
Abstract
Background:
In the current study, we reported our experience on sentinel node mapping of breast cancer patients during the extreme shortage of Mo99-Tc99m generators using Tc-99m phytate.
Methods and Results:
During the period from March 7, 2019, to April 18, 2020, due to disruption of molybdenum supply chain, we used low specific activity Tc-99m pertechnetate elute (0.5–2 mCi of 99mTcO4 in 5 mL) for each kit preparation. Two or three intradermal periareolar injections were done for each patient (0.02–0.1 mCi/0.2 mL for each injection). Immediately following injection, dynamic lymphoscintigraphy was done. Surgery was done the same day of injection and the axillary sentinel node was sought using a gamma probe. Overall, 35 patients were included in the study. The specific activity of the Tc-99m elute (in 5 mL) used for kit preparation was 2 mCi/10 mg in four, 1.5 mCi/10 mg in eight, 1.25 mCi/10 mg in eight, 1 mCi/10 mg in three, 0.75 mCi/10 mg in five, and 0.5 mCi/10 mg of 99mTc-Phytate in seven patients. For the first four groups of patients, we used two 0.2 mL injections, while in the latter two groups, three 0.2 mL injections were used. At least one sentinel node was detected in all patients but three in whom axilla was involved.
Conclusion:
Sentinel node biopsy can be achieved with low specific activity of Tc-99m elute at the time of Mo99-Tc-99m generator shortage. If special personal protection is used, sentinel node mapping can be done in nuclear medicine departments with excellent results despite the COVID-19 pandemic and disruption of generator shipment.
Introduction
Lymphatic staging of solid tumors is an important aspect of surgical oncology. Historically, lymph node dissection during surgery was considered a gold standard for this purpose for many tumors, including breast cancer and melanoma. 1 With the advent of sentinel node mapping, lymphatic staging of many solid tumors has been changed drastically and lymph node dissection is not needed in patients with pathologically noninvolved sentinel nodes. The concept of sentinel node biopsy is considered the standard of care in many cancers, including breast cancer, melanoma, gynecological, gastrointestinal, and urological cancers.2–7
Sentinel node mapping can be done by various methods, including radiotracers, dyes, and magnetic materials.8,9 Thus far radiotracers are used most frequently due to better access to nuclear medicine facilities as well as better design and cost effectiveness of gamma probes.
On February 3, 2020, the World Health Organization (WHO) declared a public health emergency, and on March 11, declared COVID-19 a pandemic. 10 The COVID-19 pandemic changed the world dramatically and one of the consequences has been disruption of molybdenum 99 supply and shortage of Mo99-Tc-99m generators. 11 Although nuclear medicine societies have addressed the COVID-19 pandemic in several guidelines, they mostly covered the protection of the patients and personnel against COVID-19 infection.12–15
In the current study, we reported our experience on sentinel node mapping of breast cancer patients during the extreme shortage of Mo99-Tc99m generators using Tc-99m phytate.
Materials and Methods
During the period from March 7, 2019, to April 18, 2020, due to disruption of molybdenum supply chain, no Mo99-Tc99m generator was provided in our nuclear medicine department. The last shipment of the generators was on February 29, 2019, with two 600 mCi generators calibrated for February 29.
In this period, we had 35 early breast cancer patients (clinically N0) referred to our department for sentinel node mapping and lymphoscintigraphy. In our department, we use Tc-99m phytate for sentinel node mapping.16,17 The Phytate kit is a vial of sterile, nonpyrogenic, lyophilized powder that contains a mixture of 10 mg phytic acid and 1 mg Sncl2. For preparation of the kit, up to 100 mCi freshly eluted Tc-99m pertechnetate in 2–5 mL should be added to the kit, and incubated for 15 minutes. 99mTc-Phytate has to be used within 6 hours, where its radiochemical purity is more than 90%. No lower limit for added activity is provided by the supplying company.
Instant thin-layer chromatography on silica gel was performed using methanol 85% for 99mTc-Phytate at Rf = 0–0.1, and Free Tc-99m at Rf = 0.55–0.7. The radioactivity was quantified by cutting the strip (1 × 10 cm2) into 1 cm pieces and counting in a well-type gamma counter (DL 100; Delshid).
We used low specific activity Tc-99m pertechnetate elute (0.5–2 mCi of 99mTcO4 in 5 mL) for each kit preparation. Molybdenum assay was done after each elution of the generators using a molybdenum assay canister.
Radiotracer injection was done on the gamma camera bed using insulin syringe in an intradermal manner. Two or three intradermal periareolar injections were done for each patient (0.02–0.1 mCi/0.2 mL for each injection). Immediately, following radiotracer injection, a dynamic lymphoscintigraphy was done (10 frames, 120 seconds each frame) using a variable angle gamma camera (Philips Medical Systems, The Netherlands) in a 90-degree configuration to image both anterior and lateral images. The gamma camera was equipped with a low-energy, high-resolution collimator and imaging was done at Tc-99m photopeak. Lymphoscintigraphy images were interpreted by two nuclear medicine specialists with expertise in sentinel node mapping. If no axillary sentinel node was visible on the dynamic images, delayed planar images were done (5 minutes/image in 90-degree configuration) 1 hour postinjection. Patients were sent to the operating room the same day of injection (2–3 hours postinjection) and any hot axillary sentinel node was sought using a gamma probe (Surgioguide; Partopardaz Persia). 18 The decision to perform axillary dissection was made following a frozen section assessment of the sentinel nodes. In case of pathologically involved sentinel nodes or sentinel node detection failure, axillary lymph node dissection was done. No blue dye was used for sentinel node mapping of the patients.
To minimize the risk of COVID-19 dissemination, we follow a strict protocol in our department. Each patient is asked specific questions regarding symptoms of COVID-19 and all relevant radiological and laboratory tests are reviewed. Any patient with suspicious laboratory, radiological, or clinical signs of COVID-19 infection is sent for further evaluation to special COVID-19 centers located in the city. All personnel should wear surgical mask, protective gowns, and face shields. Disposable table sheets are used for gamma camera tables and hand disinfectant dispensers are installed for patients and personnel. All patients should also wear masks (provided by the reception) during their entire time of presence in the department.
The study was approved by the local ethics committee under the approval number of 980234.
Results
Overall, 35 patients were included in the study (mean age = 48 ± 23). Table 1 shows the demographic data as well as sentinel node mapping results of the patients.
Demographic Data of the Included Patients
IDC, invasive ductal carcinoma; ILC, invasive lobular carcinoma.
The specific activity of the Tc-99m elute (in 5 mL) used for kit preparation was 2 mCi/10 mg in four, 1.5 mCi/10 mg in eight, 1.25 mCi/10 mg in eight, 1mCi/10 mg in three, 0.75 mCi/10 mg in five, and 0.5 mCi/10 mg of 99mTc-Phytate in seven patients. For the first four groups of patients, we used two 0.2 mL injections, while in the latter two groups, three 0.2 mL injections were used, corresponding to the overall dosage of 0.16, 0.12, and 0.1 mCi for the first three groups and 0.09 and 0.06 mCi for the last two groups of patients.
At least one sentinel node was detected in all patients but three in whom axilla was involved. Figures 1 and 2 show lymphoscintigraphy images of patient 24 and 31, respectively.
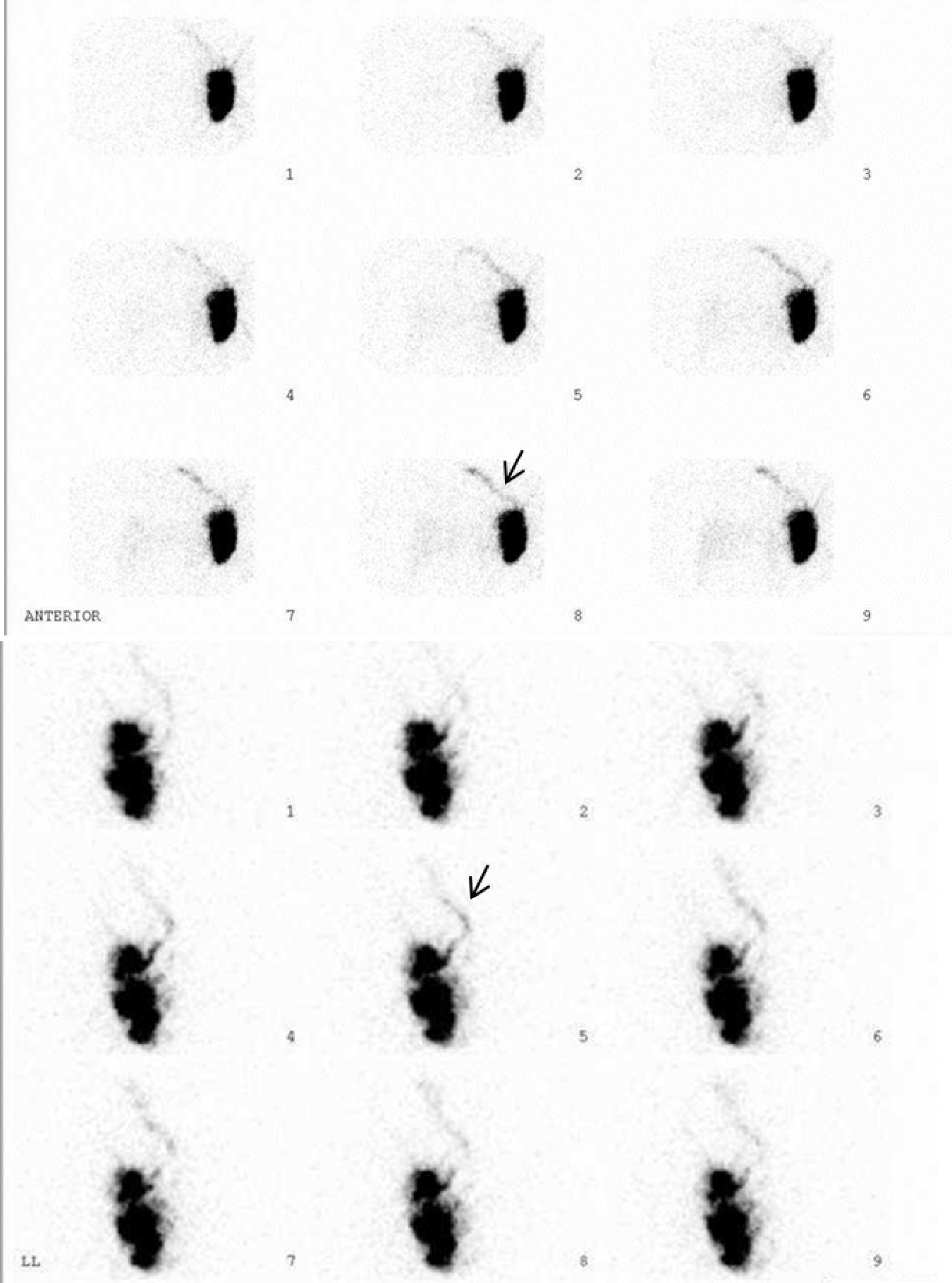
Anterior (top) and lateral (bottom) dynamic lymphoscintigraphy images of patient 24. Note lymphatic drainage to an internal mammary area (arrows) without any axillary sentinel node.
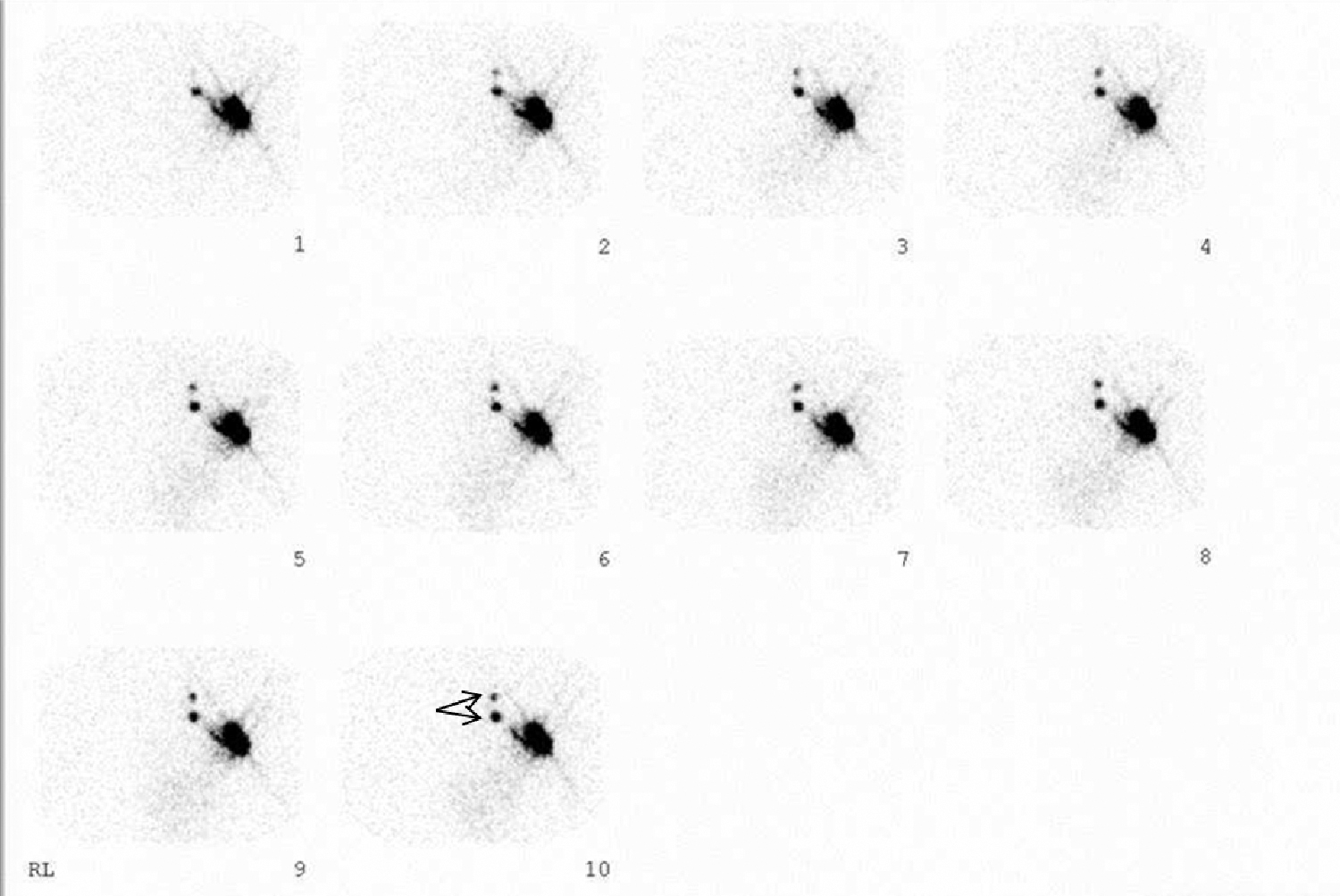
Lateral dynamic lymphoscintigraphy images of patient 31. Note two visible axillary sentinel nodes (arrows).
Discussion
Following several randomized trials on sentinel node mapping in breast cancer, this technique has replaced axillary dissection as the method of lymph node staging. 19 However, several aspects of sentinel node mapping were and are still under debate: type of the tracer, injection technique, injection volume, dose, and so on.20–26
Our study showed that even without a regular supply of Mo99-Tc99m generators, sentinel node mapping using radiotracer can be performed with excellent success. We used different specific activities during the length time that our study was done. The doses and specific activities were decreasing from the start to the end of the study as the generator yield continually decreased as time passes.
Sentinel node mapping was successful in all patients except for the three patients in our study. In those three patients with intraoperative harvesting failure, axilla was involved. Intraoperatively, surgeons could find sentinel nodes using a handheld gamma probe without difficulty in patients who had axillary sentinel nodes on lymphoscintigraphy. Actually the count rates of axillary sentinel nodes were at least 10 times higher than the background (thigh).
The time interval between radiotracer injection and operation was 2 to 3 hours in our study. Longer time intervals may increase the risk of sentinel node detection failure intraoperatively as the radioactivity in the sentinel nodes decays over time. Specifically, the center that uses the 2-day protocol (operation a day after radiotracer injection) may have difficulties regarding intraoperative sentinel node detection.
Effect of specific activity of the Tc99m elute for kit preparation on the success of sentinel node mapping has been evaluated in several studies before.27–30 Major results of these studies can be found in Table 2. All four previous studies on this topic showed that increased sentinel node count rate can be achieved by increasing the specific activity of the Tc-99m elute (by using 2-hour elute vs. 24-hour elute, using a proportion of a kit, or using a lower volume of Tc-99m for kit preparation). However, the results of sentinel node biopsy in the groups with low specific activity were minimally inferior to the high specific activity groups, and sentinel node detection was achieved in both groups in a satisfactory manner. Our study also was consistent with the previous studies as the sentinel lymph node count rates were consistently lower in groups with lower specific activity of Tc-99m compared with the higher specific activities. However sentinel node detection rate was not different between groups in our study, which shows that even very low specific activity of Tc-99m elute can be successful for kit preparation and sentinel node biopsy.
Results of the Studies on Effect of Specific Activity of Tc-99m Elute on the Successful Sentinel Node Mapping
Injection depth of the radiotracer is an important factor that can affect the count rate of sentinel nodes as well as the detection rate of the technique. In our study, we used the intradermal method of injection that yields the highest sentinel node count rate compared with subdermal and peritumoral injections. Actually, multiple studies confirmed that intradermal injection of the radiotracer resulted in higher count rates in the axillary sentinel nodes compared with the deep injections.31–35 Time to sentinel node visualization was also shorter with an intradermal injection, which is due to rich lymph tissue in this area of the skin.20,23 We did not have any experience with deep injections; however, deep injection techniques may also be as successful as intradermal injections.
Type of the radiotracer is another important aspect of sentinel node biopsy in surgical oncology. Surprisingly all radiotracers perform well for this purpose. 36 We used Tc-99m phytate in the current study with excellent results. Previous studies also showed successful sentinel node mapping using Tc-99m phytate. An important property of the Tc-99m Phytate kit is the ease of preparation without any need for filtering or boiling. In addition, the kit remains stable for 6 hours following preparation, which makes it a suitable radiotracer for sentinel node mapping.16,17,37,38
Two important aspects of sentinel node mapping in breast cancer patients (which are relevant in the time of radiotracer shortage) are volume of injection and dose of the radiotracer.
In our study, we used 0.2 mL volume for each injection as recommended by most guidelines for intradermal injections.39,40 As intradermal injection of the tracer can be very painful, it seems that 0.2 mL volume is optimal. Actually it has been shown that increasing the volume of intradermal injections can decrease the detection rate of sentinel nodes in breast cancer patients. 22 Anyhow the volume of injection does not seem to be a limiting factor in sentinel node mapping of breast cancer if divided doses are used for high volumes.
The major concern during the Mo99-Tc99m generator shortage is the dose of injections for sentinel node mapping. In our study, even doses as low as 0.06 mCi were successful for sentinel node mapping. The recommended dose of radiotracer for sentinel node biopsy of breast cancer patients differed widely in different guidelines and for different injection techniques.40–42 Although higher doses of radiotracer have been reported with a better detection rate in some studies, 43 doses as low as 0.2 mCi were also used with excellent results. 44 Our study showed that lower doses than usual can be successful and that sentinel node mapping should not be precluded in the breast cancer patients at the time of radiotracer shortage.
Conclusion
Sentinel node biopsy can be achieved with low specific activity of Tc-99m elute at the time of Mo99-Tc-99m generator shortage. Lymphatic mapping and biopsy should not be avoided under the context of radiopharmaceutical shortage. If special personal protection is used, sentinel node mapping can be done in nuclear medicine departments with excellent results despite the COVID-19 pandemic and disruption of generator shipment.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was funded by the Vice Chancellery of Research; Mashhad University of Medical Sciences, Mashhad, Iran (Grant no. 980234).