
Abstract
Background:
To investigate the role of tissue dielectric constant (TDC) in the detection and assessment of breast cancer-related lymphedema (BCRL) and to determine whether the TDC could potentially be used as a complementary method for arm volume measurement.
Methods:
Sixty-nine patients with BCRL were enrolled in this study. Local tissue water was assessed bilaterally by using the TDC method in four sites: upper arm, forearm, hand, and lateral thorax. Arm circumferences were measured at the 4-cm interval, starting from the shoulder to the wrist by using a tape measure. The arm volume was calculated by a standard formula. Patients' demographic information and clinical characteristics were also recorded.
Results:
Fifty-one of the 69 patients were diagnosed with clinical lymphedema. Using a TDC ratio of 1.2 or a diagnostic reference standard of ≥2 cm arm circumference, the sensitivity of these two methods was found to be identical at 73.9%. The TDC values in four sites on the affected side were significantly higher (p < 0.05) relative to the unaffected side. The inter-side TDC ratio of upper arm and forearm was substantially higher than that of lateral thorax and hand (p < 0.05). The TDC ratio of upper arm, forearm, and hand, especially of the upper arm and forearm, was positively correlated with inter-limb volume difference and stage of lymphedema.
Conclusion:
The TDC method elucidated a meaningful clinical correlation to the arm volume measurement. Applying those two methods together showed promise in the detection and assessment of BCRL. The forearm and upper arm were reliable examination sites for TDC measurements in the clinic.
Introduction
Breast cancer-related lymphedema (BCRL) is a common complication that affects survivors after breast cancer surgery. 1 BCRL causes physical symptoms such as pain, heaviness, and loss of joint range of motion along with psychological symptoms such as a changed body appearance, decreased self-esteem, and diminished social relationships. 2 There is currently no cure for lymphedema. Early detection of lymphedema and appropriate intervention are critical to prevent disease progression and provide effective treatment for a chronic progressive disease.3,4
The incidence of BCRL was between 5.6% and 28.2%. 5 With an increasing number of long-term breast cancer survivors, 6 the number of cases may continue to rise. As reported in the articles, the variation in incidence rate primarily depends on the diagnostic method used. Various types of methods have been developed and used to aid in clinical evaluation of BCRL, including quantitative methods such as volume measurements (limb circumferences, water replacement, perometry), bioelectrical impedance analysis (BIA), tissue dielectric constant (TDC), or imaging technology such as ultrasound, lymphoscintigraphy, magnetic resonance lymphography, and near-infrared fluorescence imaging. Among these, the volume measurement is the most commonly used method in the clinic. The TDC is a noninvasive technique that has attracted attention in recent years. Studies have showed that TDC can be used in the early diagnosis and efficacy evaluation of BCRL 7 and is more sensitive and convenient than BIA, because it can be easily applied to almost any site of the body.8,9 Each method has its advantages and limitations. Considering the complexity of BRCL, using several complementary methods will likely be more accurate, as well as efficient for early detection and assessment of lymphedema. Identifying the closely correlating methods and applying those in clinics is of great importance. The TDC and volume measurement are two methods that we are interested in investigating. The purpose of this study is to ascertain whether the results of TDC correlate to volume measurement and to determine whether the complementary application of TDC and arm volume measurements could potentially be used as a diagnostic method for early lymphedema in the clinical setting.
Methods
Conduct of study
The study was approved by the Medical Ethics Committee of Peking Union Medical College Hospital, Beijing, China and was conducted after the Helsinki Declaration. Written informed consent was obtained from each patient before the initiation of the study.
Study design and study population
This study was a single-center, cross-sectional, and noninterventional study executed at the Peking Union Medical College Hospital. TDC and volume measurements were conducted on each patient. Sixty-nine female breast cancer survivors who underwent axillary lymph node dissection and complained of swelling or heaviness in the affected side throughout China were eventually enrolled.
Inclusion criteria
Breast cancer survivors with a history of mastectomy, complaint of swelling or heaviness in the affected side, and diagnosed as lymphedema stage 0–2 (Table 1) using the grading standard issued by the International Society of Lymphology (ISL) in 20167,10 were included in this study.
Clinical Features of Patients with Breast Cancer-Related Lymphedema (n = 69)
The stage of lymphedema was evaluated by using the grading standard issued by the ISL in 2016.
ISL, International Society of Lymphology.
Exclusion criteria
The following situations were excluded from participation in the data collection: survivors who had any evidence of cancer metastases or recurrences; a history of bilateral breast cancer; venous insufficiency, acute thrombophlebitis, or deep venous thrombosis; cellulitis; co-morbid conditions such as congestive heart failure, renal failure, and musculoskeletal, neuromuscular, or cerebrovascular disease that may influence upper limbs.
Eighty-one women with stage 0–2 BCRL enrolled in the study initially. Twelve patients with cancer metastases or recurrences (n = 2), bilateral breast cancer (n = 1), or combined with other diseases (n = 9) were excluded. Finally, 69 eligible patients were investigated. The mean age was 54.4 ± 9.3 years, and the mean body mass index was 25.4 ± 2.5 kg/m2. Forty-nine of 69 patients (71.0%) had completed radiotherapy before they participated in this study (Table 1). The median postoperative time was 26 months. The course of BCRL was 0.5 months to 10 years (Table 2). All the patients were right-hand dominant. Twenty-nine of 69 patients (42.0%) were diagnosed with breast cancer on their dominant side.
Demographic Characteristics of Patients with Breast Cancer-Related Lymphedema (n = 69)
BCRL, breast cancer-related lymphedema; BMI, body mass index.
TDC measurements
The local tissue water (LTW) on the arm, trunk, and hand was measured by using the TDC method (MoistureMeterD Compact; Delfin Technologies Ltd., Kuopio Finland). MoistureMeterD is a portable device that consists of an electronic control unit and an integrated probe. 11 A high-frequency electromagnetic wave is transmitted into the probe in contact with the skin. The portion of the electromagnetic wave reflected depends on the TDC, which, in turn, depends on the amount of water in the tissue under the probe. 12 A probe with a diameter of 23 mm and a detection depth of 2.5 mm was selected in this study. Four measurement sites were located at 8 cm proximal to the antecubital fossa in the ventral midline; 6 cm distal to the antecubital fossa in the ventral midline; 10 cm inferior to axilla on the midaxillary line; and the midpoint of the third metacarpal bone on the dorsum of hand.7,13 During the examination, patients took a supine position with their elbows extending and shoulders relaxed in the abduction position of 30°. The probe was vertically placed in contact with the skin with constant and gentle pressure for 3 to 4 seconds. The LTW was measured following the same procedure by the same rater to ensure the measurement pressure was consistent across all of the sites and study participants. Triplet measurements were conducted at each site. The inter-side TDC ratio was calculated by using the following formula: The inter-side TDC ratio = TDC value in the affected side/TDC value in the unaffected side. The TDC values may vary by site and depth, but the inter-side ratio is relatively consistent. 14 Also, a study investigating the effect of handedness in healthy female adults indicated that limb dominance had no impact on TDC values or ratios. 15 Therefore, we set 1.20 as the diagnostic threshold of the TDC ratio on all of the four measurement sites.
Volume measurements
Arm circumferences were measured at the 4-cm interval, starting from the ulnar styloid to the shoulder with a tape measure. Arm volumes were calculated based on the arm circumferences, and the sum of segmental volumes was calculated by using the frustum model.16–21 Same as the TDC measurement, all the patients were measured by the same researcher using the same procedure with the same tape to ensure the intra-rater reliability. Clinical lymphedema was considered to be present when there was a ≥2 cm circumference difference at any measured point on the arm, or a ≥200 mL and/or ≥10% volume difference of the whole arm from the ulnar styloid to the shoulder between the affected and unaffected limbs. 22
Due to the natural physical inter-limb volume variations, the right-to-left arm or left-to-right dominance ratio was also considered in the study. The right-arm volume of right-hand dominant women is 1.6% greater than the left arm, whereas the left-arm volume of left-hand dominant women is 1.4% higher relative to the contralateral limb. 23 So right-to-left arm dominance ratio for right-hand dominant women is 1.016. For a right-hand dominant patient with right-side breast cancer, the required threshold ratio for a 10% increase would be 1.10 × 1.016 = 1.118; if tumor occurs on the left side, the left-to-right threshold ratio would be (1/1.016) × 1.10 = 1.083. 11
Statistical analysis
The data were analyzed with SPSS 19.0 statistical software. A paired t-test was used to compare the affected and unaffected side. One-way ANOVA and S-N-K were used to determine the difference among various sites. Pearson method was used for correlation analysis. The statistically significant difference is p < 0.05.
Results
According to the arm volume diagnostic standard, the sensitivity of clinical lymphedema in this study was 73.9% (51/69). Moreover, using the inter-side TDC ratio threshold of 1.2,8,24 the sensitivity of the TDC method was also found to be 73.9% (51/69) (Fig. 1). However, the two methods had different diagnostic sensitivities for patients with different clinical stages. Stage 0, namely subclinical lymphedema, was difficult to detect by volume difference. However, 44.4% of these patients were diagnosed as clinical lymphedema by the TDC method (Table 3). Lymphedema in stage 1 and stage 2 was easy to detect by circumference and volume difference, and the sensitivities of both diagnoses were 100.0% (Table 4). The sensitivity of TDC method in the diagnosis of stage 2 lymphedema was 96.2%, which was very close to that of volume measurement. However, the sensitivity of the TDC method in the diagnosis of stage 1 lymphedema was only 52.0% and it was lower than that of volume measurement.
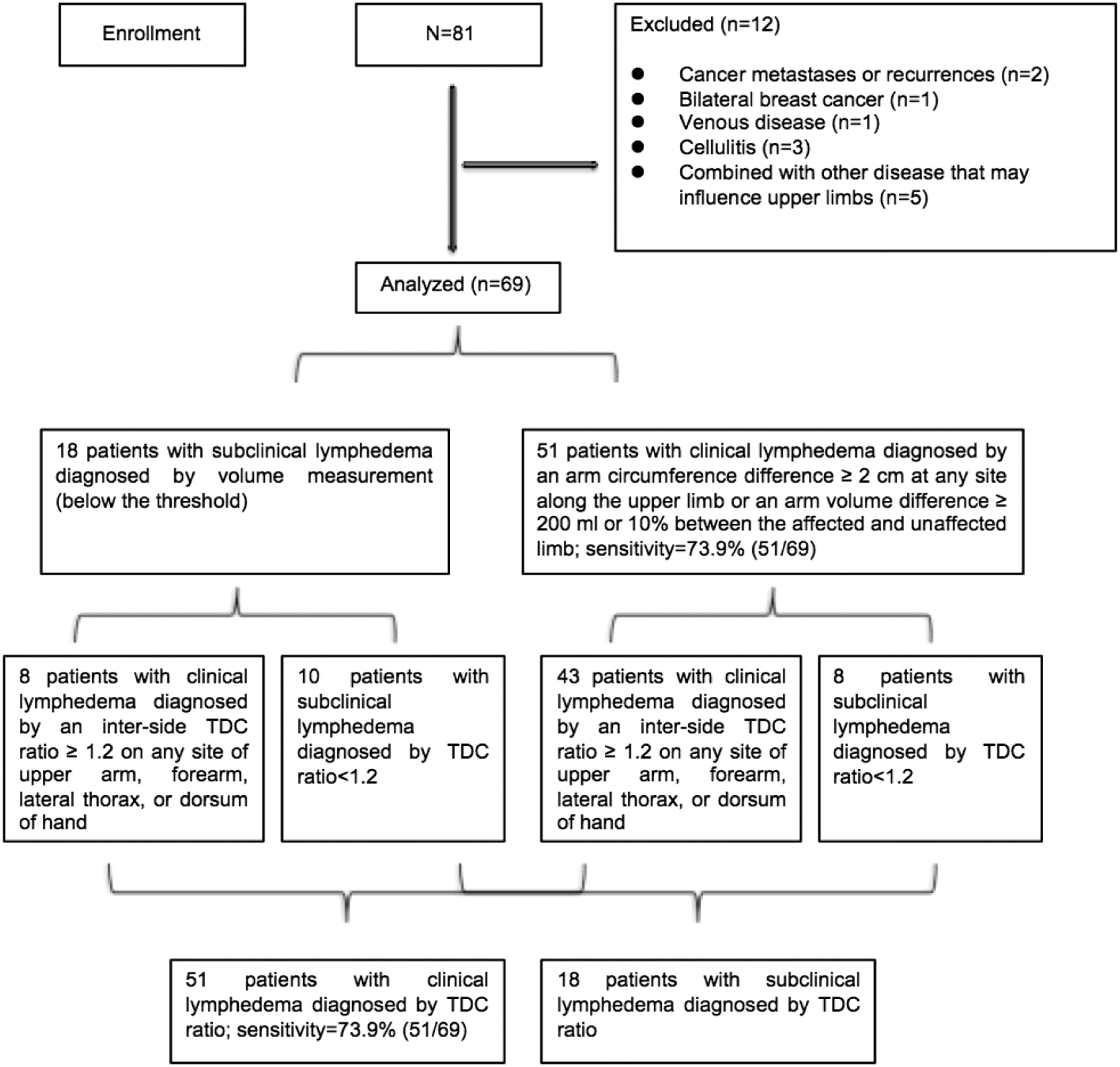
Enrollment of participants; diagnosis of BCRL with TDC method and volume measurement: patients were diagnosed with clinical lymphedema if the threshold was exceeded. BCRL, breast cancer-related lymphedema; mL, milliliter; TDC, tissue dielectric constant.
Number of Subjects Diagnosed as Clinical Lymphedema and the Sensitivities of Diagnosis with Inter-Side Tissue Dielectric Constant Ratio by Stage (n = 69)
Sensitivities of diagnosis: The total number of subjects diagnosed as clinical lymphedema by TDC ratio more than 1.20 at each measurement point. The patient with TDC ratio more than 1.20 at two or more measurement points was counted as one subject.
TDC, tissue dielectric constant.
Number of Subjects Diagnosed as Clinical Lymphedema and the Sensitivities of Volume and Circumference Measurements by Stage (n = 69)
The stage of lymphedema was evaluated by using the grading standard issued by the ISL in 2016.
The average volume of the affected limb was 2415.9 ± 642.9 mL, and that of the unaffected arm was 2023.4 ± 401.4 mL. The volume difference between arms was 392.5 ± 396.7 mL; the percentage of inter-limb volume difference was 19.1% ± 18.7%; and statistically significant (p < 0.05) differences were observed between the affected and the unaffected arms.
The TDC value of all the measurement sites on the affected side was significantly higher compared with the unaffected side (p < 0.05, Table 5). Among the sites tested, the TDC ratio of the upper arm and forearm was higher than that of the lateral thorax and the dorsum of the hand (p < 0.05). However, there was no significant difference observed between the TDC ratio of the upper arm and the forearm (p > 0.05), or of the lateral thorax and the dorsum of the hand (p > 0.05, Table 6).
Comparison of Tissue Dielectric Constant Value and Inter-Side Tissue Dielectric Constant Ratio Between the Affected and Unaffected Side (n = 69, Means ± Standard Deviations)
Denotes a p-value <0.05, showing a significant difference between the affected and unaffected side.
Comparison of Inter-Side Tissue Dielectric Constant Ratio Among Four Measurement Sites (n = 69, Means ± Standard Deviations)
Denotes a p-value <0.05, showing a significant difference compared with the upper arm.
Denotes a p-value <0.05, showing a significant difference compared with the forearm.
According to the statistical analysis, the inter-limb volume difference was positively correlated with the TDC ratio of the forearm, upper arm, and the dorsum of the hand (p < 0.05). The correlation coefficients were 0.644, 0.560, and 0.407, respectively, among which the correlation coefficient of the TDC ratio of the forearm was the highest. However, there was no correlation observed with the lateral thorax (p > 0.05, Table 7).
Correlation of Inter-Limb Tissue Dielectric Constant Ratio and Volume Difference (n = 69)
Denotes a p-value <0.05, showing a positive correlation with inter-limb volume difference.
In addition, our study also indicated that the TDC ratio was closely related to the ISL stage of lymphedema (p < 0.05). Similar to the data discussed earlier, the upper arm, forearm, and the dorsum of the hand were the sites that showed a significant difference; the correlation coefficient of the forearm was the highest (0.571, Table 8).
Correlation of Tissue Dielectric Constant Ratio of Four Measurement Sites and the International Society of Lymphology Stage of Lymphedema (n = 69)
Denotes a p-value <0.05, showing a positive correlation with the ISL stage of lymphedema.
Discussion
It is generally believed that conventional methods used for volume measurements are sufficient to detect the clinical lymphedema but are not sensitive enough to detect minor changes in extracellular fluid and latent lymphedema. 25 BCRL may be initially manifest in the skin and subcutaneous tissue early.11,26 LTW measurement has been shown to be a sensitive predictor of those earliest changes. 8 TDC and BIA have been used as the detection methods for early lymphedema.8,27–29 Although BIA devices are considered to be capable of differentiating intracellular and extracellular fluid volume, several caveats are limiting the extensive usage of BIA. First, BIA cannot be used to inspect the trunk, and in some instances, they are unable to be used because of its low current intensity. 11 Second, BIA or total limb volume measures cannot provide localized evidence of fluid volume. Therefore, alternative approaches such as TDC 30 are needed to allow for localized assessment of early LTW changes in the skin and subcutaneous tissues of limbs, trunk, and other body parts. Recent studies have indicated that TDC is more sensitive than BIA regarding the early detection of lymphedema.11,14 The depth of the TDC measurement is critical for accurately detecting the early changes of lymphedema. The probe of our TDC device used in the study has an effective measurement depth of 2.5 mm, which can only be detected in the skin and subcutaneous tissue, where the most initial changes occur.11,31 This feature allows us to potentially measure any anatomical site that may be at risk for developing lymphedema. 12 The TDC method could be an accurate and flexible method for the assessment of BCRL.
Our study demonstrated that the TDC ratio of each measurement site on the arm was positively related to the inter-limb volume difference; the results were consistent with Bakar's study, which also regarded 1.2 as the threshold of the TDC ratio. 7 The global TDC threshold has not been unified. Mayrovitz’ study suggested that a ratio of ≥1.2 could be used as a threshold to detect clinical lymphedema. 24 The mean value of the inter-side TDC ratio of our study on both the ventral forearm and the upper arm was 1.2. We found that the sensitivity of the diagnosis of BCRL using the inter-side TDC ratio threshold was 73.9%, which was firmly correlated to the sensitivity defined by the volume diagnostic standard. For severe lymphedema in stage 2, these two methods had similar sensitivities of diagnosis. The TDC method was more sensitive to detect latent lymphedema than volume measurement, which seemed to be more suitable for the early diagnosis of stage 1 lymphedema. Our data suggested that the TDC method was as important as volume measurement for BCRL, especially for the early detection of subclinial lymphedema, and these two methods could be used complementarily. The sensitivity of our study was 8.9% higher than in Bakar's study. 7 Unfortunately, they did not mention the number of BCRL cases enrolled in every stage. We assumed that the differences might be related to the postoperative time, course, and severity of lymphedema in patients involved or due to more TDC measurement sites used in our study.
The findings of this study could help to select the site with more identification value for the detection of BCRL. TDC is site-specific. The standard clinical diagnostic site is to be determined. Usually, preclinical or mild lymphedema may only occur in certain areas, such as the distal limb. For early detection of lymphedema, it is necessary to examine multiple sites, which will inevitably require more time. In clinical practice, it is not feasible for clinicians to measure TDC of various sites on the trunk, limbs, or hands. Therefore, it is of great importance to prioritize the measurement sites based on sensitivity. The diagnostic sensitivity of the TDC ratio of the forearm and upper arm in our study was significantly higher than the trunk and hand. Data suggested that for latent or mild BCRL patients, the ventral forearm might be the first choice for TDC detection, followed by the ventral upper arm. If time permits or if a patient has a complaint of swelling in her trunk or hand, further examination of these areas can be performed.
As we know, it has been quite challenging to measure truncal lymphedema due to the inability to perform side-to-side comparisons by using measures of total volume such as water displacement, perometry or circumferential assessment. Also, preoperative to postoperative comparisons using full-volume measures are challenging because of the anatomical changes in the breast after cancer surgery. As mentioned earlier, although there was no correlation of the TDC ratio on truncal sites to the arm volume measurement observed, the actual TDC values on the affected side were significantly higher than the unaffected side. This evidence indicated that the TDC method could be a reliable method for the assessment of BCRL in the trunk.
To be transparent, we would like to address that due to the limited resource and study duration, there were only 69 patients enrolled in the study. The sample size was relatively small, and we were not able to include a control group. Also, it is difficult to define the stages of lymphedema, postoperative time, or course with a limited number of patients. To date, there is no unified threshold of the TDC ratio,8,11,12,24 and additional harmonized studies are still needed in the future.
In conclusion, our study indicated that TDC was a reliable and flexible method for screening, diagnosis, and quantitative evaluation of BCRL in the clinic.
The TDC ratio of the forearm and upper arm was a more sensitive indicator and had better clinical-stage differentiation of lymphedema. The TDC ratio and arm volume demonstrated a significant clinical meaningful correlation. Meanwhile, they had their own advantages in the early diagnosis of mild or subclinical lymphedema, respectively. Based on the data of this study, we would like to suggest that the complementary combination of TDC and arm volume measurement might be a promising diagnostic approach for early detection and objective assessment of lymphedema.
Footnotes
Acknowledgments
The authors thank Dr. Lixia Chen, Dr. Qiang Sun, Dr. Meixia Bi, and Miss. Xiaojuan Du for their kind support and help. They are grateful to the patients for them having participated in this study. The work reported in this article would be incredible without them.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.