CNS) is considered to be immune privileged, owing in part to the absence of major histocompatibility (MHC) class II(+) cells in the healthy brain parenchyma. However, systemic inflammation can activate microglia to express MHC class II, suggesting that systemic inflammation may be sufficient to mature microglia into functional antigen presenting cells (APCs). We examined the effects of systemic lipopolysaccharide (LPS)-induced inflammation on the phenotype and function of putative APCs within the mouse brain parenchyma, as well as its supporting tissues-the choroid plexus and meninges. Microglia isolated from different regions of the brain demonstrated significant heterogeneity in their ability to present antigen to naive OT-II CD4(+) T cells following exposure to systemic LPS. Olfactory bulb microglia (but not cortical microglia) intimately interacted with T cells in vivo and stimulated T cell proliferation in vitro, albeit in the absence of co-stimulation. In contrast, myeloid cells within the choroid plexus and meninges were immunogenic and upregulated the co-stimulatory molecule CD80 following systemic inflammation. Dural APCs, which clustered around LYVE-1(+) lymphatics, were more efficient at stimulating naive T cell proliferation than choroid plexus APCs, suggesting that the dura may be an under-appreciated site for immune interactions. This study has highlighted the functional diversity of myeloid cells within the sub-compartments of the CNS and its supporting tissues. Furthermore, these findings demonstrate that systemic inflammation can mature selected microglia populations and choroid plexus/meningeal myeloid cells into functional APCs, which may contribute to the pathogenesis of neuroinflammation and neurodegenerative diseases.
Ferrao, J. S. P., et al. (2019). “Vascular endothelial growth factor C treatment for mouse hind limb lymphatic revascularization.” Vet Med Sci. [EPub Feb 11]
Spontaneous lymphatic revascularization is a challenge and the establishment of new therapeutic strategies may improve life quality for patients suffering from lymphatic disorders. This study was designed to verify if VEGFC treatment improves lymphatic vascularization in a time-dependent manner in mouse hindlimb (HL) after resection of the inguinal lymph node. Lymphatic vascular density (Vv) and length (Lv) were evaluated by stereology after immunohistochemistry. The control Group (CG) was not manipulated but received saline instead of VEGFC treatment. The surgery Group (SG) had the left inguinal lymph node resected but did not received VEGFC treatment. VEGFC Treated Group (TG) had the node resected and received VEGFC treatment. VEGFC and VEGFR3 local expression were assessed by qPCR. There was an effect of time over Vv and Lv in the SG and significant difference between CG and SG in the regions studied (proximal, medium and distal regions) of the left HL (LHL). The Lv showed significant difference between CG and SG only in the medium region. The Vv and the Lv for TG were higher than the other groups. VEGFC and VEGFR3 gene expression presented time effect in all regions of the LHL for SG and TG. Both VEGFC and VEGFR3 gene expression presented significant difference between CG and SG, between SG and TG and between CG and TG. This study showed significant decrease in lymphatic vascularization in the left hindlimb of mice after surgical removal of the inguinal lymph node and adjacent lymphatic vessels. Exogenous VEGFC could recover lymphatic vascularization through stimulating neolymphangiogenesis.
Hsu, M., et al. (2019). “Neuroinflammation-induced lymphangiogenesis near the cribriform plate contributes to drainage of CNS-derived antigens and immune cells.” Nat Commun 10(1): 229.
There are no conventional lymphatic vessels within the CNS parenchyma, although it has been hypothesized that lymphatics near the cribriform plate or dura maintain fluid homeostasis and immune surveillance during steady-state conditions. However, the role of these lymphatic vessels during neuroinflammation is not well understood. We report that lymphatic vessels near the cribriform plate undergo lymphangiogenesis in a VEGFC - VEGFR3 dependent manner during experimental autoimmune encephalomyelitis (EAE) and drain both CSF and cells that were once in the CNS parenchyma. Lymphangiogenesis also contributes to the drainage of CNS derived antigens that leads to antigen specific T cell proliferation in the draining lymph nodes during EAE. In contrast, meningeal lymphatics do not undergo lymphangiogenesis during EAE, suggesting heterogeneity in CNS lymphatics. We conclude that increased lymphangiogenesis near the cribriform plate can contribute to the management of neuroinflammation-induced fluid accumulation and immune surveillance.
Ishikawa, K., et al. (2019). “Changes in high endothelial venules in lymph nodes after vascularized and nonvascularized lymph node transfer in a murine autograft model.” J Surg Oncol. [EPub Jan 12]
BACKGROUND AND OBJECTIVES: Vascularized lymph node transfer (LNT) is gaining popularity in the treatment of lymphedema. However, it is unclear whether the vascularization of transferred lymph nodes (LNs) contributes to functional improvement. High endothelial venules (HEVs) are specialized vessels that allow lymphocytes to enter LNs. In this study, we compared the numbers of HEVs and lymphocytes in LNs after vascularized and nonvascularized LNT. METHODS: Fifty mice were divided into three groups (group 1, pedicled vascularized LNT; group 2, pedicled nonvascularized LNT; group 3, free nonvascularized LNT). Afferent lymphatic reconnection was confirmed by patent blue staining. The transferred LNs were harvested 4 weeks after surgery. HEVs, B-cells, and T-cells were subjected to immunohistochemical staining and quantified. RESULTS: Afferent lymphatic reconnection was observed in 13 of 20 transferred LNs in group 1, 11 of 15 in group 2, and 7 of 15 in group 3. The ratio of dilated/total HEVs in transferred LNs with afferent lymphatic reconnection was significantly higher in group 1 than in groups 2 and 3. No significant differences in numbers of B-cells and T-cells were found in the transferred LNs. CONCLUSIONS: We found that more functional HEVs were preserved in cases with successful afferent lymphatic reconnection after vascularized LNT than after nonvascularized LNT.
Janardhan, H. P. and C. M. Trivedi (2019). “Establishment and maintenance of blood-lymph separation.” Cell Mol Life Sci. [EPub Feb 13]
Hippocratic Corpus, a collection of Greek medical literature, described the functional anatomy of the lymphatic system in the fifth century B.C. Subsequent studies in cadavers and surgical patients firmly established that lymphatic vessels drain extravasated interstitial fluid, also known as lymph, into the venous system at the bilateral lymphovenous junctions. Recent advances revealed that lymphovenous valves and platelet-mediated hemostasis at the lymphovenous junctions maintain life-long separation of the blood and lymphatic vascular systems. Here, we review murine models that exhibit failure of blood-lymph separation to highlight the novel mechanisms and molecular targets for the modulation of lymphatic disorders. Specifically, we focus on the transcription factors, cofactors, and signaling pathways that regulate lymphovenous valve development and platelet-mediated lymphovenous hemostasis, which cooperate to maintain blood-lymph separation.
Karakashian, K., et al. (2019). “Computational investigation of the Laplace law in compression therapy.” J Biomech 85: 6–17.
This study aims to use computational methods for elucidating the effect of limb shape on subgarment and subcutaneous pressures, stresses and strains. A framework was built that generates computational models from 3D arm scans using a depth sensing camera. Finite Element Analysis (FEA) was performed on the scans taken from 23 lymphoedema patients. Subgarment pressures were calculated based on local curvature for each patient and showed a large variability of pressure across each arm. Across the cohort an average maximum subgarment pressure of 5100Pa was found as opposed to an intended garment pressure of 2500Pa. Subcutaneous results show that stresses/strains in the adipose tissues more closely follow the subgarment pressures than in the stiffer skin tissues. Another novel finding was that a negative axial gradient in subgarment pressure (from wrist to elbow) consistently led to positive axial gradients for the Von Mises stresses in the adipose tissues; a phenomenon caused by a combination of arm shape and the stiffness ratio between skin and adipose tissues. In conclusion, this work fills a knowledge gap in compression therapy in clinical practice and can inform garment design or lead to optimal treatment strategies.
Kiesewetter, A., et al. (2019). “Phase-specific functions of macrophages determine injury-mediated corneal hem- and lymphangiogenesis.” Sci Rep 9(1): 308.
Macrophages are critical mediators of injury-associated corneal hemangiogenesis (HA) and lymphangiogenesis (LA). Yet, molecular regulators of the hem- and lymphangiogenic potential of corneal wound macrophages are poorly understood. Using two different mouse models of acute (perforating corneal incision injury) and chronic (corneal suture placement model) corneal injury, here we identified distinct functions of early- versus late-phase corneal wound macrophages in corneal HA and LA. Whereas early-phase wound macrophages are essential for initiation and progression of injury-mediated corneal HA and LA, late-phase wound macrophages control maintenance of established corneal lymphatic vessels, but not blood vessels. Furthermore, our findings reveal that the hem- and lymphangiogenic potential of corneal wound macrophages is controlled by the type of the corneal damage. Whereas perforating corneal incision injury induced primarily wound macrophages with lymphangiogenic potential, corneal suture placement provoked wound macrophages with both hem- and lymphangiogenic potential. Our findings highlight a previously unrecognized injury-context dependent role of early- versus late-phase corneal wound macrophages with potential clinical impact on therapy development for sight-threatening corneal neovascular diseases.
Kim, Y., et al. (2019). “Attenuated Lymphatic Proliferation Ameliorates Diabetic Nephropathy and High-Fat Diet-Induced Renal Lipotoxicity.” Sci Rep 9(1): 1994.
Lymphangiogenesis occurs in response to renal injury and is correlated with interstitial fibrosis. Diabetes- and high-fat diet (HFD)-induced intrarenal lipotoxicity and their relationships with lymphangiogenesis are not established. We used PPARalpha agonist, fenofibrate, to unravel the linkage between lipotoxicity and lymphangiogenesis. Eight-week-old male C57BLKS/J db/db mice and HFD Spontaneously hypertensive rats (SHRs) were fed fenofibrate for 12 weeks. HK-2 and RAW264.7 cells were used to investigate their lymphangiogenic capacity in relation to lipotoxicity. Fenofibrate improved intrarenal lipotoxicity by increasing expression of PPARalpha and phosphorylation of AMPK. Lymphatic proliferation was attenuated; expression of lymphatic endothelial hyaluronan receptor-1 (LYVE-1), podoplanin, vascular endothelial growth factor-C (VEGF-C), and vascular endothelial growth factor receptor-3 (VEGFR-3) was decreased. In parallel, extent of tubulointerstitial fibrosis, apoptosis and inflammatory cell infiltration was reduced. In HK2 cells, palmitate- and high glucose-induced over expression of lymphatic makers was diminished by fenofibrate via activation of PPARalpha-AMPK-pACC signaling. Enhanced expression of M1 phenotype in RAW264.7 cells correlated with increased lymphatic growth. A causal relationship between lipotoxicity and lymphatic proliferation with a cellular link to macrophage activation can be speculated; pro-inflammatory M1 type macrophage is involved in the development of lymphangiogenesis through stimulation of VEGF-C and by its transdifferentiation into lymphatic endothelial cells.
Ly, C. L., et al. (2019). “Small Numbers of CD4+ T Cells Can Induce Development of Lymphedema.” Plast Reconstr Surg 143(3): 518e–526e.
BACKGROUND: CD4 T cells have been implicated in the pathology of lymphedema. Interestingly, however, there have been case reports of lymphedema development in patients with low levels of CD4 T cells because of immunosuppression. In this study, the authors sought to delineate the effect of relative CD4 T-cell deficiency on the development of lymphedema in a mouse model. METHODS: A mouse model of relative CD4 T-cell deficiency was created through lethal total body irradiation of wild-type mice that then underwent bone marrow transplantation with progenitors harvested from CD4 knockout mice (wild-type/CD4 knockout). Irradiated CD4 knockout mice reconstituted with wild-type mouse-derived progenitors (CD4 knockout/wild-type), and unirradiated CD4 knockout and wild-type mice were used as controls. All mice underwent tail skin and lymphatic excision to induce lymphedema, and analysis was performed 6 weeks later. RESULTS: Wild-type/CD4 knockout chimeras were not protected from developing lymphedema. Despite a global deficit in CD4 T cells, these mice had swelling, fibrosis, inflammation, and impaired lymphatic transport function indistinguishable from that in wild-type and CD4 knockout/wild-type mice. In contrast, unirradiated CD4 knockout mice had no features of lymphedema after lymphatic injury. CONCLUSIONS: Relatively small numbers of bone marrow and peripheral CD4 T cells are sufficient to induce the development of lymphedema. These findings suggest that lymphatic injury results in expansion of CD4 T-cell populations in lymphedematous tissues.
Ma, C. X., et al. (2019). “Deep lymphatic anatomy of the upper limb: An anatomical study and clinical implications.” Ann Anat 223: 32–42.
BACKGROUND: The deep and perforating lymphatic anatomy of the upper limb still remains the least described in medical literature. MATERIALS AND METHODS: Six upper limbs with the axillary tissue were harvested from three unembalmed human cadavers amputated at the shoulder joint. A small amount of 6% hydrogen peroxide was employed to detect the lymphatic vessels around the deep palmar arch, radial and ulnar neurovascular bundles. A 30-gauge needle was inserted into the vessels and they were injected with a barium sulphate compound. Each specimen was dissected, photographed and radiographed to demonstrate deep lymphatic distribution of the upper limb. RESULTS: Continuing from the deep lymph vessels of the hand, single or multiple deep collecting lymph vessels have been found along the radial, ulnar, anterior and posterior interosseous neurovascular bundles in the forearm, brachial and deep branchial neurovascular bundles in the upper arm. During their courses, lymph nodes were found setting in the trunk of the radial, ulnar and brachial lymph vessels near or in the cubital fossa, and in the axillar. Perforating lymph vessels have been found near the wrist and in the cubital fossa, which linked the superficial and deep lymph vessels. The direction of lymphatic drainage was from the deep to superficial or superficial to deep vessels. CONCLUSION: The deep lymphatic anatomy of the upper limb has been described. The results will provide an anatomical basis for clinical management, educational reference and scientific research.
Narimatsu, A., et al. (2019). “Corneal lymphangiogenesis ameliorates corneal inflammation and edema in late stage of bacterial keratitis.” Sci Rep 9(1): 2984.
Lymphatic vessels play a crucial role in systemic immune response and regulation of tissue fluid homeostasis. Corneal lymphangiogenesis in bacterial keratitis has not been studied. In this study, we investigated the mechanism and the role of corneal lymphangiogenesis in a murine bacterial keratitis model using Pseudomonas aeruginosa. We first demonstrated that corneal lymphangiogenesis was enhanced mainly in the late stage of bacterial keratitis, contrary to corneal angiogenesis that started earlier. Corresponding to the delayed lymphangiogenesis, expression of the pro-lymphangiogenic factors VEGF-C and VEGFR-3 increased in the late stage of bacterial keratitis. We further found that F4/80 and CD11b positive macrophages played an essential role in corneal lymphangiogenesis. Notably, macrophages were specifically involved in corneal lymphangiogenesis in the late stage of bacterial keratitis. Finally, we demonstrated the beneficial role of corneal lymphangiogenesis in ameliorating the clinical course of bacterial keratitis. Our study showed that bacterial activity was not directly involved in the late stage of keratitis, while corneal lymphangiogenesis reduced corneal edema and clinical manifestation in the late stage of bacterial keratitis. These findings suggest that the process of lymphangiogenesis in bacterial keratitis ameliorates corneal inflammation and edema in the late stage of bacterial keratitis.
Olszewski, W. L., et al. (2019). “Edema Fluid Can Be Successfully Evacuated from the Lymphedematous Limbs by Implantation of Silicone Tubings Bypassing the Site of Flow Obstruction Long-Term Observations.” Lymphat Res Biol.
BACKGROUND: Lymphedema of limbs is caused by partial or total obstruction of lymphatic collectors. In advanced cases all main lymphatics are obstructed and tissue fluid accumulates in the interstitial spaces. The microsurgical lympho-venous shunts cannot be performed. We propose in such cases drainage of fluid accumulations by creating artificial flow pathways to the nonobstructed regions by implantation of silicone tubes. AIM: To present the 3 to over 6 year follow-up results of therapy by subcutaneous implantation of silicone tubes. METHODS: In 150 patients with obstructive limb lymphedema after pelvic or axillary lymphadenectomy and irradiation in uterine or breast cancer or following soft tissue inflammation silicone tubes were implanted subcutaneously. RESULTS: There was (1) immediate decrease of limb circumference within days after implantation; (2) in lower limbs in a 3-year follow-up a decrease in mid-calf circumference by a mean − 8.7% (p < 0.05) with range of −3.2% to −31.0% corresponding to 90–900 mL volume and in the mid-thigh a mean − 1.8% (p < 0.05) with range of −9.3% to +3% equal to 0–900 mL. In the upper limb in the 2-year follow-up the decrease in the mid-forearm was −8.5% (p < 0.01) with a range of −3.0% to −22.0% and in the mid-arm a mean − 12% (p < 0.05) with a range of −7% to −22%. That corresponded to 180–700 mL volume for the limb; (3) decreased tissue stiffness; (4) maintenance of tubes patency on control lymphoscintigraphy, contrast opacification, and ultrasonography; and (5) lack of reaction to foreign body and effective control of inflammation at the site of implantation using low doses of benzathine penicillin. CONCLUSIONS: The technical simplicity of the surgical procedure, fast decrease of limb edema, and lack of tissue reaction to the implant make the method worth applying in advanced stages of lymphedema.
Omura, S., et al. (2018). “Theiler's Virus-Mediated Immunopathology in the CNS and Heart: Roles of Organ-Specific Cytokine and Lymphatic Responses.” Front Immunol 9: 2870.
Theiler's murine encephalomyelitis virus (TMEV) induces different diseases in the central nervous system (CNS) and heart, depending on the mouse strains and time course, with cytokines playing key roles for viral clearance and immune-mediated pathology (immunopathology). In SJL/J mice, TMEV infection causes chronic TMEV-induced demyelinating disease (TMEV-IDD) in the spinal cord about 1 month post-inoculation (p.i.). Unlike other immunopathology models, both pro- and anti-inflammatory cytokines can play dual roles in TMEV-IDD. Pro-inflammatory cytokines play beneficial roles in viral clearance while they are also detrimental in immune-mediated demyelination. Anti-inflammatory cytokines suppress not only protective anti-viral immune responses but also detrimental autoreactive immune responses. Conversely, in C3H mice, TMEV infection induces a non-CNS disease, myocarditis, with three distinctive phases: phase I, viral pathology with interferon and chemokine responses; phase II, immunopathology mediated by acquired immune responses; and phase III, cardiac fibrosis. Although the exact mechanism(s) by which a single virus, TMEV, induces these different diseases in different organs is unclear, our bioinformatics approaches, especially principal component analysis (PCA) of transcriptome data, allow us to identify the key factors contributing to organ-specific immunopathology. The PCA demonstrated that in vitro infection of a cardiomyocyte cell line reproduced the transcriptome profile of phase I in TMEV-induced myocarditis; distinct interferon/chemokine-related responses were induced in vitro in TMEV-infected cardiomyocytes, but not in infected neuronal cells. In addition, the PCA of the in vivo CNS transcriptome data showed that decreased lymphatic marker expressions were weakly associated with inflammation in TMEV infection. Here, dysfunction of lymphatic vessels is shown to potentially contribute to immunopathology by delaying the clearance of cytokines and immune cells from the inflammatory site, although this can also confine the virus at these sites, preventing virus spread via lymphatic vessels. On the other hand, in the heart, dysfunction of lymphatics was associated with reduced lymphatic muscle contractility provoked by pro-inflammatory cytokines. Therefore, TMEV infection may induce different patterns of cytokine expressions as well as lymphatic vessel dysfunction by rather different mechanisms between the CNS and heart, which might explain observed patterns of organ-specific immunopathology.
Paniagua, D., et al. (2019). “Antivenom effect on lymphatic absorption and pharmacokinetics of coral snake venom using a large animal model.” Clin Toxicol (Phila): 1–8.
CONTEXT: Historically, administration and dosing of antivenom (AV) have been guided primarily by physician judgment because of incomplete understanding of the envenomation process. As demonstrated previously, lymphatic absorption plays a major role in the availability and pharmacokinetics (PK) of coral snake venom injected subcutaneously, which suggests that absorption from subcutaneous tissue is the limiting step for venom bioavailability, supporting the notion that the bite site is an ongoing venom depot. This feature may underlie the recurrence phenomena reported in viperid envenomation that appear to result from a mismatch between venom and AV PK. The role of lymphatic absorption in neutralization of venom by AV administered intravenously remains unclear. METHODS: The effect of AV on systemic bioavailability and neutralization of Micrurus fulvius venom was assessed using a central lymph-cannulated sheep model. Venom was administered by subcutaneous injection in eight sheep, four with and four without thoracic duct cannulation and drainage. Two hours after venom injection, AV was administered intravenously. Venom and AV concentrations in serum and lymph were determined by ELISA assay from samples collected over a 6-h period and in tissues harvested post-mortem. RESULTS: After AV injection, venom levels in serum fell immediately to undetectable with a subsequent increase in concentration attributable to non-toxic venom proteins. In lymph, AV became detectable 6 min after treatment; venom levels dropped concurrently but remained detectable 4 h later. Post-mortem samples from the venom injection site confirmed the presence of venom near the point of injection. Neither venom nor AV was detected at significant concentrations in major organs or contralateral skin. CONCLUSIONS: Intravenous AV immediately neutralizes venom in the bloodstream and can extravasate to neutralize venom absorbed by lymph but this neutralization seems to be slow and incomplete. Residual venom in the inoculation site demonstrates that this site functions as a depot where it is not neutralized by AV, which allows the venom to remain active with slow delivery to the bloodstream for ongoing systemic distribution.
Patel, T. K., et al. (2019). “Dural lymphatics regulate clearance of extracellular tau from the CNS.” Mol Neurodegener 14(1): 11.
BACKGROUND: Alzheimer's disease is characterized by two main neuropathological hallmarks: extracellular plaques of amyloid-beta (Abeta) protein and intracellular aggregates of tau protein. Although tau is normally a soluble monomer that bind microtubules, in disease it forms insoluble, hyperphosphorylated aggregates in the cell body. Aside from its role in AD, tau is also involved in several other neurodegenerative disorders collectively called tauopathies, such as progressive supranuclear palsy (PSP), corticobasal degeneration (CBD), some forms of frontotemporal dementia, and argyrophilic grain disease (AGD). The prion hypothesis suggests that after an initial trigger event, misfolded forms of tau are released into the extracellular space, where they spread through different brain regions, enter cells, and seeding previously normal forms. Thus understanding mechanisms regulating the clearance of extracellular tau from the CNS is important. The discovery of a true lymphatic system in the dura and its potential role in mediating Abeta pathology prompted us to investigate its role in regulating extracellular tau clearance. METHODS: To study clearance of extracellular tau from the brain, we conjugated monomeric human tau with a near-infrared dye cypate, and injected this labeled tau in the parenchyma of both wild-type and K14-VEGFR3-Ig transgenic mice, which lack a functional CNS lymphatic system. Following injection we performed longitudinal imaging using fluorescence molecular tomography (FMT) and quantified fluorescence to calculate clearance of tau from the brain. To complement this, we also measured tau clearance to the periphery by measuring plasma tau in both groups of mice. RESULTS: Our results show that a significantly higher amount of tau is retained in the brains of K14-VEGFR3-Ig vs. wild type mice at 48 and 72 h post-injection and its subsequent clearance to the periphery is delayed. We found that clearance of reference tracer human serum albumin (HSA) was also significantly delayed in the K14-VEGFR3-Ig mice. CONCLUSIONS: The dural lymphatic system appears to play an important role in clearance of extracellular tau, since tau clearance is impaired in the absence of functional lymphatics. Based on our baseline characterization of extracellular tau clearance, future studies are warranted to look at the interaction between tau pathology and efficiency of lymphatic function.
Perrault, D. P., et al. (2019). “Small Peptide Modulation of Fibroblast Growth Factor Receptor 3-Dependent Postnatal Lymphangiogenesis.” Lymphat Res Biol 17(1): 19–29.
BACKGROUND: The fibroblast growth factor receptor (FGFR) family includes transmembrane receptors involved in a wide range of developmental and postdevelopmental biologic processes as well as a wide range of human diseases. In particular, FGFR3 has been implicated in the mechanism by which 9-cis retinoic acid (9-cisRA) induces lymphangiogenesis and improves lymphedema. The purpose of this study was to validate the efficacy of a novel small peptide FGFR3 inhibitor, peptide P3 (VSPPLTLGQLLS), and to elucidate the role of FGFR3 in 9-cisRA-induced lymphangiogenesis using this peptide. METHODS AND RESULTS: Peptide P3 effectively inhibited FGFR3 phosphorylation. In vitro, peptide P3-mediated FGFR3 inhibition did not decrease lymphatic endothelial cell (LEC) proliferation, migration, or tubule formation. However, peptide P3-mediated FGFR3 inhibition did block 9-cisRA-stimulated LEC proliferation, migration, and tubule formation. In vivo, peptide P3-mediated FGFR3 inhibition was sufficient to inhibit 9-cisRA-induced tracheal lymphangiogenesis. CONCLUSION: FGFR3 does not appear to be essential to nonpromoted LEC proliferation, migration, and tubule formation. However, FGFR3 may play a key role in LEC proliferation, migration, tubule formation, and postnatal in vivo lymphangiogenesis when pharmacologically induced by 9-cisRA. P3 may have the potential to be used as a precise regulatory control element for 9-cisRA-mediated lymphangiogenesis.
Petrova, T. V. and G. Y. Koh (2018). “Organ-specific lymphatic vasculature: From development to pathophysiology.” J Exp Med 215(1): 35–49.
Recent discoveries of novel functions and diverse origins of lymphatic vessels have drastically changed our view of lymphatic vasculature. Traditionally regarded as passive conduits for fluid and immune cells, lymphatic vessels now emerge as active, tissue-specific players in major physiological and pathophysiological processes. Lymphatic vessels show remarkable plasticity and heterogeneity, reflecting their functional specialization to control the tissue microenvironment. Moreover, alternative developmental origins of lymphatic endothelial cells in some organs may contribute to the diversity of their functions in adult tissues. This review aims to summarize the most recent findings of organotypic differentiation of lymphatic endothelial cells in terms of their distinct (patho)physiological functions in skin, lymph nodes, small intestine, brain, and eye. We discuss recent advances in our understanding of the heterogeneity of lymphatic vessels with respect to the organ-specific functional and molecular specialization of lymphatic endothelium, such as the hybrid blood-lymphatic identity of Schlemm's canal, functions of intestinal lymphatics in dietary fat uptake, and discovery of meningeal lymphatic vasculature and perivascular brain lymphatic endothelial cells.
Polomska, A. K., et al. (2019). “Minimally invasive method for the point-of-care quantification of lymphatic vessel function.” JCI Insight 4(4).
Current clinical methods for the evaluation of lymphatic vessel function, crucial for early diagnosis and evaluation of treatment response of several pathological conditions, in particular of postsurgical lymphedema, are based on complex and mainly qualitative imaging techniques. To address this unmet medical need, we established a simple strategy for the painless and quantitative assessment of cutaneous lymphatic function. We prepared a lymphatic-specific tracer formulation, consisting of the clinically approved near-infrared fluorescent dye, indocyanine green, and the solubilizing surfactant Kolliphor HS15. The tracer was noninvasively delivered to the dermal layer of the skin using MicronJet600 hollow microneedles, and the fluorescence signal decay at the injection site was measured over time using a custom-made, portable detection device. The decay rate of fluorescence signal in the skin was used as a direct measure of lymphatic vessel drainage function. With this method, we could quantify impaired lymphatic clearance in transgenic mice lacking dermal lymphatics and distinguish distinct lymphatic clearance patterns in pigs in different body locations and under manual stimulus. Overall, this method has the potential for becoming a noninvasive and quantitative clinical “office test” for lymphatic function assessment.
Rockson, S. G. (2019). “Modulation of Fibroblast Growth Factor Expression in Lymphedema.” Lymphat Res Biol 17(1): 1.
Rockson, S. G., et al. (2018). “Pilot studies demonstrate the potential benefits of antiinflammatory therapy in human lymphedema.” JCI Insight 3(20).
BACKGROUND: Lymphedema is a common condition affecting millions around the world that still lacks approved medical therapy. Because ketoprofen, an NSAID, has been therapeutic in experimental lymphedema, we evaluated its efficacy in humans. METHODS: We first performed an exploratory open-label trial. Patients with either primary or secondary lymphedema received ketoprofen 75 mg by mouth 3 times daily for 4 months. Subjects were evaluated for changes in histopathology, with skin thickness, limb volume, and tissue bioimpedance changes serving as secondary endpoints. Based on our encouraging findings, we next conducted a placebo-controlled trial, with the primary outcome defined as a change in skin thickness, as measured by skin calipers. Secondary endpoints for this second study included histopathology, limb volume, bioimpedance, and systemic inflammatory mediators. RESULTS: We enrolled 21 lymphedema patients in the open-label trial, from November 2010 to July 2011. Histopathology and skin thickness were significantly improved at 4 months compared with baseline. In the follow-up, double-blind, placebo-controlled trial, we enrolled 34 patients from August 2011 to October 2015, with 16 ketoprofen recipients and 18 placebo-treated subjects. No serious adverse events occurred. The ketoprofen recipients demonstrated reduced skin thickness, as well as improved composite measures of histopathology and decreased plasma granulocyte CSF (G-CSF) expression. CONCLUSION: These 2 exploratory studies together support the utility of targeted antiinflammatory therapy with ketoprofen in patients with lymphedema. Our results highlight the promise of such approaches to help restore a failing lymphatic circulation. TRIAL REGISTRATION: ClinicalTrials.gov NCT02257970.
Sato, T., et al. (2019). “Involvement of premacular mast cells in the pathogenesis of macular diseases.” PLoS One 14(2): e0211438.
We previously reported on the elevated intravitreal activities of tryptase and chymase in association with idiopathic epiretinal membrane (ERM) and idiopathic macular hole (MH). In this present study, we investigated the potential intraocular production of these serine proteases, and measured and compared tryptase and chymase activities in the vitreous body and serum in ERM, MH, proliferative diabetic retinopathy (PDR), and rhegmatogenous retinal detachment (RRD) patients. In addition, nuclear staining with hematoxylin and eosin (H&E) and mast-cell staining with toluidine blue were performed on samples of the vitreous core and bursa premacularis (BPM) of MH. We also performed immunostaining on the above two regions of vitreous samples for MH with anti-tryptase antibody, anti-chymase antibody, anti-podoplanin antibody, anti-lymphatic vessel endothelial hyaluronan receptor 1 (LYVE-1) antibody, and anti-fibroblast antibody. Moreover, we performed immunostaining with anti-tryptase antibody and anti-chymase antibody on ERMs collected intraoperatively. Tryptase activity in the vitreous body was significantly higher in ERM and MH than in PDR. However, no significant differences were observed in the tryptase activity in the serum among these four diseases. Chymase activity in the vitreous body was significantly higher in MH than in the other three diseases, yet chymase activity in the serum was below detection limit in any of the diseases. Nuclear staining with H&E revealed an abundance of nuclei in the BPM region, but few in the surrounding area. Mast-cell staining with toluidine blue revealed that the BPM showed metachromatic staining. In immunostaining with anti-fibroblasts antibody, anti-tryptase antibody, anti-chymase antibody, anti-podoplanin antibody, and anti-LYVE-1 antibody, the BPM stained more strongly than the vitreous core. Tryptase and chymase-positive cells were also observed in ERM. These findings revealed that the presence of mast cells in the BPM potentially represent the source of these serine proteases. Moreover, the BPM, as a lymphatic tissue, may play an important role in the pathogenesis of macular disease.
Subileau, M., et al. (2019). “Bone Morphogenetic Protein 9 Regulates Early Lymphatic-Specified Endothelial Cell Expansion during Mouse Embryonic Stem Cell Differentiation.” Stem Cell Reports 12(1): 98–111.
Exogenous cues involved in the regulation of the initial steps of lymphatic endothelial development remain largely unknown. We have used an in vitro model based on the co-culture of vascular precursors derived from mouse embryonic stem cell (ESC) differentiation and OP9 stromal cells to examine the first steps of lymphatic specification and expansion. We found that bone morphogenetic protein 9 (BMP9) induced a dose-dependent biphasic effect on ESC-derived vascular precursors. At low concentrations, below 1 ng/mL, BMP9 expands the LYVE-1-positive lymphatic progeny and activates the calcineurin phosphatase/NFATc1 signaling pathway. In contrast, higher BMP9 concentrations preferentially enhance the formation of LYVE-1-negative endothelial cells. This effect results from an OP9 stromal cell-mediated VEGF-A secretion. RNA-silencing experiments indicate specific involvement of ALK1 and ALK2 receptors in these different BMP9 responses. BMP9 at low concentrations may be a useful tool to generate lymphatic endothelial cells from stem cells for cell-replacement strategies.
Sun, Y., et al. (2019). “IL-7 enhances the differentiation of adipose-derived stem cells toward lymphatic endothelial cells through AKT signaling.” Cell Biol Int. [EPub Jan 28]
Our study was designed to investigate the effects of IL-7 during the differentiation process of adipose-derived stem cells (ADSCs) toward lymphatic endothelial cells (LECs). IL-7 was added to the traditional induced medium, which was called the IL-7 (+) group, while the group that used traditional induced medium was called the IL-7 (-) group. After 7 days of induction of ADSCs, a comprehensive analysis was conducted between these two groups. We examined the changes in Prox1, LYVE-1, Podoplanin and VEGFR-3 on the RNA and protein level and found that the expression of LEC markers in the IL-7 (+) group was higher than in the IL-7 (-) group. The characteristics of differentiated cells were confirmed by flow cytometry and immunofluorescence. At the same time, we detected the MAPK/ERK and PI3K/AKT pathway involved in the differentiation process, and we found that the phosphorylation of AKT increased, however the expression of ERK was not significantly changed. In conclusion, our study found that IL-7 could improve the differentiation efficiency of ADSCs toward LECs through AKT signaling pathways.
Surya, V. N., et al. (2019). “Lymphatic endothelial cell calcium pulses are sensitive to spatial gradients in wall shear stress.” Mol Biol Cell: mbcE18100618.
Cytosolic calcium (Ca(2+)) is a ubiquitous second messenger that influences numerous aspects of cellular function. In many cell types cytosolic Ca(2+) concentrations are characterized by periodic pulses whose dynamics can influence downstream signal transduction. Here, we examined the general question of how cells use Ca(2+) pulses to encode input stimuli in the context of the response of lymphatic endothelial cells (LECs) to fluid flow. Previous work shows that fluid flow regulates Ca(2+) dynamics in LECs, and that Ca(2+)-dependent signaling plays a key role in regulating lymphatic valve formation during embryonic development. However, how fluid flow might influence the Ca(2+) pulse dynamics of individual LECs remained, to our knowledge, little explored. We used live-cell imaging to characterize Ca(2+) pulse dynamics in LECs exposed to fluid flow in an in vitro flow device that generates spatial gradients in wall shear stress (WSS) such as are found at sites of valve formation. We found that the frequency of Ca(2+) pulses was sensitive to the magnitude of WSS, while the duration of individual Ca(2+) pulses increased in the presence of spatial gradients in WSS. These observations reveal an example of how cells can separately modulate Ca(2+) pulse frequency and duration to encode distinct forms of information, a phenomenon that could extend to other cell types. Movie S1 Movie S1 HLMVEC Ca(2+) dynamics in the IFC, recorded for 30 minutes starting from the onset of flow at t = 50 s. Regions corresponding to Rings 1 and 2 are shown, which have average WSSs of 32 and 65 dyn/cm(2), respectively. The flow direction is radially outward and symmetric about the jet center at the center of Ring 1. Frames were recorded every 5 seconds. Scale bar, 100 mum. Movie S2 Movie S2 HLMVEC Ca(2+) dynamics as in Movie 1 for Rings 2 -6, which have average WSSs of 65, 53, 30, 17 and 11 dyn/cm(2). The flow direction is radially outward and here is roughly from left to right. Frames were recorded every 5 seconds. Scale bar, 100 mum. Movie S3 Movie S3 HLMVEC Ca(2+) dynamics for cells exposed to uniform WSS (parallel plate flow), recorded for 30 minutes from the onset of flow at t = 50 s. Here, all HLMVECs experience a WSS of 50 dyn/cm(2). The flow direction is from the bottom of the video to the top. Frames were recorded every 5 seconds. Scale bar, 100 mum. Movie S4 Movie S4 HLMVEC Ca(2+) dynamics under no flow conditions, recorded for 30 minutes. Frames were recorded every 5 seconds. Scale bar, 100 mum.
Suzuki, Y., et al. (2019). “Comparison of patency rates of lymphaticovenous anastomoses at different sites for lower extremity lymphedema.” J Vasc Surg Venous Lymphat Disord 7(2): 222–227.
OBJECTIVE: Lymphaticovenous anastomosis (LVA) is one of the surgical treatments of lymphedema. However, only a few reports have evaluated LVA directly. This study aimed to evaluate the patency of LVA using indocyanine green fluorescence lymphography and to determine the optimal anastomosis site in patients with lower extremity lymphedema. METHODS: Thirty-six patients, with a total of 123 anastomoses for lower extremity lymphedema including 3 cases of idiopathic lymphedema, who underwent LVA for the first time between March 2014 and March 2017 were selected for enrollment in this study. The patency of the anastomoses was evaluated using PDE-neo (Hamamatsu Photonics, Hamakita, Japan) by injecting indocyanine green into the subcutaneous tissue at 6 months postoperatively. The site of anastomosis was the intersection point of the lymphatic vessel and vein, which was identified preoperatively. To determine the best surgical location, the anastomosis site was classified into the joint area (ankle and knee) and nonjoint area (dorsum and lower leg). The anastomosis was evaluated as either patent or nonpatent. RESULTS: Patency was confirmed in 37 of the 76 (49%) anastomoses at the joint area and 12 of the 47 (26%) at nonjoint areas (P = .01). CONCLUSIONS: The patency rate was significantly higher around the joint area than at the nonjoint areas. LVA around the joint area is recommended to ensure favorable technical and surgical outcomes for patients with lower extremity lymphedema.
Trincot, C. E., et al. (2019). “Adrenomedullin Induces Cardiac Lymphangiogenesis After Myocardial Infarction and Regulates Cardiac Edema Via Connexin 43.” Circ Res 124(1): 101–113.
RATIONALE: Cardiac lymphangiogenesis contributes to the reparative process post-myocardial infarction, but the factors and mechanisms regulating it are not well understood. OBJECTIVE: To determine if epicardial-secreted factor AM (adrenomedullin; Adm = gene) improves cardiac lymphangiogenesis post-myocardial infarction via lateralization of Cx43 (connexin 43) in cardiac lymphatic vasculature. METHODS AND RESULTS: Firstly, we identified sex-dependent differences in cardiac lymphatic numbers in uninjured mice using light-sheet microscopy. Using a mouse model of Adm (hi/hi) (Adm overexpression) and permanent left anterior descending ligation to induce myocardial infarction, we investigated cardiac lymphatic structure, growth, and function in injured murine hearts. Overexpression of Adm increased lymphangiogenesis and cardiac function post-myocardial infarction while suppressing cardiac edema and correlated with changes in Cx43 localization. Lymphatic function in response to AM treatment was attenuated in mice with a lymphatic-specific Cx43 deletion. In vitro experiments in cultured human lymphatic endothelial cells identified a novel mechanism to improve gap junction coupling by pharmaceutically targeting Cx43 with verapamil. Finally, we show that connexin protein expression in cardiac lymphatics is conserved between mouse and human. CONCLUSIONS: AM is an endogenous, epicardial-derived factor that drives reparative cardiac lymphangiogenesis and function via Cx43, and this represents a new therapeutic pathway for improving myocardial edema after injury.
van Beek, J. G. M., et al. (2019). “Absence of Intraocular Lymphatic Vessels in Uveal Melanomas with Extrascleral Growth.” Cancers (Basel) 11(2).
The aim of this study was to investigate the presence of intraocular lymphatic vessels in patients with uveal melanomas and extrascleral extension using a panel of lymphatic markers. The following immunohistochemical markers were analyzed: lymphatic vessel endothelial hyaluronic acid receptor-1 (LYVE-1), podoplanin (D2-40), prospero-related homeobox gene-1 (Prox-1), pan-endothelial marker cluster of differentiation 31 (CD31), and blood vessel endothelium-specific CD34. Lymphatic vessels were defined as a combination of staining of the following positive markers: LYVE-1, D2-40, Prox-1, and CD31; and no staining of the negative marker CD34. In total, 456 patients were enucleated; 16 of the 46 uveal melanomas with extrascleral extension were contained in stored paraffin tissue. Two samples of the 16 uveal melanomas showed focal positive intraocular vascular staining for LYVE-1 and co-expression of CD31 and CD34. Due to the lack of Prox-1 and D2-40, and positive expression of CD34, these cannot be classified as lymphatic vessels. In one case recruitment of an extraocular, intratumoral lymphatic vascular structure was observed in the periphery of the subconjunctival extrascleral extension. Intraocular lymphatic vessels are absent in uveal melanomas with extrascleral extension; however, we provide proof for recruitment of intratumoral lymphatics by uveal melanomas with extraocular extension from subconjunctival lymphatics that may explain the rare cases of regional lymphatic spread. A panel of antibodies is necessary to detect lymphatic vessels with high specificity.
Van de Velde, M., et al. (2018). “Ear Sponge Assay: A Method to Investigate Angiogenesis and Lymphangiogenesis in Mice.” Methods Mol Biol 1731: 223–233.
Angiogenesis and lymphangiogenesis have become important research areas in the biomedical field. The outgrowth of new blood (angiogenesis) and lymphatic (lymphangiogenesis) vessels from preexisting ones is involved in many pathologies including cancer. In-depth investigations of molecular determinants such as proteases in these complex processes require reliable in vivo models. Here we present the ear sponge assay as an easy, rapid, quantitative and reproducible model of angiogenesis and lymphangiogenesis. In this system, a gelatin sponge soaked with tumor cells, cell-conditioned medium, or a compound to be tested is implanted, for 2–4 weeks, between the two mouse ear skin layers. The two vascular networks are next examined through histological procedures.
Vishwakarma, N., et al. (2019). “Lipid-Based Nanocarriers for Lymphatic Transportation.” AAPS PharmSciTech 20(2): 83.
The effectiveness of any drug is dependent on to various factors like drug solubility, bioavailability, selection of appropriate delivery system, and proper route of administration. The oral route for the delivery of drugs is undoubtedly the most convenient, safest and has been widely used from past few decades for the effective delivery of drugs. However, despite of the numerous advantages that oral route offers, it often suffers certain limitations like low bioavailability due to poor water solubility as well as poor permeability of drugs, degradation of the drug in the physiological pH of the stomach, hepatic first-pass metabolism, etc. The researchers have been continuously working extensively to surmount and address appropriately the inherent drawbacks of the oral drug delivery. The constant and continuous efforts have led to the development of lipid-based nano drug delivery system to overcome the aforesaid associated challenges of the oral delivery through lymphatic transportation. The use of lymphatic route has demonstrated its critical and crucial role in overcoming the problem associated and related to low bioavailability of poorly water-soluble and poorly permeable drugs by bypassing intestinal absorption and possible first-pass metabolism. The current review summarizes the bonafide perks of using the lipid-based nanocarriers for the delivery of drugs using the lymphatic route. The lipid-based nanocarriers seem to be a promising delivery system which can be optimized and further explored as an alternative to the conventional dosage forms for the enhancement of oral bioavailability of drugs, with better patient compliance, minimum side effect, and improved the overall quality of life.
Voisin, M. B. and S. Nourshargh (2018). “Neutrophil trafficking to lymphoid tissues: physiological and pathological implications.” J Pathol. [EPub Dec 25]
Recent advances have provided evidence for the involvement of neutrophils in both innate and adaptive immunity, robustly challenging the old dogma that neutrophils are short-lived prototypical innate immune cells solely involved in acute responses to microbes and exerting collateral tissue damage. There is now ample evidence showing that neutrophils can migrate into different compartments of the lymphoid system where they contribute to the orchestration of the activation and/or suppression of lymphocyte effector functions in homeostasis and during chronic inflammation, such as autoimmune disorders and cancer. In support of this notion, neutrophils can generate a wide range of cytokines and other mediators capable of regulating the survival, proliferation and functions of both T and B cells. In addition, neutrophils can directly engage with lymphocytes and promote antigen presentation. Furthermore, there is emerging evidence of the existence of distinct and diverse neutrophil phenotypes with immunomodulatory functions that characterise different pathological conditions, including chronic and autoimmune inflammatory conditions. The aim of this review is to discuss the mechanisms implicated in neutrophil trafficking into the lymphoid system and to provide an overview of the immuno-regulatory functions of neutrophils in health and disease in the context of adaptive immunity. Copyright (c) 2018 The Authors. The Journal of Pathology published by John Wiley & Sons Ltd on behalf of Pathological Society of Great Britain and Ireland.
Yanev, P., et al. (2019). “Impaired meningeal lymphatic vessel development worsens stroke outcome.” J Cereb Blood Flow Metab: 271678 × 18822921.
The discovery of meningeal lymphatic vessels (LVs) has sparked interest in identifying their role in diseases of the central nervous system. Similar to peripheral LVs, meningeal LVs depend on vascular endothelial growth factor receptor-3 (VEGFR3) signaling for development. Here we characterize the effect of stroke on meningeal LVs, and the impact of meningeal lymphatic hypoplasia on post-stroke outcomes. We show that photothrombosis (PT), but not transient middle cerebral artery occlusion (tMCAo), induces meningeal lymphangiogenesis in young male C57Bl/J6 mice. We also show that Vegfr3(wt/mut) mice develop significantly fewer meningeal LVs than Vegfr3(wt/wt) mice. Again, meningeal lymphangiogenesis occurs in the alymphatic zone lateral to the sagittal sinus only after PT-induced stroke in Vegfr3(wt/wt) mice. Interestingly, Vegfr3(wt/mut) mice develop larger stroke volumes than Vegfr3(wt/wt) mice after tMCAo, but not after PT. Our results reveal differences between PT and tMCAo models of stroke and underscore the need to consider method of stroke induction when investigating the role of meningeal lymphatics. Taken together, our data indicate that ischemic injury can induce the growth of meningeal LVs and that the absence of these LVs can impact post-stroke outcomes.
Yen, H. H., et al. (2019). “Characterisation of ovine lymphatic vessels in fresh specimens.” PLoS One 14(1): e0209414.
BACKGROUND AND AIM: The development and use of experimental models using lymphatic cannulation techniques have been hampered by the lack of high-quality colour imaging of lymphatic vessels in situ. Most descriptions of lymphatic anatomy in sheep have historically depended on schematic diagrams due to limitations in the ability to publish colour images of the lymphatic vessels with decent resolution. The aim of this work was to encourage more widespread use of the ovine cannulation model by providing clear photographic images identifying the location and anatomical layout of some major lymphatic ducts and their in situ relationship to surrounding tissues. METHODS: The cadavers of the sheep were collected after they had been euthanized at the end of animal trials not associated with this study. The lymphatics were dissected and exposed to show their appearance in the surrounding tissues and their relationship to other organs. Patent Blue was used to locate lymphatic vessels in exploratory preparations. However, in order to present the natural appearance of the vessels, we used minimal dissection and dye was not used for the photographed examples. Instead, we have indicated the course of the vessels with lines where their position is less clear. RESULTS AND CONCLUSION: In this paper, we have used sheep specimens as examples to show characteristic images of lymphatic vessels. The images of in situ lymphatics and lymph nodes combined with schematic summaries provide a concise illustration of the lymphatic drainage scheme in sheep.
Yuan, Y., et al. (2019). “Modulation of Immunity by Lymphatic Dysfunction in Lymphedema.” Front Immunol 10: 76.
The debilitating condition known as secondary lymphedema frequently occurs after lymphadenectomy and/or radiotherapy for the treatment of cancer. These therapies can damage lymphatic vessels leading to edema, fibrosis, inflammation and dysregulated adipogenesis, which result in profound swelling of an affected limb. Importantly, lymphedema patients often exhibit impaired immune function which predisposes them to a variety of infections. It is known that lymphadenectomy can compromise the acquisition of adaptive immune responses and antibody production; however the cellular mechanisms involved are poorly understood. Here we discuss recent progress in revealing the cellular and molecular mechanisms underlying poor immune function in secondary lymphedema, which has indicated a key role for regulatory T cells in immunosuppression in this disease. Furthermore, the interaction of CD4(+) T cells and macrophages has been shown to play a role in driving proliferation of lymphatic endothelial cells and aberrant lymphangiogenesis, which contribute to interstitial fluid accumulation in lymphedema. These new insights into the interplay between lymphatic vessels and the immune system in lymphedema will likely provide opportunities for novel therapeutic approaches designed to improve clinical outcomes in this problematic disease.
Clinical
Choi, S. M., et al. (2019). “Successful treatment of conjunctival lymphangiectasia accompanied by corneal dellen using a high-frequency radiowave electrosurgical device.” Indian J Ophthalmol 67(3): 409–411.
A 62-year-old man presented with a 1-month history of right eye pain unresponsive to artificial tears and topical steroids. At presentation, bullous yellowish fluid collection was noted in the nasal conjunctiva. Corneal thinning and opacity were observed at the 3 o'clock position of the cornea. High-frequency radiowave ablation and biopsy were performed at the affected area. Conjunctival lymphangiectasia was confirmed by excisional biopsy. An improvement in the degree of corneal dellen and chemosis was evident 1 week after ablation. Use of a high-frequency radiowave electrosurgical device may be a simple and effective treatment option for symptomatic conjunctival lymphangiectasia.
Ciudad, P., et al. (2019). “Comprehensive multimodal surgical treatment of end-stage lower extremity lymphedema with toe management: The combined Charles,' Homan's, and vascularized lymph node transfer (CHAHOVA) procedures.” J Surg Oncol 119(4): 430–438.
BACKGROUND: End-stage lower extremity lymphedema (LEL) poses a particularly formidable challenge to surgeons as multiple pathological processes are at work. Because single modality treatment is often unsuccessful, we devised a comprehensive multimodal surgical treatment. The aim of this study is to share the technical considerations and examine the clinical outcomes of this combined approach. METHODS: Between 2013 and 2017, patients with International Society of Lymphology stage III, who underwent the combination treatment of Charles,' Homan's procedure with toe management and vascularized lymph node transfer (CHAHOVA), were included in this retrospective study. Outcomes evaluated were limb size, number of infectious episodes, compression garment usage, and rate of complications. RESULTS: A total of 68 patients were included. With a mean follow-up of 29 months, the overall circumference reduction rate for the upper thigh and the rest of the extremity was 67.4% (48.2–88.2%) and 98.1% (88–100%), respectively. During the follow-ups, 2 (2.9%) patients experienced episodes of cellulitis and the average number of yearly infections decreased from 4.2 to 1.2 episodes per person. All patients were able to discontinue compression therapy without recurrence of lymphedema. Nine (13.2%) patients reported minor complications. CONCLUSION: The combine CHAHOVA in a single-stage procedure is an effective and safe approach in the end-stage LEL.
Craven, M. D. and R. J. Washabau (2019). “Comparative pathophysiology and management of protein-losing enteropathy.” J Vet Intern Med. [EPub Feb 14]
Protein-losing enteropathy, or PLE, is not a disease but a syndrome that develops in numerous disease states of differing etiologies and often involving the lymphatic system, such as lymphangiectasia and lymphangitis in dogs. The pathophysiology of lymphatic disease is incompletely understood, and the disease is challenging to manage. Understanding of PLE mechanisms requires knowledge of lymphatic system structure and function, which are reviewed here. The mechanisms of enteric protein loss in PLE are identical in dogs and people, irrespective of the underlying cause. In people, PLE is usually associated with primary intestinal lymphangiectasia, suspected to arise from genetic susceptibility, or “idiopathic” lymphatic vascular obstruction. In dogs, PLE is most often a feature of inflammatory bowel disease (IBD), and less frequently intestinal lymphangiectasia, although it is not proven which process is the true driving defect. In cats, PLE is relatively rare. Review of the veterinary literature (1977–2018) reveals that PLE was life-ending in 54.2% of dogs compared to published disease-associated deaths in IBD of <20%, implying that PLE is not merely a continuum of IBD spectrum pathophysiology. In people, diet is the cornerstone of management, whereas dogs are often treated with immunosuppression for causes of PLE including lymphangiectasia, lymphangitis, and crypt disease. Currently, however, there is no scientific, extrapolated, or evidence-based support for an autoimmune or immune-mediated mechanism. Moreover, people with PLE have disease-associated loss of immune function, including lymphopenia, severe CD4+ T-cell depletion, and negative vaccinal titers. Comparison of PLE in people and dogs is undertaken here, and theories in treatment of PLE are presented.
Drivdal, M., et al. (2018). “A nine year follow-up study of patients with lymphoedema cholestasis syndrome 1 (LCS1/Aagenaes syndrome).” Scand J Clin Lab Invest 78(7–8): 566–574.
The risks of developing energy or nutrient deficits are of great concern in infants and children with the rare lymphoedema cholestasis syndrome 1 (LCS1)/Aagenaes syndrome. In adolescents and adults, it is not known whether LCS1 patients need specific dietary advice outside periods of cholestasis. The primary objective of the present study was to evaluate the progression of the liver disease and nutritional status in patients with LCS1 over a period of nine years. Dietary and biochemical data were obtained for patients and healthy controls in two cross-sectional studies, a baseline (2000) and a follow-up study (2009). Thirteen patients above 18 years of age with LCS1 (65%) were included (six females). Dietary intake and biochemical measures were stable in the patients from baseline until follow-up. Compared to healthy controls, the patients had significantly higher serum levels of alkaline phosphatase (p = .015 and p = .002), gamma-glutamyltransferase (p = .001 and p < .001), total bile acids (p = .037 and p = .016), and fibrinogen (p = .046 and p < .001) and lower albumin (p = .033 and p < .001) and alpha-tocopherol (p = .011 and p = .003) at baseline and follow-up. Despite stable liver function, the presence of a low grade of hepatobiliary dysfunction in these patients was suggested. Patients with LCS1 had a nutritional status similar to healthy controls, with no clinical deterioration of liver function during the nine-year period. The findings presented in this paper support that more than 50% of patients with LCS1 can expect a normal lifespan.
Esposito, C., et al. (2019). “Indocyanine Green Fluorescence Lymphography: A New Technique to Perform Lymphatic Sparing Laparoscopic Palomo Varicocelectomy in Children.” J Laparoendosc Adv Surg Tech A. [EPub Jan 25]
BACKGROUND: Laparoscopic Palomo varicocelectomy is one the most common approaches adopted to treat pediatric varicocele, but postoperative hydrocele still remains a potential problem with this procedure. This study aimed to evaluate the outcome of a new technique of lymphography using indocyanine green (ICG)-enhanced fluorescence to perform lymphatic sparing laparoscopic Palomo varicocelectomy. PATIENTS AND METHODS: The records of 25 patients who underwent laparoscopic left varicocelectomy in our unit from March 2017 to March 2018 were retrospectively evaluated. The average patients' age was 13.7 years (range 12–16). All patients had a high degree varicocele associated with left testicular hypotrophy and symptoms. All procedures were performed in laparoscopy using three trocars. After trocars' positioning, 2 mL of ICG solution was directly injected into the left testicle. Using ICG fluorescence, the lymphatic vessels were clearly identified and spared, and then the entire spermatic bundle was clipped and divided according to Palomo's principle. RESULTS: The average operative time was 18 minutes (range 10–25). No conversions to open surgery and no allergy or other adverse reactions induced by ICG were reported. At a maximum follow-up of 18 months, no recurrence of varicocele or postoperative hydrocele was recorded. CONCLUSIONS: Our preliminary experience showed that ICG fluorescence lymphography is a safe and effective option to perform lymphatic sparing laparoscopic Palomo varicocelectomy in children and adolescents with high degree varicocele. The intratesticular injection of ICG and use of fluorescence vision allowed identification of lymphatic vessels in 100% of cases. No allergy to ICG or postoperative hydrocele was reported in our experience.
Garmy-Susini, B. (2019). “Hormone therapy outcome in lymphedema.” Aging (Albany NY) 11(2): 291–292.
Gutierrez, C., et al. (2019). “Head and Neck Lymphedema: Treatment Response to Single and Multiple Sessions of Advanced Pneumatic Compression Therapy.” Otolaryngol Head Neck Surg: 194599818823180.
Ten head and neck cancer survivors diagnosed with head and neck lymphedema (HNL) were imaged using near-infrared fluorescence lymphatic imaging (NIRFLI) prior to and immediately after an initial advance pneumatic compression device treatment and again after 2 weeks of daily at-home use. Images assessed the impact of pneumatic compression therapy on lymphatic drainage. Facial composite measurement scores assessed reduction/increase in external swelling, and survey results were obtained. After a single pneumatic compression treatment, NIRFLI showed enhanced lymphatic uptake and drainage in all subjects. After 2 weeks of daily treatment, areas of dermal backflow disappeared or were reduced in 6 of 8 subjects presenting with backflow. In general, reductions in facial composite measurement scores tracked with reductions in backflow and subject-reported improvements; however, studies are needed to determine whether longer treatment durations can be impactful and whether advanced pneumatic compression can be used to ameliorate backflow characteristic of HNL.
Hespe, G. E., et al. (2019). “Baseline Lymphatic Dysfunction Amplifies the Negative Effects of Lymphatic Injury.” Plast Reconstr Surg 143(1): 77e–87e.
BACKGROUND: Genetic mutations and obesity increase the risk of secondary lymphedema, suggesting that impaired lymphatic function before surgical injury may contribute to disease pathophysiology. Previous studies show that obesity not only decreases lymphatic function, but also markedly increases pathologic changes, such as swelling, fibroadipose deposition, and inflammation. However, although these reports provide circumstantial evidence supporting the hypothesis that baseline lymphatic defects amplify the effect of lymphatic injury, the mechanisms regulating this association remain unknown. METHODS: Baseline lymphatic morphology, leakiness, pumping, immune cell trafficking, and local inflammation and fibroadipose deposition were assessed in wild-type and Prox1-haploinsufficient (Prox1) mice, which have previously been shown to have abnormal vasculature without overt evidence of lymphedema. In subsequent experiments, wild-type and Prox1 mice underwent popliteal lymph node dissection to evaluate the effect of lymphatic injury. Repeated testing of all variables was conducted 4 weeks postoperatively. RESULTS: At baseline, Prox1 mice had dilated, leaky lymphatic vessels corresponding to low-grade inflammation and decreased pumping and transport function, compared with wild-type mice. Popliteal lymph node dissection resulted in evidence of lymphedema in both Prox1 and wild-type mice, but popliteal lymph node dissection-treated Prox1 mice had increased inflammation and decreased lymphatic pumping. CONCLUSIONS: Subclinical lymphatic dysfunction exacerbates the pathologic changes of lymphatic injury, an effect that is multifactorial and related to increased lymphatic leakiness, perilymphatic accumulation of inflammatory cells, and impaired pumping and transport capacity. These findings suggest that preoperative testing of lymphatic function may enable clinicians to more accurately risk-stratify patients and design targeted preventative strategies.
Iker, E., et al. (2019). “Characterizing Lower Extremity Lymphedema and Lipedema with Cutaneous Ultrasonography and an Objective Computer-Assisted Measurement of Dermal Echogenicity.” Lymphat Res Biol. [EPub Jan 7]
BACKGROUND: Sonographic findings differ in patients with primary lipedema from those with lymphedema. This project was designed to quantify those differences and objectively characterize findings of lipedema and lymphedema in the lower extremity. METHODS AND RESULTS: Patients with a clinical diagnosis of ISL stage I-II lipedema or lower extremity lymphedema that received ultrasound evaluation were included in this study. Thickness and echogenicity of the skin and subcutaneous fat layer were measured at the level of the ankle, calf, and thigh in each patient. The cohort analyzed included 12 patients with lipedema (12 lower extremities) and 10 patients with unilateral lymphedema (10 lower extremities with lymphedema and 8 lower extremities used as controls). Mean skin thickness of the ankle and calf was greatest in the lymphedema group compared to those with lipedema or controls (p < 0.01 and p < 0.01, respectively). The mean thickness of the subcutaneous fat layer of the thigh was greatest in those with lipedema (p < 0.01). Mean dermal to subcutaneous fat echogenicity ratio was decreased in those with lymphedema (ankle, 0.91; calf, 1.05; thigh, 1.19) compared to lipedema (ankle, 1.36; calf, 1.58; thigh, 1.54) and control (ankle, 1.26; calf, 1.54; thigh, 1.56) (p < 0.01, p < 0.01, and p = 0.02, respectively). CONCLUSIONS: Lymphedema appears to be associated with increased skin thickness and dermal hypoechogenicity, particularly in the distal lower extremity, compared to lipedema or controls. Conversely, lipedema may be associated with increased thickness and hypoechogenicity of the subcutaneous fat. Overall, these findings suggest that ultrasound may be an effective tool to differentiate these diseases and potentially guide treatment.
Kanth, A. M., et al. (2019). “Surgical Management of Pediatric Lymphedema: A Systematic Review.” J Reconstr Microsurg. [EPub Feb 27]
INTRODUCTION: Lymphedema is a rare, progressive, and debilitating condition caused by failure of the lymphatic system to adequately drain the protein-rich fluid exiting the capillaries. Conservative management is often emphasized in pediatric patients, resulting in a paucity of literature describing surgical treatment in this population. METHODS: A systematic review was performed using PubMed, ScienceDirect, and Google Scholar to identify all studies describing surgical management of lymphedema in the pediatric population. RESULTS: Of the 343 relevant articles identified, 14 met the criteria for full review. Articles were divided into the following treatment categories: genital lymphedema, excisional procedures for extremity lymphedema, and physiologic procedures for extremity lymphedema. Outcomes for genital lymphedema were overall positive. For extremity lymphedema, excisional procedures yielded good results overall and included the majority of patients in this study. Physiologic procedures had mixed outcomes in the small population included in this study, but definitive conclusions cannot be drawn due to the paucity of existing data. CONCLUSION: While conservative management of pediatric lymphedema is well described, the literature remains sparse regarding surgical treatment. Further studies are needed to evaluate efficacy and outcomes in all three categories in this population.
Li, B. (2018). “Mei R. Fu: mHealth facilitates real-time detection and prediction of lymphedema.” Mhealth 4: 53.
Mari, J., et al. (2019). “Pediatric localized intestinal lymphangiectasia treated with resection.” Int Med Case Rep J 12: 23–27.
Introduction: Primary intestinal lymphangiectasia (PIL) is a very rare disorder usually diagnosed before the third year of life or later in adulthood, presenting with pitting edema, hypoproteinemia and low immunoglobulin levels. The location and the extent of the affected bowel greatly influence the clinical manifestation. The localized or segmental form of PIL is extremely rare with only five pediatric cases reported worldwide. Case presentation: A 10 year-old Caucasian boy presented with 3 months history of recurrent abdominal pain and a 1 month history of diarrhea. An ultrasound scan was performed on two separate occasions 10 days apart, revealing a growing cystic mass on the right side of the abdomen, in front of the psoas muscle. Subsequently an MRI scan confirmed that the mass originated from the mesenteries and infiltrates a short segment of the small bowel. Surgical resection of the affected segment was performed. Histopathological examination of the removed segment of ileum was consistent with intestinal lymphangiectasia. We could not identify any associated genetic syndromes or any other conditions that could have caused secondary intestinal lymphangiectasia. The patient's recovery from surgery was uneventful and no recurrence was observed in the following 4 years. Conclusion: Despite being a benign condition, mortality of PIL can be as high as 13% due to the difficulties associated with the management of the disease. PIL should be considered as a rare but potential cause for an abdominal mass, even in the older child, when cystic mesenterial involvement might be seen on ultrasound or MRI. In selected cases of PIL affecting only a short segment of the bowel or following unsuccessful conservative treatment, surgical resection of the affected bowel segment can be curative.
Mosti, G. and A. Cavezzi (2019). “Compression therapy in lymphedema: Between past and recent scientific data.” Phlebology: 268355518824524.
AIM: To extrapolate and discuss the scientific data on compression in lymphedema treatment, so to review old and innovative concepts about pressure, stiffness and other interplaying factors related to its efficacy and comfort. MATERIAL AND METHODS: Narrative review based on search in Medline/Google Scholar through key-words related to compression in lymphedema. RESULTS: Currently available literature lacks relevant details about data on protocol, devices, techniques, interface pressure, stiffness, as well as biases are represented by the different descriptions to present the outcomes. More recent evidence from adjustable wrap devices and elastic garments question the need for high pressure (especially for the upper limb) and stiffness in lymphedema treatment. CONCLUSIONS: At present time a very strong compression pressure exerted by material with high stiffness seem to be questionable in lymphedema treatment. A low pressure provides the best outcomes in arm lymphedema, while a pressure in the range of 40–60 mm Hg seems to provide higher efficacy in lower limb lymphedema, provided it is maintained overtime. A high stiffness seems to be unnecessary to treat chronic edema. Future clinical trials, including proper description of treatment methodology and adequate investigating instrumental tools, are awaited to possibly corroborate the conclusive outcomes of our review.
Nganga, E. C. and K. Makhdomi (2019). “Comparison of quantitative analysis to qualitative analysis for interpretation of lower-limb lymphoscintigraphy.” World J Nucl Med 18(1): 36–41.
Qualitative analysis of lymphoscintigrams is subject to wide variability and may miss subtle differences in ilioinguinal uptake between normal and abnormal limbs. This study compared quantitative analysis to qualitative analysis of lower-limb lymphoscintigraphy in diagnosing lymphedema. Fifty-two lymphoscintigrams performed using standardized protocol, 99-metastable technetium nanocolloid intradermal injection at the first interdigital space, were analyzed quantitatively. Fifty-three normal and 51 abnormal limbs were analyzed. For each limb, a region of interest (ROI) was drawn around the injection site, and ilioinguinal nodes on the 1.5 h static images and the counts in these ROIs were recorded. Percentage ilioinguinal nodes uptake was then computed. Analysis of variance (ANOVA) was performed to determine the difference in ilioinguinal uptake between normal and abnormal limbs. Specificity and sensitivity were calculated and the figures were used to plot a receiver operator characteristic (ROC) curve. Thirty-six females and 16 males (104 limbs) were analyzed. ANOVA revealed a significant difference between the mean uptake in normal (19.7%) and abnormal limbs (5.5%) (F = 81, P < 0.001). ROC had a maximal area under the curve of 0.924 (P < 0.001). The significant difference in the means of ilioinguinal uptake between normal and lymphedema limbs infers reduced lymphatic function. Ilioinguinal lymph node uptake is thus a reliable parameter in quantitative analysis of lymphoscintigrams.
Santulli, G. (2018). “The lymphatic border patrol outwits inflammatory cells in myocardial infarction.” Sci Transl Med 10(451).
Lymphangiogenesis modulates inflammation by clearing immune cells in the infarcted heart in a lymphatic vessel endothelial hyaluronan receptor 1 (LYVE-1)-dependent process to ameliorate cardiac dysfunction.
Singhal, D., et al. (2019). “Technological Advances in Lymphatic Surgery: Bringing to Light the Invisible.” Plast Reconstr Surg 143(1): 283–293.
Lymphatic surgery has become an integral and flourishing component of the field of plastic surgery. The diversity of ongoing technological innovations in perioperative imaging, including intraoperative dyes and cameras, allows plastic surgeons to work at the supermicrosurgical level. This study aims to highlight innovations that have shaped and will continue to revolutionize the perioperative management of the lymphatic surgery patient in the future. As additional advances emerge, we need a systematic and objective way to evaluate the efficacy and clinical integration readiness of such technologies. Undoubtedly, these technologies will help lymphatic surgery trend toward increasing objectivity, which will be critical for continued evolution and advancement.
Sood, N. and M. Mukherjee (2018). “Dermal Lymphatic Invasion: A Rare Feature in Benign Intradermal Nevus.” Int J Appl Basic Med Res 8(4): 253–255.
The present case describes classical intradermal nevus with intralymphatic nevus cell emboli. A 13-year-old boy presented with black colored macule on the shin 1 cm in diameter which was gradually increasing in size. Histopathology of the lesion was typical of an intradermal melanocytic nevus. The most notable feature of this case, however, was an occasional aggregate of nevus cells within a lymphatic vessel of the upper dermis. The nevus cells within lymphatic lumen had morphological features of type A nevus cells. The cells were roundtocuboidal, exhibited abundant cytoplasm with welldefined cell borders and formed nests. These nevus cell aggregates were surrounded by flattened endothelial cells. Due to its rarity, a lymphatic nevus cell embolus creates diagnostic issues for pathologists. This observation must not be interpreted as evidence of malignancy but significant as a rare histological feature. In other words, the nevus cells might have been transported through the lymphatic vessels as a “benign metastasis.”
Suzuki, Y., et al. (2019). “Comparison of patency rates of lymphaticovenous anastomoses at different sites for lower extremity lymphedema.” J Vasc Surg Venous Lymphat Disord 7(2): 222–227.
OBJECTIVE: Lymphaticovenous anastomosis (LVA) is one of the surgical treatments of lymphedema. However, only a few reports have evaluated LVA directly. This study aimed to evaluate the patency of LVA using indocyanine green fluorescence lymphography and to determine the optimal anastomosis site in patients with lower extremity lymphedema. METHODS: Thirty-six patients, with a total of 123 anastomoses for lower extremity lymphedema including 3 cases of idiopathic lymphedema, who underwent LVA for the first time between March 2014 and March 2017 were selected for enrollment in this study. The patency of the anastomoses was evaluated using PDE-neo (Hamamatsu Photonics, Hamakita, Japan) by injecting indocyanine green into the subcutaneous tissue at 6 months postoperatively. The site of anastomosis was the intersection point of the lymphatic vessel and vein, which was identified preoperatively. To determine the best surgical location, the anastomosis site was classified into the joint area (ankle and knee) and nonjoint area (dorsum and lower leg). The anastomosis was evaluated as either patent or nonpatent. RESULTS: Patency was confirmed in 37 of the 76 (49%) anastomoses at the joint area and 12 of the 47 (26%) at nonjoint areas (P = .01). CONCLUSIONS: The patency rate was significantly higher around the joint area than at the nonjoint areas. LVA around the joint area is recommended to ensure favorable technical and surgical outcomes for patients with lower extremity lymphedema.
Teven, C. M., et al. (2019). “Management of High Output Chyle Leak after Harvesting of Vascularized Supraclavicular Lymph Nodes.” Plast Reconstr Surg. [EPub Jan 21]
Vascularized lymph node transfer (VLNT) is a physiologic microsurgical technique used for the treatment of lymphedema. As VLNT is becoming more common, it is essential that we are aware of all potential complications associated with VLNT and know how to avoid and manage them when they do occur.We recently encountered a complication after supraclavicular vascularized lymph node transfer (SCVLNT) that has not been previously reported. A patient developed a recalcitrant high output (>500 mL/day) chyle leak in the neck donor site after harvesting of SCVLNT. In this paper, we share our experience with massive chyle leak and review the management strategies of how to effectively avoid and treat this potentially dangerous complication. This review of a previously unreported complication of SCVLNT is timely and important as this procedure is increasingly being offered to patients, and surgeons performing these procedures should be familiarly with effectively managing this potentially dangerous complication.
Viswanathan, P. and I. Novak (2017). “Intestinal Lymphangiestasia With Hennekam Syndrome.” J Pediatr Gastroenterol Nutr 65(6): e133.
Yuan, Y., et al. (2019). “The Effect and Mechanism of Negative Pressure Wound Therapy on Lymphatic Leakage in Rabbits.” J Surg Res 235: 329–339.
BACKGROUND: Lymphatic leakage is one of the severe complications after lymphadenectomy. However, efficient treatment it still unclear. MATERIALS AND METHODS: We employed inguinal lymphadenectomy and saphenous lymphatic vessel excision to establish a inguinal lymphatic leakage rabbit model. Rabbits with bilateral lymphatic leakage were divided in two groups, which were subject to negative pressure wound therapy (NPWT) on right sides and dressing change on left sides, respectively. Following 7–11 d of treatment, skin thickness and drainage volume were measured. Western blot and RT-PCR were used for analyzing the VEGF-C level. Tissues of wound were dissected and subject to anti-LYVE-1 immunohistochemical for lymphatic average positive staining area percentage and the ratio of lymphatic lumen area evaluation. RESULTS: Our lymphatic leakage model showed significant lymph stasis, delayed wound healing, and skin swelling and was confirmed by methylene blue instillation. Using this rabbit model, we found that NPWT could largely promote wound healing and resolution of skin edema. Compared with the dressing change group, the thickness of the dermis layer in the NPWT group was significantly reduced. Western blot and RT-PCR analysis showed a decrease of VEGF-C in the NPWT group. The immunohistochemical result of the NPWT group did not show a significant change in lymphatic average positive staining area percentage, whereas the ratio of lymphatic lumen area was significantly decreased, suggesting that NPWT treatment can significantly compress the dilated lymphatic vessels. CONCLUSIONS: We successfully established the first clinically relevant lymphatic leakage model in rabbits. NPWT can be an effective treatment for lymphatic leakage via reducing edema and lymphatic stasis by compressing dilated lymph vessels and promoting lymphatic drainage.
Oncology
Ammitzboll, G., et al. (2019). “Effect of progressive resistance training on health-related quality of life in the first year after breast cancer surgery - results from a randomized controlled trial.” Acta Oncol: 1–8.
AIMS: To examine the effect of progressive resistance training (PRT) on health related quality of life and a predefined symptom cluster of pain-sleep-fatigue. METHODS: This study was a planned secondary analysis of a randomized controlled trial examining the effect of PRT on prevention of arm lymphedema in a population of women between 18 and 75 years undergoing breast cancer surgery with axillary lymph node dissection. Participants were allocated by computer randomization to usual care control or a PRT intervention in a 1:1 ratio. The intervention, initiated in the third post-operative week, consisted of three times PRT per week, supervised in groups in the first 20 weeks, and self-administered in the following 30 weeks. Questionnaire assessments were made at baseline, 20 weeks and 12 months, with the European Organization for Research and Treatment in Cancer Core questionnaire (EORTC QLQ C30) and the Functional Assessment of Chronic Illness Therapy-(FACIT) fatigue questionnaire. The symptom cluster of pain-sleep-fatigue was measured with a constructed score adding EORTC C30 subscales of insomnia, pain, and fatigue. Data were treated as repeated measurements and analyzed with mixed models. RESULTS: Among 158 recruited participants, we found a clinically relevant increased emotional functioning with nine points at both follow-ups (p = .02), and 16 and 11 points at 20 weeks and 12 months respectively (p = .04) in social functioning. Furthermore, in the subgroup of women with the symptom cluster pain-sleep-fatigue present at baseline, a significant effect was found for global health status (p = .01) and social functioning (p = .02). CONCLUSION: To our knowledge, this is the first study to report clinically relevant effects of PRT on social and emotional functioning in the first postoperative year after breast cancer surgery. Furthermore, a subgroup of women with the pain-sleep-fatigue symptom cluster had particular benefit from PRT on global health status and social functioning.
Belhassine, M., et al. (2018). “Gastric adenocarcinoma revealed by atypical pulmonary lymphangitic carcinomatosis.” J Gastrointest Oncol 9(6): 1207–1212.
Pulmonary lymphangitic carcinomatosis (PLC) is a well-known form of tumour metastasis to the pulmonary lymphatic system or to the adjacent interstitial tissue resulting in thickening of the bronchovascular bundle and septa. Another type of tumour metastasis to the lung involves the pulmonary vascular system and is known as pulmonary tumour thrombotic microangiopathy (PTTM). In this article, we will describe the unusual case of a young Chinese woman with gastric adenocarcinoma revealed by atypical radiographic lesions consistent with both PLC and PTTM. We will discuss the existing evidence and hypotheses about the pathophysiology of both conditions.
Brahma, B. and T. Yamamoto (2019). “Breast cancer treatment-related lymphedema (BCRL): An overview of the literature and updates in microsurgery reconstructions.” Eur J Surg Oncol. [EPub Jan 4]
Breast cancer is the most common cancer in Dharmais hospital. The treatment can give rise to breast cancer treatment-related lymphedema (BCRL) that will cause significant morbidities. Based on author's (BB) patient series in Dharmais hospital, BCRL occurred in 27.7% after axillary lymph nodes dissection (ALND). The development of diagnostic modalities as well as lymphatic microsurgery have become promising instruments for lymphedema treatment. To date, modern approach of lymphedema care and surgical intervention have not been recognized and established in Indonesia. A literature review in this field is needed to overcome our limitation in BRCL or lymphedema management.
Chen, Y., et al. (2018). “Podoplanin+ tumor lymphatics are rate limiting for breast cancer metastasis.” PLoS Biol 16(12): e2005907.
Metastatic dissemination employs both the blood and lymphatic vascular systems. Solid tumors dynamically remodel and generate both vessel types during cancer progression. Lymphatic vessel invasion and cancer cells in the tumor-draining lymph nodes (LNs) are prognostic markers for breast cancer metastasis and patient outcome, and tumor-induced lymphangiogenesis likely influences metastasis. Deregulated tumor tissue fluid homeostasis and immune trafficking associated with tumor lymphangiogenesis may contribute to metastatic spreading; however, the precise functional characterization of lymphatic endothelial cells (LECs) in tumors is challenged by the lack of specific reagents to decipher their rate-limiting role in metastasis. Therefore, we generated novel transgenic mice (PDPN promoter-driven Cre recombinase transgene [PDPN-Cre] and PDPN promoter-driven thymidine kinase transgene [PDPN-tk]) that allow for the identification and genetically controlled depletion of proliferating podoplanin (Pdpn)-expressing LECs. We demonstrate that suppression of lymphangiogenesis is successfully achieved in lymphangioma lesions induced in the PDPN-tk mice. In multiple metastatic breast cancer mouse models, we identified distinct roles for LECs in primary and metastatic tumors. Our findings support the functional contribution of primary tumor lymphangiogenesis in controlling metastasis to axillary LNs and lung parenchyma. Reduced lymphatic vessel density enhanced primary tumor lymphedema and increased the frequency of intratumoral macrophages but was not associated with a significant impact on primary tumor growth despite a marked reduction in metastatic dissemination. Our findings identify the rate-limiting contribution of the breast tumor lymphatic vessels for lung metastasis.
Co, M., et al. (2019). “Cutaneous Angiosarcoma Secondary to Lymphoedema or Radiation Therapy - A Systematic Review.” Clin Oncol (R Coll Radiol) 31(4): 225–231.
AIMS: Secondary angiosarcoma is known to be associated with lymphoedema or radiation after cancer treatment. This systematic review aims to evaluate the clinical features and outcomes of secondary angiosarcoma commonly arising after breast cancer treatment. MATERIALS AND METHODS: A systematic review was carried out according to the PRISMA protocol. Medline, EMBASE, CINAHL and Cochrane databases were searched for English articles to April 2018 with predefined strategy. Retrieved studies were independently screened and rated for relevance. Data were extracted by two researchers. RESULTS: There were 72 secondary angiosarcomas of the limbs. Most patients (n = 68, 94.4%) had a history of lymphoedema. The median latent period was 15 years (range 3–40 years). Thirty-eight (52.8%) patients received wide excision or amputation as a treatment for the angiosarcoma, two (2.8%) patients received isolated limb perfusion and one (1.4%) patient received systemic chemotherapy. The remaining patients received palliative care/undocumented treatment. The pooled median duration to mortality was 10.5 months (range 1–144 months). Of note, obesity was documented in seven (9.7%) patients. There were 83 breast angiosarcomas; all with known breast cancer history. Thirty-one (37.3%) patients received mastectomy as breast cancer treatment. Fifty-four (65.1%) patients had a history of adjuvant radiotherapy for the primary breast cancer. The median latent period was 6 years (range 2–50 years); the median size was 40 mm (range 8–200 mm). Forty-one (49.4%) patients received wide excision, 19 (22.9%) patients received completion mastectomy and 23 (27.7%) patients have undocumented treatment for angiosarcoma. The pooled median duration to mortality was 31 months (range 6–168 months). CONCLUSION: Angiosarcoma in lympedematous upper limbs or after breast cancer irradiation remains uncommon. However, its long latency and high mortality warrant long-term vigilant surveillance.
Commerford, C. D., et al. (2018). “Mechanisms of Tumor-Induced Lymphovascular Niche Formation in Draining Lymph Nodes.” Cell Rep 25(13): 3554–3563 e3554.
Enlargement of the lymphatic vascular network in tumor-draining lymph nodes (LNs) often precedes LN metastasis, likely providing a lymphovascular niche for tumor cells. We investigated morphological and molecular changes associated with the lymphatic remodeling process, using the 4T1 breast cancer and B16F10 melanoma models. Lymphatic expansion in tumor-draining LNs is mediated by sprouting and proliferation of lymphatic endothelial cells (LECs) as early as 4 days after tumor implantation. RNA sequencing revealed an altered transcriptional profile of LECs from tumor-draining compared to naive LNs with similar changes in both tumor models. Integrin alphaIIb is upregulated in LECs of tumor-draining LNs and mediates LEC adhesion to fibrinogen in vitro. LEC-associated fibrinogen was also detected in LNs in vivo, suggesting a role of integrin alphaIIb in lymphatic remodeling. Together, our results identify specific responses of LN LECs to tumor stimuli and provide insights into the mechanisms of lymphovascular niche formation in tumor-draining LNs.
Hasenoehrl, T., et al. (2019). “Resistance exercise and breast cancer related lymphedema - a systematic review update.” Disabil Rehabil: 1–10.
BACKGROUND: Purpose of this systematic review update was analyzing resistance exercise (RE) intervention trials in breast cancer survivors (BCS) regarding their effect on breast cancer-related lymphedema (BCRL) status. Articles published until 31 September 2017 were included. METHODS: A systematic literature search was conducted utilizing PubMed, MEDLINE, and EMBASE databases. Included articles were analyzed regarding their level of evidence and their methodological quality using the Cochrane risk of bias tool. RESULTS: Altogether, 23 articles could be included of which 16 were independent RE intervention studies and seven additional articles. Lymphedema assessment was so heterogeneous that conduction of a thorough meta-analysis regarding lymphedema status was still impossible. In all but one study, which reported a small but methodologically weak increase in arm volume, no negative effects of RE on BCRL was recorded. CONCLUSIONS: RE seems to be a safe exercise intervention for BCS and not to be harmful concerning the risk of lymphedema. Lymphedema assessment methods that allow for a qualitative analysis of arm tissue composition should be favored. Implications for rehabilitation Breast cancer-related lymphedema affects a considerable proportion of breast cancer patients and is debilitating on the physical, functional, social, and psychological domain. At the current time breast cancer related lymphedema is incurable but well manageable by a number of physical therapy modalities, especially complete decongestive therapy (CDT). One of the encouraging treatment methods is resistance exercise.
Invernizzi, M., et al. (2019). “Breast Cancer Systemic Treatments and Upper Limb Lymphedema: A Risk-Assessment Platform Encompassing Tumor-Specific Pathological Features Reveals the Potential Role of Trastuzumab.” J Clin Med 8(2).
Breast cancer related lymphedema (BCRL) is frequent but strategies for an individualized risk assessment are lacking. We aimed to define whether tumor-specific pathological features, coupled with clinical and therapeutic data, could help identify patients at risk. Data from 368 patients with node-positive breast cancers were retrospectively collected, including 75 patients with BCRL (0.4(-)25.6 years follow-up). BCRL was assessed during the standard follow-up oncology visits using the circumferential measurement. Clinicopathologic and therapeutic factors associated with BCRL were integrated into a Cox proportional hazards regression model. Lymphovascular invasion (LVI) was more common in BCRL patients (n = 33, 44% vs. n = 85, 29%, p = 0.01), akin extra nodal extension (ENE) of the metastasis (n = 57, 76% vs. n = 180, 61%, p = 0.02). Sentinel lymph node excision without axillary dissection and extra-axillary radiotherapy were BCRL-unrelated. A higher number of BCRL-positive patients were treated with taxane-based chemotherapy with or without trastuzumab, compared to BCRL-negative patients (p < 0.01). Treatment with trastuzumab and/or taxanes, adjusted for systemic infections, laterality, therapy, and pathological features (i.e., LVI and ENE), had a significant impact in BCRL-free survival (p < 0.01). This work offers new insights on BCRL risk stratification, where the integration of clinical, therapeutic, and tumor-specific pathological data suggests a possible role of anti-human epidermal growth factor receptor 2 (HER2) therapy in BCRL pathogenesis.
Michelotti, A., et al. (2018). “Tackling the diversity of breast cancer related lymphedema: Perspectives on diagnosis, risk assessment, and clinical management.” Breast 44: 15–23.
Breast cancer related lymphedema (BCRL) develops as a consequence of surgical treatment and/or radiation therapy in a significant number of breast cancer patients. The etiology of this condition is multifactorial and has not yet been completely elucidated. Risk factors include high body mass index, radical surgical procedures (i.e., mastectomy and axillary lymph node dissection), number of lymph nodes removed and number of metastatic lymph nodes, as well as nodal radiation, and chemotherapy. However, these predisposing factors explain only partially the BCRL occurrence, suggesting the possible involvement of individual determinants. Despite the implementation of conservative approaches, BCRL still remains in a proportion of cases an incurable and progressive condition with major physical and psychological implications. To date, diagnostic methods and staging systems lack uniformity, leading to a possible underestimation of the real incidence of this condition, decreasing early detection and thus the possibility of an effective treatment. Several preventive and therapeutic options are available, both conservative and surgical, but are not included in a standardized intervention protocol, tailored on patient's specific characteristics. In this review, we provide a comprehensive overview of the current state-of-knowledge of BCRL management, novel advantages in the assessment of pre-operative evaluation and risk prediction and discuss strengths and weaknesses of diagnostic and treatment strategies currently accessible in clinical practice.
Naymagon, L., et al. (2019). “Severe Protein-Losing Enteropathy Due to an Indolent Splenic Lymphoma: Case Report and Review of the Literature.” Clin Lymphoma Myeloma Leuk. [EPub Jan 3]
Rockson, S. G. (2019). “Lymphedema after Breast Cancer Treatment.” N Engl J Med 380(7): 694.
Salehi, S., et al. (2019). “Lymphedema, serious adverse events, and imaging 1 year after comprehensive staging for endometrial cancer: results from the RASHEC trial.” Int J Gynecol Cancer 29(1): 86–93.
BACKGROUND AND OBJECTIVES: In the Robot Assisted Surgery for High Risk Endometrial Cancer (RASHEC) trial, patients with high-risk endometrial cancer were randomly assigned to robot-assisted laparoscopic surgery (RALS) or laparotomy for pelvic and infrarenal para-aortic lymph node dissection. We here report on self-reported lower limb lymphedema (LLL), lymphocyst formation, ascites, and long-term serious adverse events 12 months after surgery. PATIENTS AND METHODS: Patients were enrolled between 2013 and 2016, and 96 patients were included in the per protocol analysis, evenly distributed between RALS and laparotomy. Self-reported LLL was recorded using the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire for endometrial cancer-EN24, assessed before and 12 months after surgery. Computed tomography was assessed at baseline, 3, and 12 months. Medical charts were reviewed for serious adverse events and hospital admissions 31 to 365 days after surgery. RESULTS: At 12 months after laparotomy and RALS, 61% and 50% patients, respectively, reported LLL (p = 0.31). In univariate analysis, the mean score of LLL at 12 months was significantly higher for laparotomy than for RALS (p < 0.05) and for those without abdominal drainage (p = 0.02), but was not independently associated with LLL in the multivariate analysis. Imaging showed no significant difference in lymphocyst formation or ascites between surgical modalities. No difference was found in serious adverse events and admissions to hospital for any reason. There was no agreement between lymphocyst formation or ascites and self-reported LLL. CONCLUSION: Follow-up 1 year after comprehensive surgical staging for high-risk endometrial cancer showed no differences in self-reported LLL, findings on imaging, or SAE between laparotomy and robot-assisted surgery.
Seo, K. S., et al. (2019). “The New Possibility of Lymphoscintigraphy to Guide a Clinical Treatment for Lymphedema in Patient With Breast Cancer.” Clin Nucl Med 44(3): 179–185.
OBJECTIVES: Lymphedema is a chronic disease that occurs frequently after breast cancer treatment. For the treatment of lymphedema, surgical approach such as vascularized lymph node transfer and super-microscopic lymphovenous anastomosis surgery is well established. Complex decongestive therapy (CDT) and sympathetic ganglion block (SGB) are two non-surgical therapeutic options. This study aimed to evaluate the effectiveness of lymphoscintigraphy in guiding the selection of the optimal non-surgical treatment in lymphedema. METHODS: A total of 81 lymphedema patients who underwent lymphoscintigraphy and were treated with CDT or SGB were retrospectively evaluated. The parameters for the lymphoscintigraphic findings included the extent of dermal backflow (small extent/large extent groups), the level of lymphatic flow (trunk flow pattern/upper arm-restricted pattern/forearm-restricted pattern groups), and the visualization of lymph nodes (visualized/non-visualized groups). The change in the circumferential difference between the two sides of the body at the upper arm and forearm was used as the clinical outcome variable. Paired comparison and group comparison analysis were conducted. RESULTS: Of 81 patients, 41 received CDT and 40 received SGB. There were no significant differences in demographic data between the CDT and SGB groups. Both CDT and SGB had a significant therapeutic effect. Upper arm edema was more significantly reduced after SGB than after CDT in the small extent group (P = 0.004), the forearm-restricted pattern group (P = 0.002), and the non-visualized group (P = 0.018). In the other groups, SGB and CDT showed comparable therapeutic effects without statistical differences. CONCLUSION: SGB was found to have a better therapeutic effect in the lymphedema patients with specific lymphoscintigraphic findings compared with CDT. Lymphoscintigraphy may be helpful in selecting the appropriate approach to lymphedema treatment. Further well-designed prospective studies are warranted to validate the findings of this study.
Tashiro, K., et al. (2019). “Flap reconstruction after groin and medial thigh sarcoma resection reduces the risk of lower-extremity lymphedema.” J Plast Reconstr Aesthet Surg. [EPub Jan 12]
van Leeuwen, F. W. B., et al. (2019). “Technologies for image-guided surgery for managing lymphatic metastases in prostate cancer.” Nat Rev Urol. [EPub Jan 15]
One of the challenges for the surgical management of prostate cancer is the lymphatic spread of metastases. Lymph node metastases vary in size (micrometastases (<2 mm) or macrometastases (>2 mm)), and their interactions with the lymphatic environment differ (whether they are hypoxic or connected to blood flow). Thus, devising a universal imaging system and an image-guided surgical approach that supports the resection of all affected lymph nodes is difficult. Two complementary approaches to identifying affected lymph nodes have been described as alternatives to performing a traditional pelvic lymph node dissection: lymphatic mapping using radioguidance (the most widely applied modality), fluorescence guidance, integrated hybrid radioguidance and fluorescence guidance or magnetic guidance; and surgery guided by radiolabelled prostate-specific membrane antigen. Careful patient selection using preoperative imaging seems to be a crucial aspect in determining whether one of the individual image-guided surgery procedures alone would be optimal or whether a combination would be considered to be the most desirable course of action. The successful implementation and dissemination of both lymph-node-targeted and disease-targeted procedures are very much reliant on ongoing technical developments in the field and their standardization and interpretation. However, when these innovative surgical procedures are fully refined, evaluation of their influence on oncological outcome is imperative.
Wang, J., et al. (2019). “Fucoxanthin inhibits tumour-related lymphangiogenesis and growth of breast cancer.” J Cell Mol Med 23(3): 2219–2229.
Tumour lymphangiogenesis plays an important role in promoting the growth and lymphatic metastasis of tumours. The process is associated with cell proliferation, migration and tube-like structure formation in lymphatic endothelial cells (LEC), but no antilymphangiogenic agent is currently used in clinical practice. Fucoxanthin is a material found in brown algae that holds promise in the context of drug development. Fucoxanthin is a carotenoid with variety of pharmacological functions, including antitumour and anti-inflammatory effects. The ability of fucoxanthin to inhibit lymphangiogenesis remains unclear. The results of experiments performed as part of this study show that fucoxanthin, extracted from Undaria pinnatifida (Wakame), inhibits proliferation, migration and formation of tube-like structures in human LEC (HLEC). In this study, fucoxanthin also suppressed the malignant phenotype in human breast cancer MDA-MB-231 cells and decreased tumour-induced lymphangiogenesis when used in combination with a conditional medium culture system. Fucoxanthin significantly decreased levels of vascular endothelial growth factor (VEGF)-C, VEGF receptor-3, nuclear factor kappa B, phospho-Akt and phospho-PI3K in HLEC. Fucoxanthin also decreased micro-lymphatic vascular density (micro-LVD) in a MDA-MB-231 nude mouse model of breast cancer. These findings suggest that fucoxanthin inhibits tumour-induced lymphangiogenesis in vitro and in vivo, highlighting its potential use as an antilymphangiogenic agent for antitumour metastatic comprehensive therapy in patients with breast cancer.
Winters, H., et al. (2019). “The Long-term Patency of Lymphaticovenular Anastomosis in Breast Cancer-Related Lymphedema.” Ann Plast Surg 82(2): 196–200.
BACKGROUND AND OBJECTIVES: Lymphedema is a condition that can greatly affect patient's quality of life. Promising results have been described with lymphaticovenular anastomosis (LVA) in the treatment of lymphedema. It is currently unknown at what rate anastomoses remain functional after a longer follow-up. The aim of this study was to determine LVA patency at 1-year follow-up. METHODS: Retrospective chart review was performed on patients who underwent LVA surgery. Patients who had indocyanine green lymphography performed at 12 months' follow-up after LVA were included in this study. Volume measurements were performed prior to surgery and at 6 and 12 months' follow-up. Patients quality of life was measured prior to surgery and at 6 months' follow-up. RESULTS: Twelve patients met inclusion criteria. In total, 15 (56.5%) of 23 LVAs were considered patent. In 8 patients (66.7%), at least 1 patent LVA was visible. The volume difference between the healthy and affected arms decreased 32.3% on average. Quality of life increased with 1.4 points on average. CONCLUSIONS: This study is, to our knowledge, the first to evaluate long-term patency of LVA in upper limb lymphedema. Our study demonstrates that at least 56.5% of the anastomoses created are patent after 1-year follow-up.
Vascular Anomalies
AlZahrani, F., et al. (2019). “Use of AccuVein AV400 for identification of probable RICH.” JAAD Case Rep 5(3): 213–215.
Bittles, M., et al. (2019). “Laser Ablation of Embryonic Veins in Children.” Pediatr Int. [EPub Feb 12]
INTRODUCTION: Klippel-Trenaunay syndrome (KTS) and related overgrowth syndromes are rare conditions that often present to academic pediatric units and multidisciplinary vascular anomaly clinics. These conditions are commonly associated with abnormalities of the superficial and deep venous structures and carry an increased risk of venous thromboembolism. METHODS: A retrospective chart review was completed of all patients treated at Johns Hopkins All Children's Hospital with endovenous laser therapy (EVLT) for management of dilated embryonic veins in the setting of limb overgrowth. RESULTS: Three patients with limb overgrowth underwent EVLT between 2015–2017. All patients demonstrated successful occlusion of the targeted veins on post-procedure imaging. One patient developed a cellulitis successfully treated with oral antibiotics. CONCLUSIONS: EVLT is a well-tolerated and safe procedure for prophylactic closure of abnormal superficial embryonic veins. This study supports the use of this technique in managing increased thromboembolic risk in this unique patient population and recognizes the need for a long-term study to determine its efficacy. This article is protected by copyright. All rights reserved.
Cai, D. R., et al. (2019). “Topical rapamycin in superficial lymphatic malformation: microcystic lymphatic malformation or verrucous venous malformation?” J Am Acad Dermatol. [E-Pub Jan 30]
Campanelli, R., et al. (2019). “Kinetic and Angiogenic Activity of Circulating Endothelial Colony Forming Cells in Patients with Infantile Haemangioma Receiving Propranolol.” Thromb Haemost 119(2): 274–284.
Endothelial progenitor cells (EPCs) have been suggested to contribute to the neovascularization of infantile haemangioma (IH). There is strong evidence of the efficacy of propranolol in the treatment of IH, possibly by inhibiting both vasculogenesis and angiogenesis in the tumour. We evaluate the frequency of circulating endothelial colony forming cells (ECFCs), as the best EPC surrogate, in patients with IH at diagnosis and while receiving propranolol by an ex vivo 12-month longitudinal study. Biological aspects of the ECFCs, such as their in vitro angiogenic potential, membrane CXCR4 expression and Ca(2+) signalling, were investigated. Circulating ECFCs were isolated by in vitro culture and expanded for 2 to 3 passages in 23 patients with IH (median age: 5.5 months, range: 5.5 weeks-11 months) before and 3, 6, 9 and 12 months after receiving propranolol. Twenty-four healthy subjects comparable for age were also assessed (CTRLs). Untreated patients with IH had a circulating ECFC frequency lower (p = 0.001) than CTRLs; nevertheless, in in vitro starving conditions, ECFCs showed enhanced capacity to form tube-like structures than those of CTRLs. Patients with IH following the therapy with propranolol had a significantly increased (p = 0.022) circulating ECFC frequency, that showed a diminished tube-like formation capacity in vitro, and an altered constitutive store-operated Ca(2+) entry. ECFCs play a role in IH pathogenesis; the response to propranolol therapy is associated with their increased frequency in the peripheral blood and a reduction of their vasculogenic activity.
Chen, D. Y. and J. R. Crawford (2018). “Novel KRIT1/CCM1 heterozygous nonsense mutation (c.715 C>T) associated with cerebral and cerebellar cavernous malformations in a paediatric patient.” BMJ Case Rep 2018.
Chen, S., et al. (2019). “Itraconazole induces regression of infantile hemangioma via down-regulation of the PDGF-D/PI3K/Akt/mTOR pathway.” J Invest Dermatol. [E-Pub Jan 29]
Infantile hemangioma (IH) is the most common benign vascular tumor of infancy. We have previously reported that itraconazole, a common anti-fungal agent, can clinically improve or cure IH; however, the underlying molecular mechanisms are still unclear. Here, we show that itraconazole treatment significantly inhibits the proliferation and promotes apoptosis of the endothelial cells of mouse hemangioma (EOMA) cell line and infantile primary hemangioma endothelial cell (HemEC). Itraconazole also remarkably reduced angiogenesis of HemEC in vitro. We further performed transcriptome profiling via mRNA microarrays in HemEC cells upon itraconazole treatment, and identified cytokine-cytokine receptor interaction as the top significantly enriched pathway. Importantly, itraconazole significantly reduced platelet-derived growth factor D (PDGF-D) level, resulting in suppression of PDGFR-beta activation and inhibition of its downstream effectors, such as PI3K, Akt, 4E-BP1 and p70S6K, which are important for cellular growth and survival of IH. In conclusion, our results suggest that PDGF-D is a target of itraconazole in IH.
Cheng, J., et al. (2019). “30-Day outcomes analysis of NSQIP-pediatric for surgical management of head and neck lymphatic malformations in children.” Int J Pediatr Otorhinolaryngol 118: 21–24.
OBJECTIVE: Identify adverse events associated with surgical management of head and neck lymphatic malformations in children by investigating a US national database. DATA SOURCE: Pediatric American College of Surgeons (ACS) National Surgical Quality Improvement Program((R)) (ACS NSQIP((R)) - pediatric), years 2012–2016. METHODS: Subjects included children under 18 years with a postoperative diagnosis of International Classification of Diseases (ICD), 9th revision code: 228.1 - lymphangioma, any site or ICD-10 code D18.1. RESULTS: 163 patients were identified. 67 (41.1%) were female and 96 (58.9%) were male. The median age was 4.2 years (interquartile range [IQR] 1.6–11.3 years). Sixty-five (39.9%) underwent head and neck procedures. 19 (11.7%) patients with 30-day adverse events were identified, with unplanned reoperation being the most common; in the head and neck surgery group, there were 5 (7.7%). There was no significant difference in the occurrence of adverse events between head and neck surgery and the non-head and neck surgery group (p = 0.2238). CONCLUSIONS: No individual patient clinical factors were identified to be associated with increased rates of 30-day adverse event rates for surgical management of lymphatic malformations in children. Our investigation highlights the need for quality improvement to help decrease 30-day adverse events for surgery for this group, as the rate was quite high overall (11.7%). The wound complication rate was very low, but we observed a non-negligible number of reoperations and readmissions. Improving quality of care for surgical management of lymphatic malformations in children should focus future investigations on limiting reoperations and readmissions within the first 30 days postoperatively.
Cheng, J., et al. (2019). “Outcomes of surgical treatment for hemangiomas.” Pediatr Dermatol. [E-Pub Feb 23]
OBJECTIVE: To quantify complications and rates of adverse events associated with surgical excision of hemangiomas in children using a national surgical database. DATA SOURCE: Pediatric American College of Surgeons (ACS) National Surgical Quality Improvement Program((R)) (ACS NSQIP((R)) -pediatric), years 2012–2016. METHODS: Subjects included children under 18 years with a postoperative diagnosis of International Classification of Diseases (ICD), 9th revision code: 228.00 and 228.01, or ICD 10 codes D18.00 and D18.01-hemangioma, any site and hemangioma, of skin and subcutaneous tissue. RESULTS: A total of 1180 patients were included. The median age was 3.2 years (interquartile range [IQR] 1.2 to 6.4 years old). No occurrences of deep incisional surgical site infection, nerve injury, mortality, sepsis, septic shock, or blood stream infections were noted. In multivariate analysis, age </ = 3 years and advanced American Society of Anesthesiologists class were significant predictors of adverse events (P = 0.035 and 0.001, respectively). CONCLUSIONS: For children with infantile hemangioma who fail to respond or have an incomplete response to medical therapy, surgical resection may be a relatively safe treatment alternative. Children older than 3 years of age with hemangiomas had less surgical adverse events than younger children. Overall, however, the surgical complications rates were low and deemed relatively minor.
Colletti, G., et al. (2018). “Vascular malformations of the orbit (lymphatic, venous, arteriovenous): Diagnosis, management and results.” J Craniomaxillofac Surg. [E-Pub Feb 17]
Vascular malformations are often found inside the orbit. Isolated venous malformations (frequently misnamed as cavernous hemangiomas) are the most frequent among these. However, also lymphatic and arteriovenous malformations can affect the orbit. The complex anatomy of the orbit and the fact that its content easily suffers from compartmental syndrome explain why treating orbital vascular malformations can be challenging and technically demanding. In this study, two institutions have retrospectively collected their cases, consisting in a total of 69 vascular malformations of the orbit. Each type of malformation has been evaluated separately in terms of diagnosis, indications for treatment, techniques and outcomes. Moreover, the authors have analyzed in detail venous malformations, identifying three different types, named orbital venous malformation (OVM) 1, 2 and 3. These behave differently from each other, and a prompt differential diagnosis is mandatory to pose correct indications, minimize risks and improve results. Overall, surgery was the technique of choice for OVM1, microcystic lymphatic malformations (LM) and arteriovenous malformations (AVM). A pure transnasal approach with mass removal and reconstruction of the medial wall with polyethylene sheets was chosen for OVM1 (intra- or extraconal) located in the medial or superomedial compartment. Sclerotherapy had a role in treating macrocystic LM and OVM3.
Coughlin, K., et al. (2019). “Methemoglobinemia in an Infant After Sclerotherapy With High-Dose Doxycycline.” Pediatrics. [E-Pub Jan 19]
Methemoglobinemia occurs when the heme moiety of hemoglobin (Hb) is oxidized from the ferrous to ferric state, leading to impairments in oxygen transport and delivery. Methemoglobinemia is rare in pediatric patients but has been described in the setting of congenital abnormalities in the Hb structure, inherited enzyme deficiencies, oxidative Hb injury in response to illness, and oxidative Hb injury due to toxicants. We present a 1-week-old infant born with a cervical lymphangioma who developed persistent desaturations that were unresponsive to oxygen after sclerotherapy with doxycycline. Arterial blood gas revealed a high Pao2 despite low saturations being found on pulse oximetry and a methemoglobin level that was found to be elevated. Further sclerotherapy was discontinued, the saturations eventually normalized, and the methemoglobin level decreased. This is a novel report of sclerotherapy with doxycycline associated with the development of methemoglobinemia.
Crist, A. M., et al. (2019). “Angiopoietin-2 Inhibition Rescues Arteriovenous Malformation in a Smad4 Hereditary Hemorrhagic Telangiectasia Mouse Model.” Circulation. [E-Pub Feb 13]
BACKGROUND: Hereditary Hemorrhagic Telangiectasia (HHT) is an autosomal dominant vascular disorder caused by heterozygous, loss-of-function mutations in four TGFbeta pathway members, including the central transcriptional mediator of the TGFbeta pathway, Smad4. Loss of Smad4 causes the formation of inappropriate, fragile connections between arteries and veins called arteriovenous malformations (AVM), which can hemorrhage leading to stroke, aneurysm or death. Unfortunately, the molecular mechanisms underlying AVM pathogenesis remain poorly understood and the TGFbeta downstream effectors responsible for HHT-associated AVM formation are currently unknown. METHODS: To identify potential biological targets of the TGFbeta pathway involved in AVM formation, we performed RNA- and ChIP-sequencing experiments on BMP9 stimulated endothelial cells (ECs) and isolated ECs from a Smad4 inducible, EC specific knockout (Smad4-iECKO) mouse model that develops retinal AVMs. These sequencing studies identified the Angiopoietin-Tek signaling pathway as a downstream target of SMAD4. We utilized monoclonal blocking antibodies to target a specific component in this pathway and assess its effects on AVM development. RESULTS: Sequencing studies uncovered 212 potential biological targets involved in AVM formation, including the EC surface receptor, TEK (TEK receptor tyrosine kinase) and its antagonistic ligand, ANGPT2 (angiopoietin-2). In Smad4-iECKO mice, Angpt2 expression is robustly increased, while Tek levels are decreased resulting in an overall reduction in Angiopoietin-Tek signaling. We provide evidence that SMAD4 directly represses Angpt2 transcription in ECs. Inhibition of ANGPT2 function in Smad4 deficient mice, either before or after AVMs form, prevents and alleviates AVM formation and normalizes vessel diameters. These rescue effects are attributed to a reversion in EC morphological changes, such as cell size and shape that are altered in the absence of Smad4. CONCLUSIONS: Our studies provide a novel mechanism whereby loss of Smad4 causes increased Angpt2 transcription in ECs leading to AVM formation, increased blood vessel calibers and changes in EC morphology in the retina. Blockade of ANGPT2 function in an in vivo Smad4 model of HHT alleviated these vascular phenotypes further implicating ANGPT2 as an important TGFbeta downstream mediator of AVM formation. Therefore, alternative approaches that target ANGPT2 function may have therapeutic value for the alleviation of HHT symptoms, such as AVMs.
Del Frari, L., et al. (2018). “Propranolol pharmacokinetics in infants treated for Infantile Hemangiomas requiring systemic therapy: Modeling and dosing regimen recommendations.” Pharmacol Res Perspect 6(3): e00399.
Propranolol has become the first choice therapy for complicated Infantile Hemangiomas (IH). The pharmacokinetics of propranolol were evaluated after repeated oral administration of a new pediatric solution of propranolol at 3 mg kg(−1) day(−1) given twice daily (BID) in infants (77–243 days) with IH. A population model was built to describe the pharmacokinetics of propranolol in infants and to simulate different dosing regimens. One hundred and sixty-seven plasma concentrations from 22 infants were used in the population analysis. Weight effect was tested on apparent clearance and volume of distribution. Monte-Carlo simulations were performed for 4 dosing regimens: BID dosing with irregular or strict 12-hour intervals and 2 different 3 time daily dosing (TID) regimens. The best model was a one-compartment model with first-order absorption and elimination rates. The weight affected the clearance but not the volume. Typical oral clearance was estimated at 3.06 L hour(−1) kg(−1) (95% CI: 1.14–8.61 L hour(−1) kg(−1)), close to adult clearance data. When regular BID dosing was compared to TID or irregular BID regimens, simulated median Cmin and Cmax were <20% different. To conclude, a model using a weight allometric function on clearance was established and confirmed that the dose in mg/kg should be used without adaptation by range of age in treatment of complicated IH. The simulations support the use of a BID dosing preferably to a TID dosing thanks to close Cmin and Cmax at steady state between both regimen and showed the possibility of irregular BID dosing, allowing early administration in the evening when needed.
Gordo, G., et al. (2019). “Constitutional mosaicism in RASA1-related capillary malformation-arteriovenous malformation.” Clin Genet. [E-Pub Jan 13]
Capillary malformation-arteriovenous malformation (CM-AVM) is caused by germline RASA1 and EPHB4 alterations. RASA1 intralesional second hits have also been reported. Here we report RASA1 constitutional mosaicism, defined here as the presence of a mosaic variant in all cell types of an individual, in two patients with CM-AVM. High-throughput sequencing was used to search for RASA1 pathogenic variants in blood samples from two unrelated patients with CM-AVM. An affected tissue sample from one of the patients was also analyzed. Both patients showed different nonsense RASA1 variants in mosaic, ranging from 7% to 21.5%, in blood samples and in the corresponding affected tissue sample from one of the patients. In conclusion, we report for the first time the presence of RASA1 constitutional mosaicism in CM-AVM. Constitutional mosaicism has implications for accurate molecular diagnosis and recurrence risk and helps to explain the great phenotypic variability in CM-AVM.
Hao, Q., et al. (2018). “Activin Receptor-Like Kinase 1 Combined With VEGF-A Affects Migration and Proliferation of Endothelial Cells From Sporadic Human Cerebral AVMs.” Front Cell Neurosci 12: 525.
Heterozygous loss of activin receptor-like kinase 1 (Alk1) can lead to hereditary hemorrhagic telangiectasia (HHT), which is a kind of vascular disease characterized by direct connections between arteries and veins with the lacking of capillaries, and develops into arteriovenous malformations (AVMs) in later stage. However, the changes of Alk1 in human sporadic cerebral AVMs (cAVMs) remain unknown. In the present study, we used endothelial cells (ECs) derived from human cAVMs (cAVM-ECs) specimens, to explore the characteristics of cAVM-ECs and the relationship between Alk1 and human sporadic cAVMs. Our data showed that there were obvious morphological changes in cAVM-ECs, and they could trans-differentiate into mesenchyme-like cells easily in a short period. In addition, the abilities of migration of cAVM-ECs were poorer than that in human aortic endothelial cells (HA-ECs). The abilities of proliferation of cAVM-ECs in patients with different ages were lower than HA-ECs. Immunofluorescent staining and Western blot showed that the levels of Alk1 mRNA and protein in the HA-ECs were both higher than that in cAVM-ECs. In addition, the levels of Alk1 mRNA had no significant differences between different ages in cAVM-ECs groups. The levels of VEGF-A mRNA in the cAVM were higher than HA-ECs. Besides, levels of VEGF-A mRNA expression were lower in older cAVM patients. Therefore, we conclude that Alk1 might induce the formation of sporadic human cAVMs through affecting migration and proliferation of endothelial cells combined with VEGF-A.
Kato, H., et al. (2018). “Chest imaging in generalized lymphatic anomaly and kaposiform lymphangiomatosis.” Pediatr Int 60(7): 667–668.
Kato, M., et al. (2019). “Flow Pattern Classification in Lymphatic Malformations by Indocyanine Green Lymphography.” Plast Reconstr Surg 143(3): 558e–564e.
BACKGROUND: Lymphatic malformation is a congenital lymphatic disorder. Although a few lymphangiographic and lymphoscintigraphic studies of lymphatic malformation exist, its lymphatic flow has not been fully assessed, and a classification system has not yet been established. However, indocyanine green lymphography has been developed to safely provide a fine assessment of lymph flow in the treatment of lymphedema. In addition, indocyanine green lymphography has been shown to be helpful in detecting the lymphatic malformation inflow for the treatment of refractory microcystic type lymphatic malformation using the venous anastomosis technique. Therefore, the authors aimed to reveal the in vivo lymph flow around the lymphatic malformation using indocyanine green lymphography, and to design a classification system according to the observed patterns. METHODS: Indocyanine green lymphography was performed in 20 sequential pediatric patients with lymphatic malformation (aged 11 months to 10 years). Most of the cases were intractable, with microcystic or mixed-type lymphatic malformation. RESULTS: All patients successfully completed lymphography with clear observations. The flow patterns were classified into four types: type 1 had a strong detectable inflow; type 2 had multiple small observable inflows; type 3 had a superficial lymph flow over the lesion; and type 4 had a flow around the lymphatic malformation, without any connections to the lesion. CONCLUSION: The proposed classification system may aid in the further development of surgical treatments for lymphatic malformation.
Keppler-Noreuil, K. M., et al. (2019). “Pharmacodynamic Study of Miransertib in Individuals with Proteus Syndrome.” Am J Hum Genet. [E-Pub Feb 26]
Proteus syndrome is a life-threatening segmental overgrowth syndrome caused by a mosaic gain-of-function AKT1 variant. There are no effective treatments for Proteus syndrome. Miransertib is an AKT1 inhibitor that, prior to this study, has been evaluated only in adult oncology trials. We designed a non-randomized, phase 0/1 pilot study of miransertib in adults and children with Proteus syndrome to identify an appropriate dosage starting point for a future efficacy trial using a pharmacodynamic endpoint. The primary endpoint was a 50% reduction in the tissue levels of AKT phosphorylation from biopsies in affected individuals. We also evaluated secondary efficacy endpoints. We found that a dose of 5 mg/m(2)/day (1/7 the typical dose used in oncology) led to a 50% reduction in phosphorylated AKT (pAKT) in affected tissues from five of six individuals. This dose was well tolerated. Two of the six efficacy endpoints (secondary objectives) suggested that this agent may be efficacious. We observed a decrease in a cerebriform connective tissue nevus and a reduction in pain in children. We conclude that 5 mg/m(2)/day of miransertib is an appropriate starting point for future efficacy trials and that this agent shows promise of therapeutic efficacy in children with Proteus syndrome.
Klostranec, J. M., et al. (2019). “A theory for polymicrogyria and brain arteriovenous malformations in HHT.” Neurology 92(1): 34–42.
Hereditary hemorrhagic telangiectasia (HHT) is generally considered a disorder of endothelial dysfunction, characterized by the development of multiple systemic arteriovenous malformations (AVMs), including within the brain. However, there have recently been a number of reports correlating HHT with malformations of cortical development, of which polymicrogyria is the most common type. Here we present 7 new cases demonstrating polymicrogyria in HHT, 6 of which demonstrate a brain AVM (bAVM) in close spatial proximity, with the aim of providing a common origin for the association. Upon reviewing patient genetics and imaging data and comparing with previously reported findings, we form 2 new conclusions: (1) polymicrogyria in HHT appears exclusively associated with a subset of mutations in the transmembrane protein endoglin that is involved with blood flow-related mechanotransduction signaling during angiogenesis and (2) the polymicrogyria is characteristically unilateral, typically focal, and correlates with vascular regions experiencing low fluid shear stress during corticogenesis in utero. Integrating these with findings in the literature from genetics and molecular biology experiments, we propose a theory suggesting haploinsufficient endoglin mutations, especially those that are dominant-negative, may predispose focal, aberrant hypersprouting angiogenesis during corticogenesis that leads to the production of polymicrogyria. This hypoxic insult may further serve as the revealing trigger for later development of a spatially coincident bAVM. This hypothesis suggests an essential role for endoglin-mediated hemodynamic mechanotransduction in normal corticogenesis.
Krowchuk, D. P., et al. (2019). “Clinical Practice Guideline for the Management of Infantile Hemangiomas.” Pediatrics 143(1).
Infantile hemangiomas (IHs) occur in as many as 5% of infants, making them the most common benign tumor of infancy. Most IHs are small, innocuous, self-resolving, and require no treatment. However, because of their size or location, a significant minority of IHs are potentially problematic. These include IHs that may cause permanent scarring and disfigurement (eg, facial IHs), hepatic or airway IHs, and IHs with the potential for functional impairment (eg, periorbital IHs), ulceration (that may cause pain or scarring), and associated underlying abnormalities (eg, intracranial and aortic arch vascular abnormalities accompanying a large facial IH). This clinical practice guideline for the management of IHs emphasizes several key concepts. It defines those IHs that are potentially higher risk and should prompt concern, and emphasizes increased vigilance, consideration of active treatment and, when appropriate, specialty consultation. It discusses the specific growth characteristics of IHs, that is, that the most rapid and significant growth occurs between 1 and 3 months of age and that growth is completed by 5 months of age in most cases. Because many IHs leave behind permanent skin changes, there is a window of opportunity to treat higher-risk IHs and optimize outcomes. Early intervention and/or referral (ideally by 1 month of age) is recommended for infants who have potentially problematic IHs. When systemic treatment is indicated, propranolol is the drug of choice at a dose of 2 to 3 mg/kg per day. Treatment typically is continued for at least 6 months and often is maintained until 12 months of age (occasionally longer). Topical timolol may be used to treat select small, thin, superficial IHs. Surgery and/or laser treatment are most useful for the treatment of residual skin changes after involution and, less commonly, may be considered earlier to treat some IHs.
Lalonde, E., et al. (2019). “Molecular diagnosis of somatic overgrowth conditions: A single-center experience.” Mol Genet Genomic Med. [E-Pub Feb 15]
BACKGROUND: Somatic overgrowth conditions, including Proteus syndrome, Sturge-Weber syndrome, and PIK3CA-related overgrowth spectrum, are caused by post-zygotic pathogenic variants, result in segmental mosaicism, and give rise to neural, cutaneous and/or lipomatous overgrowth. These variants occur in growth-promoting pathways leading to cellular proliferation and expansion of tissues that arise from the affected cellular lineage. METHODS: We report on 80 serial patients evaluated for somatic overgrowth conditions in a diagnostic laboratory setting, including three prenatal patients. In total, 166 tissues from these 80 patients were subjected to targeted sequencing of an 8-gene panel capturing 10.2 kb of sequence containing known pathogenic variants associated with somatic overgrowth conditions. Deep next-generation sequencing was performed with the IonTorrent PGM platform at an average depth typically >5,000x. RESULTS: Likely pathogenic or pathogenic variants were identified in 36 individuals and variants of unknown significance in four. The overall molecular diagnostic yield was 45% but was highly influenced by both submitted tissue type and phenotype. In the prenatal setting, two patients had pathogenic variants identified in cultured amniocytes but in a third patient, the pathogenic variant was only present in post-natal tissues. Finally, expanding the test to include full gene sequencing of PIK3CA in contrast to targeted sequencing identified likely pathogenic variants in 3 of 7 patients that tested negative on the original panel. CONCLUSION: Next-generation sequencing has enabled sensitive detection of somatic pathogenic variants associated with overgrowth conditions. However, as the pathogenic variant allele frequency varies by tissue type within an individual, submission of affected tissue(s) greatly increases the chances of a molecular diagnosis.
Lavaud, J., et al. (2019). “Photoacoustic imaging as an innovative technique for the exploration of Blue Rubber Bleb Nevus.” Br J Dermatol. [E-Pub Feb 12]
Blue rubber bleb nevus syndrome (BRBN, Bean syndrome) is a rare vascular malformation (VM) characterized by multiple cutaneous and mucous venous defects disseminated throughout the body. An infringement of mucous membranes is possible with potential complications as anemia or hemorrhage. Photoacoustic imaging (PAI) is an emerging technology combining the most compelling features of optical imaging and ultrasound, providing both high optical contrast and high ultrasound resolution at depth in living organisms. This article is protected by copyright. All rights reserved.
Lei, H. Z., et al. (2018). “Retrospective study on the outcomes of infantile tufted angioma complicated by Kasabach-Merritt Phenomenon.” Clin Chim Acta 486: 199–204.
OBJECTIVE: To analyze the clinical characteristics and treatment of pediatric tufted angiomas(TA)complicated by Kasabach-Merritt Phenomenon (KMP). METHOD: A retrospective analysis was conducted on the clinical data and follow-up data of 13 patients diagnosed with TA complicated by KMP. Five male and 8 female patients with an average age of 5.7months (range, 29days to 1year) were treated with surgery between January 2009 and June 2012. According to the size and location of lesions and the degree of thrombocytopenia, complete or subtotal resection was performed. The median follow-up period was 3.4years (range, 1.7years to 5.2years). Therapeutic outcomes were evaluated by platelet count and lesion size. RESULTS: Curative treatment of KMP is defined as restoration of normal hemostasis and elimination of tumor cells. Twelve patients achieved curative treatment and one died of multiple organ failure after operation. Ten patients received complete resection and three patients received incomplete resection. Thrombocyte count, hemoglobin and blood coagulation were respectively restored to normal levels within 1–3days and 1–2weeks post complete resection operation. One of the three patients who received subtotal resection operation died. In the other two patients, the platelet count fluctuated over time but remained above 60 × 10(9) /L, a significantly higher level than the preoperational level. Residual lesions slowly disappeared after continuous medication 3–6months post operation. CONCLUSION: Early surgical treatment of patients with TA complicated with KMP resulted in significantly higher curative rate and reduced side-effects of drugs.
Li, L., et al. (2019). “No Increased Risks Associated with Propranolol Treatment for Infantile Hemangioma in Preterm Infants were Identified at 3 Years of Age.” Am J Clin Dermatol. [E-Pub Jan 9]
BACKGROUND: Concerns have been raised that propranolol treatment of infantile hemangioma (IH) may be associated with increased risks of adverse effects and growth impairment in preterm infants due to their immature development. OBJECTIVE: This study aimed to find out whether treatment of IH with propranolol in preterm infants is associated with higher incidences of long-term adverse effects and growth impairment in comparison with term infants. METHODS: The clinical data of 55 preterm infants and 180 term infants with IH treated with oral propranolol for 6 months were retrospectively collected and analyzed. RESULTS: The preterm and term patients did not differ significantly in terms of the general characteristics and adverse effect incidence (all p > 0.05). Height, weight, and head circumference of the preterm infants at ages 1, 2, and 3 years did not differ significantly from the normal references (all p > 0.05). In the term patients, only 1-year-old female weight and head circumference were significantly higher than the normal references (both p < 0.05). CONCLUSION: Treatment of IH with propranolol for 6 months did not increase the risks for adverse effects or growth impairment up to age 3 years in preterm versus term patients in our study.
Li, X., et al. (2019). “Ponatinib Combined With Rapamycin Causes Regression of Murine Venous Malformation.” Arterioscler Thromb Vasc Biol 39(3): 496–512.
Objective- Venous malformations (VMs) arise from developmental defects of the vasculature and are characterized by massively enlarged and tortuous venous channels. VMs grow commensurately leading to deformity, obstruction of vital structures, bleeding, and pain. Most VMs are associated with the activating mutation L914F in the endothelial cell (EC) tyrosine kinase receptor TIE2. Therapeutic options for VM are limited and ineffective while therapy with the mammalian target of rapamycin inhibitor rapamycin shows moderate efficacy. Here, we investigated novel therapeutic targets promoting VM regression. Approach and Results- We performed an unbiased screen of Food and Drug Administration-approved drugs in human umbilical vein ECs expressing the TIE2-L914F mutation (HUVEC-TIE2-L914F). Three ABL (Abelson) kinase inhibitors prevented cell proliferation of HUVEC-TIE2-L914F. Moreover, c-ABL, common target of these inhibitors, was highly phosphorylated in HUVEC-TIE2-L914F and VM patient-derived ECs with activating TIE2 mutations. Knockdown of c-ABL/ARG in HUVEC-TIE2-L914F reduced cell proliferation and vascularity of murine VM. Combination treatment with the ABL kinase inhibitor ponatinib and rapamycin caused VM regression in a xenograft model based on injection of HUVEC-TIE2-L914F. A reduced dose of this drug combination was effective in this VM murine model with minimal side effects. The drug combination was antiproliferative, enhanced cell apoptosis and vascular channel regression both in vivo and in a 3-dimensional fibrin gel assay. Conclusions- This is the first report of a combination therapy with ponatinib and rapamycin promoting regression of VM. Mechanistically, the drug combination enhanced AKT inhibition compared with single drug treatment and reduced PLCgamma (phospholipase C) and ERK (extracellular signal-regulated kinase) activity.
Liu, C., et al. (2019). “MiR-187-3p Enhances Propranolol Sensitivity of Hemangioma Stem Cells.” Cell Struct Funct. [E-Pub Feb 5]
Infantile hemangioma is the most common soft tissue tumors in childhood. In clinic, propranolol is widely used for infantile hemangioma therapy. However, some of the infantile hemangioma patients display resistance to propranolol treatment. Previous studies show that miR-187-3p is inhibited in hepatocellular carcinoma and lung cancer, while the role of miR-187-3p in infantile hemangioma remains unclear. In the present study, we explore the biological role of miR-187-3p in infantile hemangioma. The mRNA and protein levels of related genes were detected by real-time PCR and Western blotting. CCK8 assay was used to detect cell viability and IC50 values of propranolol. Cell apoptosis was detected by Caspase-3 Activity assay. Luciferase reporter assay and biotin RNA pull down assay were used to detect the interaction between miR-187-3p and the targeted gene. MiR-187-3p was down-regulated in infantile hemangioma tissues and promoted propranolol sensitivity of HemSCs. Mechanically, NIPBL was the direct target of miR-187-3p in HemSCs. NIPBL downregulation inhibited propranolol resistance of HemSCs. Re-introduction of NIPBL reversed miR-187-3p-meidated higher propranolol sensitivity of HemSCs. MiR-187-3p enhanced propranolol sensitivity of hemangioma stem cells via targeting NIPBL. MiR-187-3p may serve as a novel prognostic indicator and potential target for infantile hemangioma therapy. Key words: MiR-187-3p, infantile hemangioma, propranolol, resistance, NIPBL.
Nicholson, P., et al. (2019). “The protean manifestations of RASA1 gene mutation.” Clin Exp Dermatol. [E-Pub Jan 8]
Park, S., et al. (2019). “A Child With Lymphangioma Due to Somatic Mutation in PIK3CA Successfully Treated With Everolimus.” Pediatr Neurol 91: 65–67.
Ricci, K. W., et al. (2019). “Efficacy of systemic sirolimus in the treatment of generalized lymphatic anomaly and Gorham-Stout disease.” Pediatr Blood Cancer: e27614.
BACKGROUND: Generalized lymphatic anomaly (GLA) and Gorham-Stout disease (GSD) are rare complicated lymphatic malformations that occur in multiple body sites and are associated with significant morbidity and mortality. Treatment options have been limited, and conventional medical therapies have been generally ineffective. Emerging data suggest a role for sirolimus as a treatment option for complex lymphatic anomalies. PROCEDURE: Disease response was evaluated by radiologic imaging, quality of life (QOL), and clinical status assessments in children and young adults with GLA and GSD from a multicenter systematic retrospective review of patients treated with oral sirolimus and the prospective phase 2 clinical trial assessing the efficacy and safety of sirolimus in complicated vascular anomalies (NCT00975819). Sirolimus dosing regimens and toxicities were also assessed. RESULTS: Eighteen children and young adults with GLA (n = 13) or GSD (n = 5) received oral sirolimus. Fifteen patients (83%) had improvement in one or more aspects of their disease (QOL 78%, clinical status 72%, imaging 28%). No patients with bone involvement had progression of bone disease, and the majority had symptom or functional improvement on sirolimus. Improvement of pleural and pericardial effusion(s) occurred in 72% and 50% of affected patients; no effusions worsened on treatment. CONCLUSIONS: Sirolimus appears effective at stabilizing or reducing signs/symptoms of disease in patients with GLA and GSD. Functional impairment and/or QOL improved in the majority of individuals with GLA and GSD with sirolimus treatment.
Rodriguez-Laguna, L., et al. (2019). “Somatic activating mutations in PIK3CA cause generalized lymphatic anomaly.” J Exp Med 216(2): 407–418.
Generalized lymphatic anomaly (GLA) is a vascular disorder characterized by diffuse or multifocal lymphatic malformations (LMs). The etiology of GLA is poorly understood. We identified four distinct somatic PIK3CA variants (Glu542Lys, Gln546Lys, His1047Arg, and His1047Leu) in tissue samples from five out of nine patients with GLA. These same PIK3CA variants occur in PIK3CA-related overgrowth spectrum and cause hyperactivation of the PI3K-AKT-mTOR pathway. We found that the mTOR inhibitor, rapamycin, prevented lymphatic hyperplasia and dysfunction in mice that expressed an active form of PIK3CA (His1047Arg) in their lymphatics. We also found that rapamycin reduced pain in patients with GLA. In conclusion, we report that somatic activating PIK3CA mutations can cause GLA, and we provide preclinical and clinical evidence to support the use of rapamycin for the treatment of this disabling and deadly disease.
Shahbahrami, K., et al. (2019). “Chronic lower extremity wounds in a patient with Klippel Trenaunay syndrome.” J Vasc Surg Cases Innov Tech 5(1): 45–48.
Klippel-Trenaunay syndrome is a rare disorder consisting of the triad of vascular and/or lymphatic malformations, capillary malformations, and soft tissue or bony hypertrophy. Symptom control is the mainstay of treatment for these patients, with many of the symptoms never fully being relieved. In this case report, we present the case of a 46-year-old man with chronic lower extremity ulcerations unresponsive to wound care therapy. Owing to the chronic nature of his wounds and associated pain, reconstruction of his iliac vein was performed using polytetrafluoroethylene graft and an arteriovenous fistula.
Speir, E. J., et al. (2019). “Volumetric Assessment of Pediatric Vascular Malformations Using a Rapid, Hand-Held Three-Dimensional Imaging System.” J Digit Imaging. [E-Pub Feb 15]
The effect of percutaneous, surgical, and medical therapies for vascular malformations (VMs) is often difficult to quantify volumetrically using cross-sectional imaging. Volumetric measurement is often estimated with serial, expensive MRI examinations which may require sedation or anesthesia. We aim to explore whether a portable 3D scanning device is capable of rapid, accurate volumetric analysis of pediatric VMs. Using an iPad-mounted infrared scanning device, 3D scans of patient faces, arms, and legs were acquired over an 8-month study period. Proprietary software was use to perform subsequent volumetric analysis. Of a total of 30 unilateral VMs involving either the face, arms, or legs, 26 (86.7%) VMs were correctly localized by discerning the larger volume of the affected side compared to the normal contralateral side. For patients with unilateral facial VMs (n = 10), volume discrepancy between normal and affected sides differed compared with normal controls (n = 19). This was true for both absolute (60 cc +/− 55 vs 15 cc +/− 8, p = 0.03) as well as relative (18.1% +/− 13.2 vs 4.0% +/− 2.1, p = 0.008) volume discrepancy. Following treatment, two patients experienced change in leg volume discrepancy ranging from - 17.3 to - 0.4%. Using a portable 3D scanning device, we were able to rapidly and noninvasively detect and quantify volume discrepancy resulting from VMs of the face, arms, and legs. Preliminary data suggests this technology can detect volume reduction of VMs in response to therapy.
Straughan, A. J., et al. (2019). “Cost Analysis of a Multidisciplinary Vascular Anomaly Clinic.” Ann Otol Rhinol Laryngol: 3489419826135.
OBJECTIVE:: Multidisciplinary vascular anomaly clinics (VACs) offer important value to pediatric patients with complex vascular anomalies whose care overlaps specialties. These clinics are labor intensive and costly to operate since providers see fewer patients compared to their individual specialty clinic. Our North American tertiary care institution's VAC specialists include a pediatric otolaryngologist, pediatric surgeon, pediatric plastic surgeon, pediatric dermatologist, and interventional radiologist. To assess financial feasibility, we conducted a cost analysis of our VACs comprised of 2 half-day multidisciplinary physician attended clinics (5 specialists at our main campus and 2 specialists at a satellite clinic) and a half-day nurse practitioner clinic. METHOD:: Assessment of net revenue based on net collections for clinic, professional, operative, hospital setting, and facility charges generated during 12 consecutive monthly VACs beginning July 1, 2015. Expense calculations included provider and staff salaries, benefits, supply costs, and clinic leasing costs. RESULTS:: There were 469 clinic visits, of which 202 were new patient evaluations. Sixty-eight patients underwent 93 procedures under general anesthesia, including procedures performed by our interventional radiologist, most commonly sclerotherapy or embolization (n = 37), surgical interventions including endoscopy (n = 36), or laser procedures (n = 20). Three patients were admitted. Fifty-seven patients received a new diagnosis different from that for which they were referred. Gross revenue was $1 810 525, and net revenue was 42.5%, or $783 152. Expenses totaled $453 415 for a net positive revenue of $329 737. CONCLUSION:: When including direct downstream revenue, particularly from operative procedures, our VAC program operates on a net positive margin, making the program financially feasible.
Ten Broek, R. W., et al. (2019). “Comprehensive molecular and clinicopathological analysis of vascular malformations: A study of 319 cases.” Genes Chromosomes Cancer. [E-Pub Jan 25]
Vascular malformations are part of overgrowth syndromes characterized by somatic mosaic mutations or rarely by germline mutations. Due to their similarities and diversity, clinicopathological classification can be challenging. A comprehensive targeted Next Generation Sequencing screen using Unique Molecular Identifiers with a technical sensitivity of 1% mutant alleles was performed for frequently mutated positions in >/ = 21 genes on 319 formalin-fixed paraffin-embedded samples. In 132 out of 319 cases pathogenic mosaic mutations were detected affecting genes previously linked to vascular malformations e.g., PIK3CA (n = 80), TEK (TIE2) (n = 11), AKT1 (n = 1), GNAQ (n = 7), GNA11 (n = 4), IDH1 (n = 3), KRAS (n = 9), and NRAS (n = 1). Six cases harbored a combination of mutations in PIK3CA and in GNA11 (n = 2), GNAQ (n = 2), or IDH1 (n = 2). Aberrations in PTEN and RASA1 with a variant allele frequency approaching 50% suggestive of germline origin were identified in six out of 102 cases tested; four contained a potential second hit at a lower allele frequency. Ninety-one of the total 142 pathogenic mutations were present at a variant allele frequency <10% illustrating the importance of sensitive molecular analysis. Clinicopathological characteristics showed a broad spectrum and overlap when correlated with molecular data. Sensitive screening of recurrently mutated genes in vascular malformations may help to confirm the diagnosis and reveals potential therapeutic options with a significant contribution of PIK3CA/mTOR and RAS-MAPK pathway mutations. The co-existence of two activating pathogenic mutations in parallel pathways illustrates potential treatment challenges and underlines the importance of multigene testing. Detected germline mutations have major clinical impact.
Thai, T., et al. (2019). “Central Nervous System Effects of Oral Propranolol for Infantile Hemangioma: A Systematic Review and Meta-Analysis.” J Clin Med 8(2).
Concerns about the effects of propranolol on the central nervous system (CNS) in the infantile hemangioma (IH) population have been raised. We conducted a meta-analysis of the CNS and sleep-related effects of oral propranolol in IH patients. PubMed, Embase, Cochrance, Web of Science, and ClinicalTrials.gov were searched for relevant studies. We included clinical trials that compared oral propranolol with other treatments among IH patients under 6 years old and monitored and reported any adverse events. Study characteristics, types and number of adverse events were abstracted. Cochrane Collaboration Risk of Bias Tool was used to assess risk of bias. Our main outcomes were CNS and sleep-related effects. Random-effects models were used to estimate the pooled risk ratio. We did not observe statistically significant associations between oral propranolol and CNS or sleep-related effects. Oral propranolol appeared to have a safer profile of CNS effects than corticosteroids (RR = 0.27, 95% CI 0.02(-)3.00), but had an increased risk versus non-corticosteroids (for CNS effect, RR = 1.40, 95% CI 0.86(-)2.27; for sleep-related effects, RR = 1.63, 95% CI 0.88(-)3.03). Despite no statistically significant associations, there were suggestive findings of increased CNS effects and sleep-related risk of propranolol versus non-corticosteroids. In practice, CNS and sleep-related events should be monitored more closely among IH patients treated with oral propranolol.
Ueno, S., et al. (2019). “Indications for tracheostomy in children with head and neck lymphatic malformation: analysis of a nationwide survey in Japan.” Surg Today. [E-Pub Feb 20]
PURPOSE: Airway obstruction caused by lymphatic malformation (LM) in the head and neck may require a tracheostomy. We present the results of our analysis of a nationwide survey on the indications for tracheostomy in children with head and neck LM. METHODS: We analyzed data in relation to tracheostomy based on a questionnaire about 518 children with head and neck LM without mediastinal involvement. RESULTS: Tracheostomy was performed for 43 of the 518 children. Most (32/43) of these children were younger than 1 year of age and the tracheostomy was almost always performed for airway obstruction (40/43). The lesion was in contact with the airway in 32 (72%) of these children, but in only 58 (12%) of the 473 children who were managed without tracheostomy. When the maximum circumferential area of contact was compared, only 20 (27%) of 74 patients with maximum contact of less than a half-circle required tracheostomy, whereas 11 of 13 with maximum contact of more than a half-circle required tracheostomy (P = 0.0001). Six patients without airway contact required tracheostomy because of acute swelling caused by hemorrhage, infection, or both. CONCLUSIONS: Children with head and neck LM required tracheostomy to relieve airway obstruction. Tracheostomy should be considered if the lesion is in contact with the airway and surrounds more than a half-circle, and when it causes acute swelling.
Ventejou, S., et al. (2019). “Hormonal receptors in cutaneous vascular malformations: 51 cases.” Virchows Arch. [E-Pub Feb 28]
Vascular malformations (VMs) are rare congenital anomalies that develop during embryogenesis in different types of vessels. Several triggering factors of cutaneous VMs include trauma, infections, or hormonal changes. We investigated the expression of hormonal receptors (androgen, estrogen, progesterone) in tissue samples of well-characterized VMs. A secondary objective was to identify self-reported triggering factors for these VMs, including hormonal changes, in the cohort of patients. We included patients with VM samples obtained in the tertiary center for vascular anomalies of the University Hospital Center of Tours, France, from January 1, 2007, to August 1, 2018. Immunohistochemistry was used to detect the expression of hormonal receptors (estrogen, progesterone, androgens). We obtained 51 samples from 51 patients: 13 cystic lymphatic malformations (CLMs), 16 venous malformations (VeMs), 11 arteriovenous malformations (AVMs), 4 combined VMs, 4 PIK3CA-related overgrowth spectrum, 1 Parkes-Weber syndrome, 1 Gorham syndrome, and 1 multiple lymphangioendotheliomatosis with thrombopenia. In total, 38 (74.5%) samples were positive for androgen receptor: 11 (84.6%) CLMs, 12 (75.0%) VeMs, 8 (72.2%) AVMs, and 7/11 (63.5%) other samples. All samples were negative for estrogen and progesterone receptors. Triggering factors were self-reported in 7 cases and were most frequently hormonal changes (n = 6, 18.2%). Hormonal triggers were frequent in AVMs (n = 4). Among patients with identified hormonal triggers, VM samples were positive for androgen receptor in 3 and negative in 3. Three-quarters of our VM samples expressed androgen receptor, and most CLM, VeM, and AVM samples were positive. Hormonal triggers were identified in 6/33 patients, mostly with AVMs.
Wang, F., et al. (2019). “Insulinlike growth factor I promotes adipogenesis in hemangioma stem cells from infantile hemangiomas.” Mol Med Rep. [E-Pub Feb 6]
Infantile hemangiomas (IH) are the most common infantile neoplasms and are characterized by initial proliferation during infancy and subsequent spontaneous regression within the next 510 years, frequently leaving fibrous fat residues. However, the specific mechanisms underlying the differentiation of hemangioma stem cells (HemSCs) into adipocytes are not clear. The purpose of the present study was to investigate the effect of insulinlike growth factor I (IGF1) on HemSCs from patients with IH and to determine the signaling mechanisms involved. Treatment of HemSCs with IGF1 led to upregulation of the protein expression levels of peroxisome proliferatoractivated receptorgamma (PPARgamma). By contrast, inhibition of the IGF1 receptor (IGF1R) or phosphoinositide 3kinase (PI3K) activity decreased the expression of PPARgamma, in addition to that of CCAAT/enhancerbinding protein (C/EBP)alpha, C/EBPbeta, and adiponectin. IGF1 upregulated the expression of phosphorylated RACalpha serine/threonineprotein kinase in IH cells, whereas a specific PI3K inhibitor or IGF1R antibody blocked this effect. These results indicated that IGF1 is a proproliferative and prolipogenic factor in IH HemSCs. Taken together, these findings indicated that IGF1 is able to upregulate PPARgamma by activating the IGF1R and PI3K pathways, thereby accelerating lipogenesis and enhancing IH HemSC adipogenesis.
Welfringer-Morin, A., et al. (2019). “Late ulceration of residual abortive infantile hemangioma: a rare complication.” Br J Dermatol. [E-Pub Feb 6]
Abortive and minimal growth infantile hemangiomas (IH) are present at birth and have a proliferative component of less than 25% of their total surface. Clinically, they appear most frequently as a telangiectatic patch with venules, surrounded by a halo of vasoconstriction. They may be large or small, segmental or focal. On immunohistochemistry, these lesions are Glut-1 positive.(2) Ulcerations are the most frequent complication and occur mostly during the proliferative phase.(3–5) To our knowledge, ulcerations on IH sequelae are not reported. This article is protected by copyright. All rights reserved.
Winkler, M., et al. (2019). “Microvascular volume visualization utilizing computed tomographic angiography data facilitates resection of a complicated massive congenital hemangioma.” Clin Imaging 55: 8–11.
CT angiography (CTA) can be used for planning procedural and operative therapies for neonatal vascular lesions, such as congenital hemangiomas (CH), that are too morbid for medical therapy. Neonatal anatomy can be displayed within a small enough field-of-view that the nominal resolution of a modern CT scanner can be realized with a standard 512 × 512 storage matrix, yielding isometric ultrahigh resolution data and allowing for microvascular volume visualization. This case report details the creation and use of microvascular volume visualizations of CTA data during pre-procedural planning for treatment of this pathological entity.
Wooderchak-Donahue, W. L., et al. (2019). “Phenotype of CM-AVM2 caused by variants in EPHB4: how much overlap with hereditary hemorrhagic telangiectasia (HHT)?” Genet Med. [E-Pub Feb 15]
PURPOSE: EPHB4 variants were recently reported to cause capillary malformation-arteriovenous malformation 2 (CM-AVM2). CM-AVM2 mimics RASA1-related CM-AVM1 and hereditary hemorrhagic telangiectasia (HHT), as clinical features include capillary malformations (CMs), telangiectasia, and arteriovenous malformations (AVMs). Epistaxis, another clinical feature that overlaps with HHT, was reported in several cases. Based on the clinical overlap of CM-AVM2 and HHT, we hypothesized that patients considered clinically suspicious for HHT with no variant detected in an HHT gene (ENG, ACVRL1, or SMAD4) may have an EPHB4 variant. METHODS: Exome sequencing or a next-generation sequencing panel including EPHB4 was performed on individuals with previously negative molecular genetic testing for the HHT genes and/or RASA1. RESULTS: An EPHB4 variant was identified in ten unrelated cases. Seven cases had a pathogenic EPHB4 variant, including one with mosaicism. Three cases had an EPHB4 variant of uncertain significance. The majority had epistaxis (6/10 cases) and telangiectasia (8/10 cases), as well as CMs. Two of ten cases had a central nervous system AVM. CONCLUSIONS: Our results emphasize the importance of considering CM-AVM2 as part of the clinical differential for HHT and other vascular malformation syndromes. Yet, these cases highlight significant differences in the cutaneous presentations of CM-AVM2 versus HHT.
Zeng, X., et al. (2019). “EphrinB2-EphB4-RASA1 Signaling in Human Cerebrovascular Development and Disease.” Trends Mol Med. [E-Pub Mar 2]
Recent whole exome sequencing studies in humans have provided novel insight into the importance of the ephrinB2-EphB4-RASA1 signaling axis in cerebrovascular development, corroborating and extending previous work in model systems. Here, we aim to review the human cerebrovascular phenotypes associated with ephrinB2-EphB4-RASA1 mutations, including those recently discovered in Vein of Galen malformation: the most common and severe brain arteriovenous malformation in neonates. We will also discuss emerging paradigms of the molecular and cellular pathophysiology of disease-causing ephrinB2-EphB4-RASA1 mutations, including the potential role of somatic mosaicism. These observations have potential diagnostic and therapeutic implications for patients with rare congenital cerebrovascular diseases and their families.