
Abstract
Lymphatic and mixed malformations are rare and variable in presentation. They arise due to errors in vascular and lymphatic formation during early embryonic development. This leads to persistent infiltration of lymph fluid into soft tissues and causes a locally invasive mass with pathologic sequelae. Departing from historically descriptive terminology, such as “cystic hygroma,” lymphatic malformations are now categorized as macrocystic, microcystic, or mixed lesions, based on size. Advances in imaging modalities, such as ultrasonography and magnetic resonance imaging, have made accurate characterization of these lesions possible and ultimately allow for early diagnosis and implementation of appropriate treatment based on the morphology of the lymphatic malformation. Management of lymphatic malformations can be quite challenging, and a multidisciplinary approach is most effective for optimum aesthetic and functional outcomes. New discoveries in the molecular biology of lymphatic malformations have provided treatment targets and established a role for pharmacotherapy. Sclerotherapy, laser, and radiofrequency ablation have all proven to be effective as minimally invasive treatment options for lymphatic malformations. Surgical intervention has a role in the treatment of focal lesions recalcitrant to these less invasive techniques. Operative planning is dictated by clinical goals, size, anatomic location, characteristics, and extent of infiltration.
Introduction
Lymphatic and mixed malformations (LMs) arise due to errors in vascular and lymphatic formation during early embryonic development and result in lymphatic, capillary, venous, or arteriole vasculature with abnormal make-up and connectivity. These vascular anomalies follow a diverse range of natural histories and include microcystic, macrocystic, and mixed lesions spanning across a multitude of pathologies. The characteristic abnormal connectivity of these lesions leads to decreased lymphatic drainage and results in persistent infiltration of lymph fluid into soft tissues, ultimately causing a locally invasive mass and pathologic sequalae. 1 Although manifestations of LMs differ with their sub-pathophysiology, they often manifest as lymphedematous limbs, accumulation of lymphatic fluid within a body cavity, diffuse infiltration and overgrowth, or localized masses. 2 Although the exact prevalence of LMs is unknown, it is likely higher than reported. Affected patients suffer from a wide array of problems related to their disease. New discoveries in basic science research have allowed for a deeper understanding of pathogenesis and cytogenetics, thereby improving the nomenclature and updating diagnostic and therapeutic modalities for LMs. Institutional Review Board review was not required for the submission of this article.
Pathogenesis
Molecular mechanisms of normal lymphatic development
Normal lymphatic development occurs early in embryologic development and leads to the development of an organized system in which interstitial fluid, proteins, antigen presenting cells, and white blood cells are transported from tissues and lymph nodes into venous circulation via unidirectional channels with one-way valves. 3 Embryologic development of lymphatics is a complex and heavily debated subject. Several theories exist, but the most widely accepted “centrifugal theory” proposes that lymph vessels are derived from central embryonic veins and can be divided into three separate processes: lymphvasculogenesis, lymphangiogenesis, and remodeling. This refers to de novo formation of lymph sacs via lymphangioblasts, lymphatic development from pre-existing lymphatic vessels mediated by lymphangiogenic growth factors, and maturation of immature lymph vessels to include valves and smooth muscle to lymph transport, respectively.4,5 Molecular biologists have also revealed the importance of transcription factors SOX18, COUP-TFII, and PROX1 in the differentiation of lymphatic endothelium from embryonic veins, induction of lymphatic development, and maintenance of lymphatic identity. 6 Tyrosine kinases VEGFR3, previously called FLT4, and VEGFR2, along with their ligand VEGF-C, and growth factors VEGF-D, IGF-1, IGF-2, PDGF-BB, HGF, Angiopoietin-1, Angiopoietin-2, and FGF-2 have also been implicated as key players in lymphangiogenesis.4,7 FOX2 is an important transcription factor in later stages of lymphatic development, as it is required, in combination with NFATc1, in the formation of valves during remodeling. Throughout embryogenesis, angiogenesis and lymphatic development are synergistic systems with a crossover of angiogenic factors, such as FGFs, VEGFs, and angiopoietins, which also induce lymphangiogenesis. 8
Molecular mechanisms of pathological development
Early errors in lymphvasculogenesis, lymphangiogenesis, or remodeling can lead to abnormal lymphatic development. 4 LMs are congenital, sporadic, and thought to arise from somatic, rather than germline, mutations. The immunohistochemical identification of LMs is distinguished by the presence of markers D2-40 and LYVE-1 on endothelial staining. 9 Cytogenetics demonstrating abnormal regulation of TGFs and VEGFs are implicated in lymphatic dysmorphogenesis. Importantly, these mutations exert their effects downstream on PI3K pathways (Fig. 1). Postzygotic somatic mutations in phosphatyidylinositol-4,5-bisphosphate 3-kinase catalytic subunit (PIK3CA), which encodes the alpha subunit of enzyme PI3K, have been associated with isolated micro and macrocystic LMs, syndromes in which LM is a common feature, and some malignant tumors.10–13 It is unclear whether isolated PI3K mutations alone cause LMs or whether genetic mutations of the PI3K pathway could explain the differences in gene expression in microcystic and macrocystic LMs. These mutations can be seen in both subgroups 14 and have also been associated with some inherited forms of primary lymphedema. 13 Additional PIK3CA-related overgrowth syndromes with lymphatic components can be reviewed in Table 1.
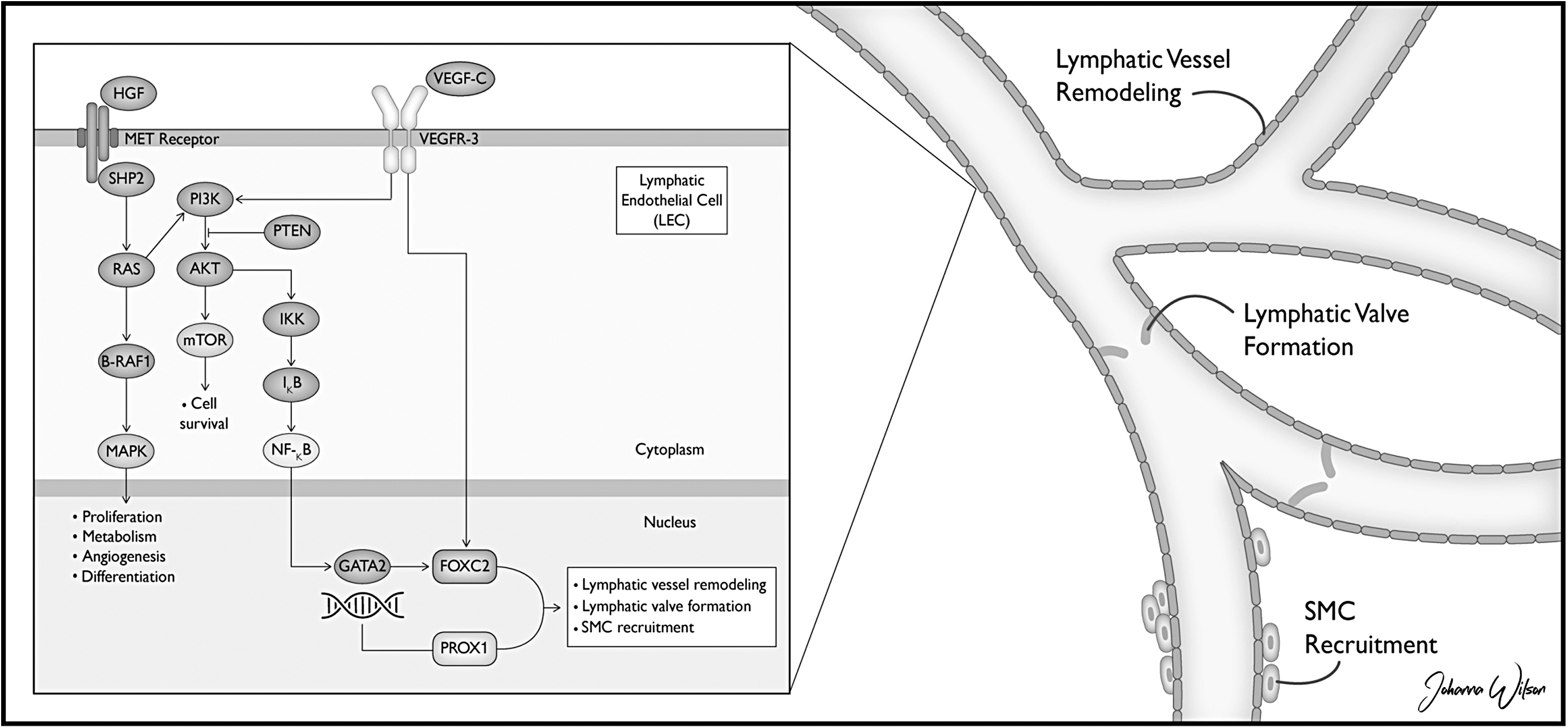
PI3K pathways.
PIK3CA-Related Overgrowth Syndromes
Classification System
The nomenclature of vascular anomalies and LMs has changed due to advancements in anatomy, pathophysiology, embryology, and diagnostic and therapeutic modalities. The vascular anomaly classification system developed by Mulliken and Glowacki is based on cellular kinetics and clinical behavior and classifies vascular malformations by either high-flow lesions (arterial malformations such as aneurysms, ectasia, stenosis, fistulas, and arteriovenous malformations) or low-flow lesions (capillary, venous, and lymphatic malformations). 15 The International Society for the Study of Vascular Anomalies (ISSVA) classifies LMs based on the size of the lymphatic channel, either microcystic, macrocystic, or mixed. 16 This nomenclature replaced previous descriptive terms such as cavernous lymphangioma, cystic hygroma, cystic lymphangioma, lymphangioma, lymphangioma circumscriptum, and lymphangiomatosis. These malformations are now grouped under the “lymphatic malformations” umbrella and subdivided by size. 2 Microcystic LMs comprised lymphatic locules less than 2 cm in diameter, whereas macrocystic LMs have locules larger in size.15,16 Discrepancy exists regarding the delineation between micro- and macrocystic lesions, some sources with a cutoff of 1 cm.14,17
The de Serres classification defines cervicofacial LMs based on anatomic location (supra or infrahyoid) and laterality (unilateral vs. bilateral) (Fig. 2). Stages range from I to V and are based on disease location and extent, with Stage V bilateral malformations containing both supra- and infrahyoid involvement. These lesions are both the most severe and most difficult to treat. 18 The de Serres staging system allows for more precise description of head and neck lymphatic malformations and has allowed for prediction of long-term prognosis based on anatomic location. 19
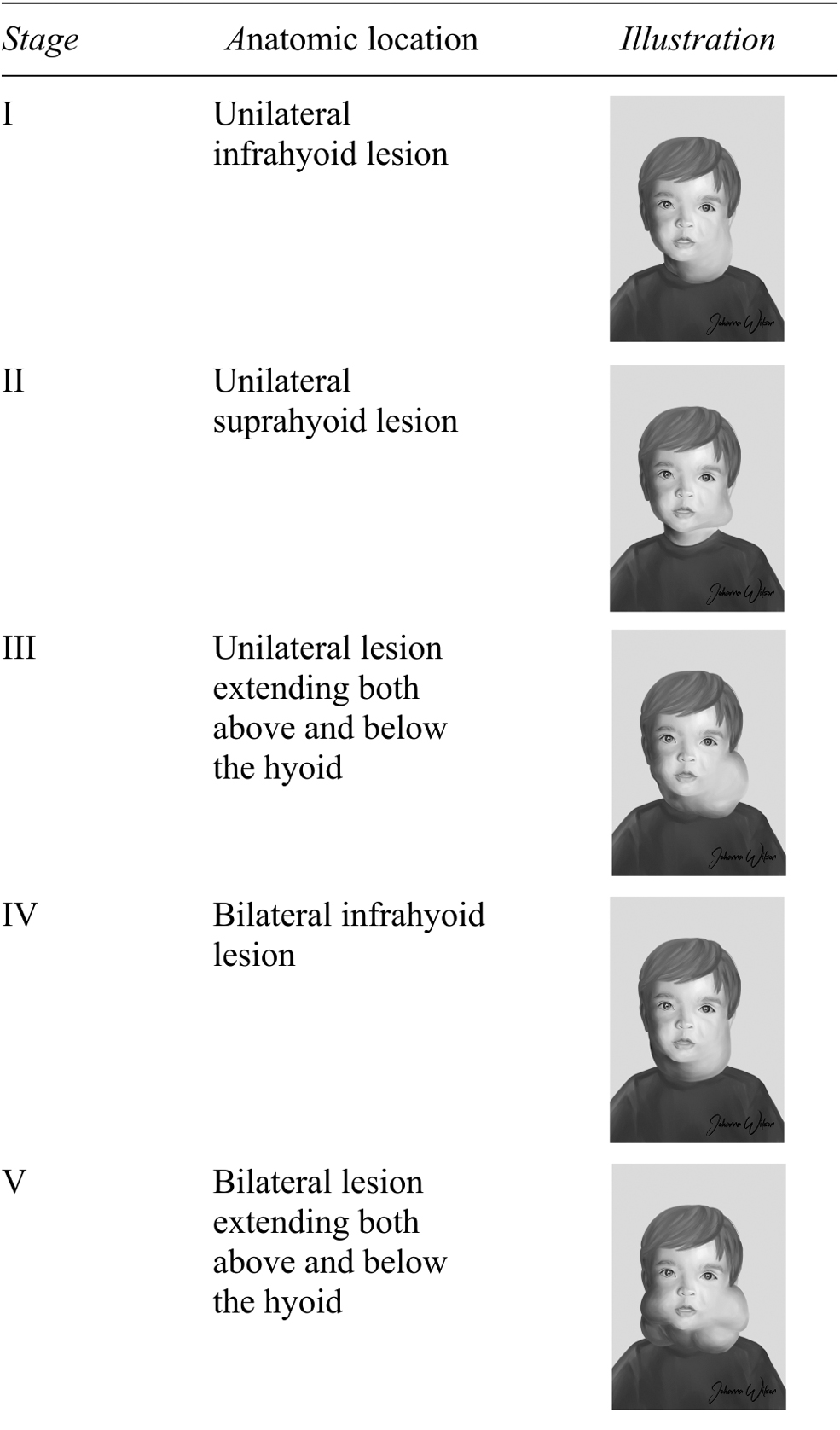
de Serres classification.
Epidemiology
The exact prevalence of LMs is not known but is quoted to be as high as 1/250 live births. 14 It is likely that underreporting of medically or cosmetically insignificant malformations—specifically in developing countries—further biases the true incidence.20,21 LMs are commonly noted at birth, but macrocystic lesions can even be detected in the late first trimester via prenatal ultrasonography (US). 2 The majority of LMs are apparent before 2 years, though LMs can present at any age. Some malformations have delayed presentation in adulthood or after a specific event, such as trauma, hormonal changes, spontaneous bleeding within the cysts, or infection. 22 LMs affect women and men equally and are phenotypically variable from patient to patient in their size, location, and characteristics. 23
Location and Morbidity
The LMs tend to be located in lymphatic-rich areas but can present anywhere on the body except the brain. The LMs of any location can bleed or become infected, but the location of each LM ultimately dictates morbidity.
Areas commonly affected include the head and neck (45%–52%), axilla (20%), groin, mediastinum, and retroperitoneum (5%).23,24 Although most cases have normal overlying skin, some lesions present with a bluish hue, deep cutaneous dimpling, vesicles, or intravascular bleeding evident as red dome-shaped nodules. 2 These lesions can lead to significant functional deficit, cosmetic disfigurement, pain, and can be life threatening if located near vital structures. Most LMs are initially painless, transilluminating soft tissue masses. Prenatal diagnosis of fetal neck LMs allows for pre-delivery planning for airway management. At times, the diagnosis is an indication for the ex utero intrapartum treatment procedure. 16 An estimated 62% of fetal LMs are associated with other syndromes and chromosomal aneuploidies, such as Noonan syndrome, Turner syndrome, Trisomy 21, 13, and 18. 24
Macrocystic lesions, often 3 referred to as “cystic hygroma,” are located in the cervicofacial region ∼80% of the time, tend to be below the level of the mylohyoid muscle, and involve both anterior and posterior cervical triangles. 18 Macrocystic LMs rarely communicate with normal lymphatic channels. Some cervical LMs have mediastinal or thoracic components and present with chylous pleural or pericardial effusions. 2 Most head and neck LMs are macrocystic; whereas lesions involving the mouth, tongue, and trachea tend to be microcystic, located in the anterior 2/3 of the tongue, violating anatomic boundaries, and may cause airway obstruction, malocclusion, excessive salivation, and speech difficulties. 25
The LMs involving the orbit make up 1%–8% of all orbital masses. 23 These lesions are often mixed, making treatment challenging due to infiltration of normal orbital structures. Orbital malformations can be asymptomatic or slow growing, with progressive proptosis, restricted eye movements, and diplopia. Acute hemorrhage or infection can cause compressive neuropathy and loss of vision, and in rare instances require decompression of the optic nerve. 26
Reports of intra-abdominal involvement are also rare, difficult to identify on imaging, and require a high index of suspicion for diagnosis. Magnetic resonance imaging (MRI) is the preferred diagnostic modality, though endoscopy can be helpful in certain locations. 22 Abdominal LMs comprise 5% of total LMs and are symptomatic in 88% of cases.27,28 Presenting symptoms may be nonspecific, such as abdominal discomfort, distension, nausea, or vomiting, but patients can also present with serious complications such as obstruction, volvulus, ischemia, bleeding, peritonitis, and abdominal compartment syndrome. 2 Retroperitoneal LMs can be complicated by ureteric obstruction and hematuria. 27 Pelvic LMs should be suspected in instances of recurrent urinary infection, constipation, or bladder outlet obstruction. 2
The LMs also occur in the arms and legs, as seen in Figure 3, which shows a focal LM of the left arm before surgical resection.
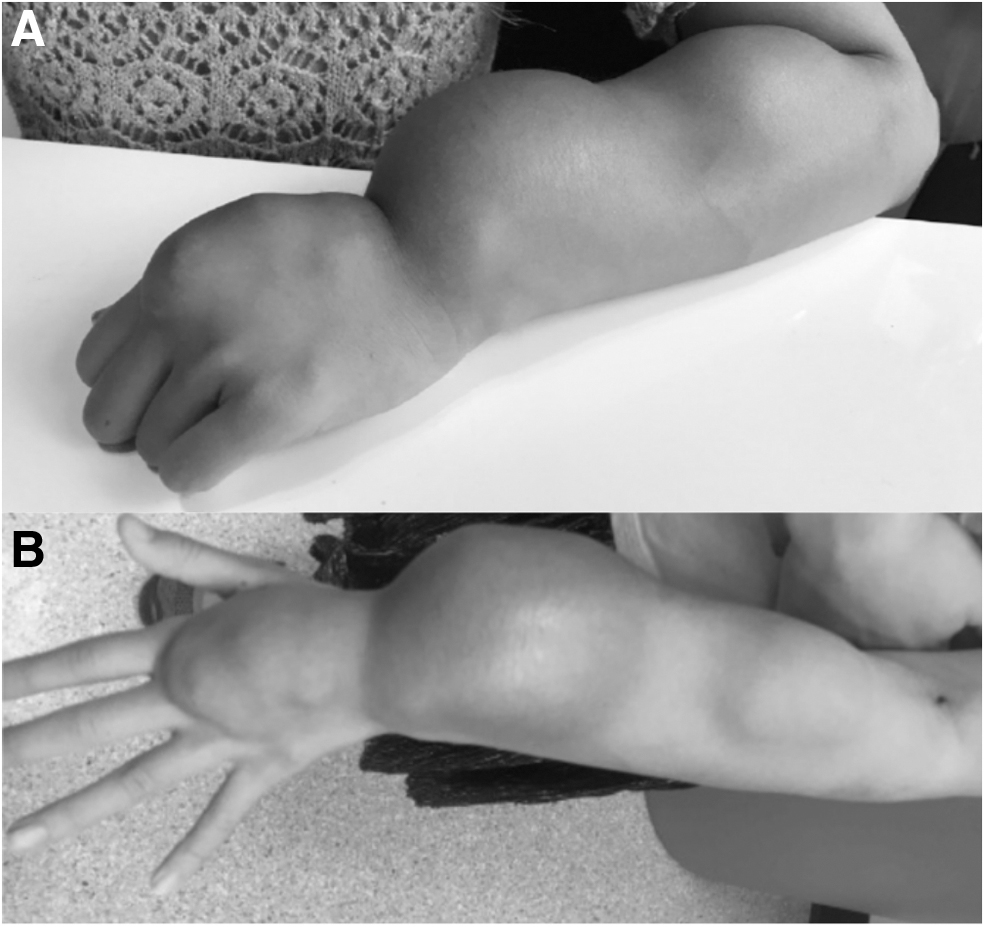
Preoperative photos of left upper extremity mixed micro- and macrocystic malformation.
Acute infection is more common in cutaneous LMs, as these lesions are associated with vesicle leakage. Spontaneous hemorrhage into the LM causes discoloration and pain. 23
Diagnostic Modalities
Early diagnosis of LMs allow for accurate staging, planning, and prediction of prognosis. Prenatal diagnosis offers opportunity for adequate planning for delivery and allows for early implementation of appropriate therapy before the onset of complications. 29 The main diagnostic tools are US and MRI (Fig. 4). Computed tomography (CT) should be avoided due to radiation exposure and used only when the size of the lesion and its relationship to surrounding structures needs further characterization. 30

Ultrasonography and magnetic resonance of microcystic and macrocystic LM of the left upper extremity.
Ultrasonography
After history and physical exam, US is the first-line diagnostic modality for all suspected malformations. Doppler US is used to determine flow characteristics and distinguishes between arterial, venous, capillary, lymphatic, and mixed malformations. 31 US is painless, radiation-free and gives real-time information about lesion characteristics. Purely macrocystic lesions appear multicystic, septated, hypoechoic, or anechoic (with no flow) on color doppler. 32 US imaging is less helpful for microcystic lesions, as these LMs are often deeply infiltrative within skin, fat, and muscle and cause distortion of normal anatomy, which is not easily visualized on US due to poor spatial resolution. 1 US is widely available and gives instant feedback on sclerotherapy injections and responses to other therapies.
Magnetic resonance imaging
The majority of patients diagnosed with LMs by US are referred for MRI. MRI is useful in characterizing both macro- and microcystic LMs and aids in accurate surgical planning. The signal of the fluid inside the cyst will be hypointense on T1- and hyperintense on T2-weighted images. 27 Heterogenous signals are seen when infection, inflammation, or hemorrhage is present. Compared with post-contrast MRI or CT images of vascular anomalies, which show arterial and venous components, there is no contrast enhancement in pure LMs. 33
Future—molecular targeting, photoacoustics, and photothermics
Sun et al. propose that the future of diagnostic workup and characterization of microcystic lesions lies with photoacoustic (PA) and photothermal (PT) flow cytometry, tomography, and spectroscopy for lymphatic mapping. These methods, in combination, have demonstrated promising results in vivo. Lymphatic mapping using nanoparticles injected intradermally into the ears of healthy mice showed successful migration to cervical lymph nodes in 3–5 minutes. The authors propose using surface biomarkers specific for LMs, such as LYVE-1 and D2-40, as molecular targets for PA and PT signals within the microcystic lymphatic network. This modality has implications for selective and targeted therapies directed at microcystic LMs. 1
Management
General principles
A multidisciplinary approach is necessary in the management of LMs and often requires coordinated effort of specialists in both medical and surgical fields. Treatment of LMs should be individualized, as approach depends on size, location, symptoms, pain, cosmetic deficits, and functional impairment. Many treatment modalities have been proposed with varying degrees of success, including invasive and non-invasive options. Historically, management of LMs relied heavily on surgical excision. Excision resulted in morbidity (bleeding and infection), high recurrence rates, and need for additional procedures. Fortunately, recent advances in medical management and minimally invasive techniques have allowed for a shift away from operative intervention, which is now reserved for only the most persistent cases. 34
Medical Management
Pharmacotherapy
Sirolimus, a rapamycin (mTOR) inhibitor, offers promising treatment results in patients with complex LMs. 35 In a retrospective review of seven neonates requiring ventilatory support due to large LMs, sirolimus was used as primary treatment and achieved complete resolution in one patient, partial resolution of the malformation with improvement of airway symptoms in five patients, and resolution of symptoms in one patient. Adverse effects are dose dependent and include hypertension, dyslipidemia, poor wound healing, bone marrow suppression (neutropenia, anemia, thrombocytopenia), and increased susceptibility to infections. Rare reports of Pneumocystis carinii pneumonia while on sirolimus support prophylaxis with trimethoprim-sulfamethoxazole. 36 Sirolimus and additional inhibitors of the PI3K/AKT/mTOR signaling pathway used in treatment of LMs 37 can be reviewed in Figure 5.
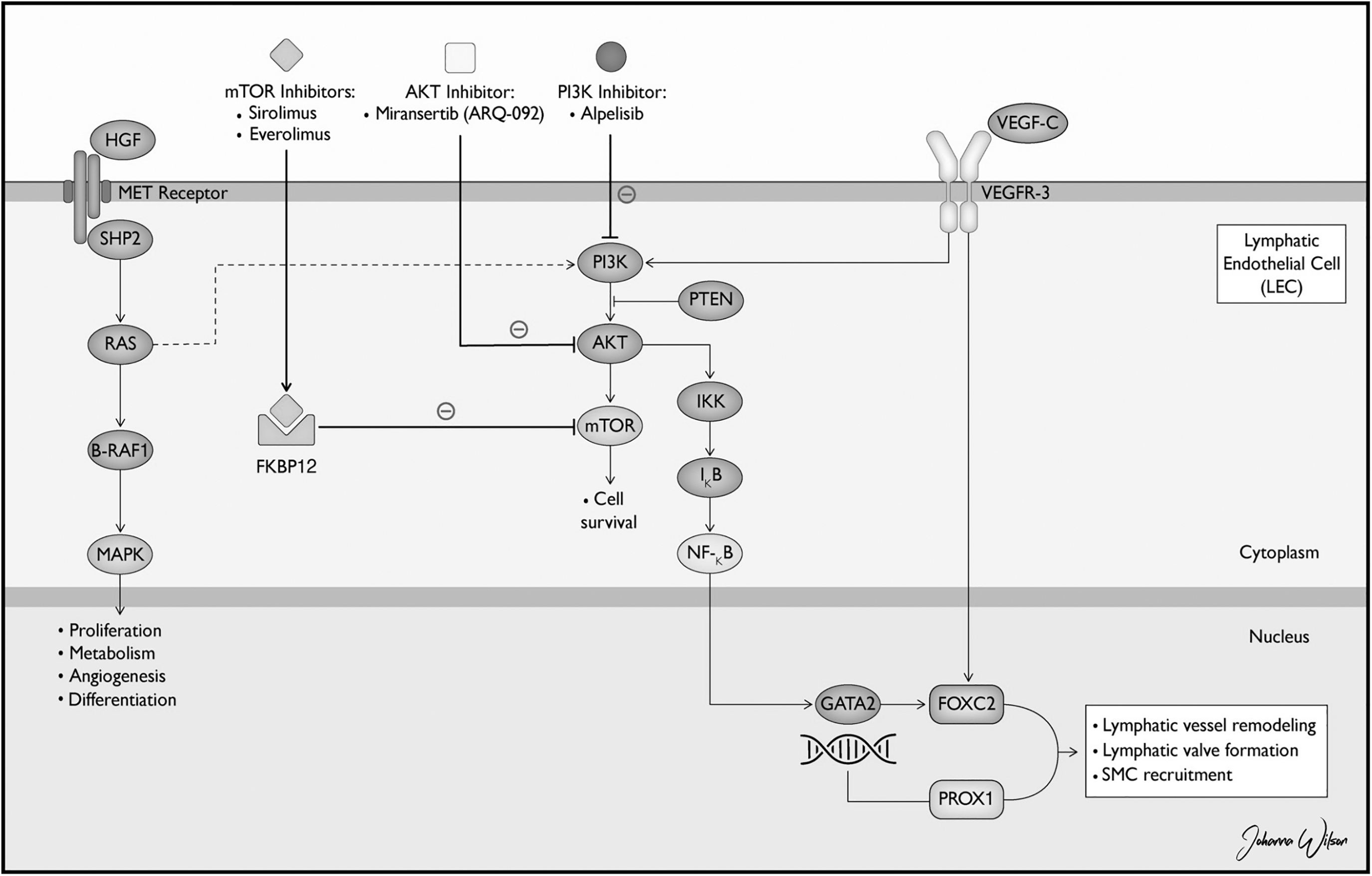
Pharmacotherapy pathways.
Sclerotherapy
Sclerotherapy is successfully used to treat large and symptomatic macrocystic LMs, but it is less effective and predictable in microcytic lesions due to the inability to insert a needle or catheter into the locules. 23 Sclerosing agents, such as bleomycin, picibanil (OK432), doxycycline, sodium tetradecyl sulfate (STS), pingyangmycin, and alcohol, are injected percutaneously or via catheter with ultrasound or fluoroscopic guidance. 15 Sclerotherapy is most commonly done by outpatient interventional radiology, with the purpose of inducing fibrosis for eventual shrinkage and collapse. It is a typically well-tolerated and easily repeatable procedure without scar and low risk of direct nerve injury. Risks include radiation exposure, skin necrosis, allergic reaction, and slow response to therapy.15,23 In a review of 40 cervicofacial LMs, sclerotherapy was used as first-line treatment in all cases, regardless of the type of LM, with complete resolution in 25% and significant improvement in 42% of cases. 30 Though best described and particularly effective in head and neck LMs, sclerotherapy can be used successfully in any location, as demonstrated in Figure 6, which shows an LM of the buttock before and after a series of intralesional bleomycin injections.

Microcystic LM of the buttock and perineum pre-sclerotherapy treatment.
Use of bleomycin, a chemotherapeutic agent that inhibits DNA synthesis by oxidative damage and induces inflammation within the cyst to cause fibrosis, is well described in the literature. 24 Risks include anaphylaxis, discoloration, and pulmonary fibrosis, which has never been described in intralesional treatment. 38
OK432, also known as Picibanil, induces inflammatory cytokines to shrink cystic spaces. Ohta et al. reported 83 patients with cystic lesions of the neck injected with OK432 with resolution of 76% of lesions. Side effects included temporary pain, swelling, and low-grade fever in approximately half of patients. 39 Doxycycline and STS are reliable alternatives to surgery in macrocystic malformations, though doxycycline was noted to have better cosmetic outcomes with less frequent treatments compared with STS. 40 Bai et al. reviewed outcomes of 79 patients who received intralesional sclerotherapy with pingyangmycin, a glycopeptide antibiotic belonging to the bleomycin family, as monotherapy and in combination with surgical resection. The authors concluded that sclerotherapy with pingyangmycin was effective in greater than two-thirds of patients but the best outcomes came from the combination sclerotherapy and surgery group, with 73% reporting “near normal” appearance. 41 Alcoholic solution of zein (Ethinbloc) is effective in the treatment of macrocystic and mixed malformations in various anatomic locations. 42 In a study of 63 patients, nearly 50% of patients with macrocystic lesions reported excellent results, compared with 23% of microcystic lesions, and only five patients required surgery for complications related to sclerotherapy. 43
Laser and radiofrequency ablation
Laser therapy is appropriate for superficial microcytic LMs and large LMs not amenable to surgical intervention. Benefits include preservation of tissue and function, reduction of tissue volume, short duration of procedure (less than 30 minutes), and ability to repeat the procedure for desired effects. 44 Systematic review of 28 patients with superficial microcytic LMs showed resolution in eight patients at 3-year follow-up, with the only reported side effects being discoloration and scarring. 45
Radiofrequency ablation (RFA) is indicated for microcystic lesions and involves destruction of diseased tissues at low temperatures with minimal damage to surrounding tissue. The RFA has been shown to decrease the severity and frequency of complications 46 and is well tolerated by the pediatric population. 47
Surgical management
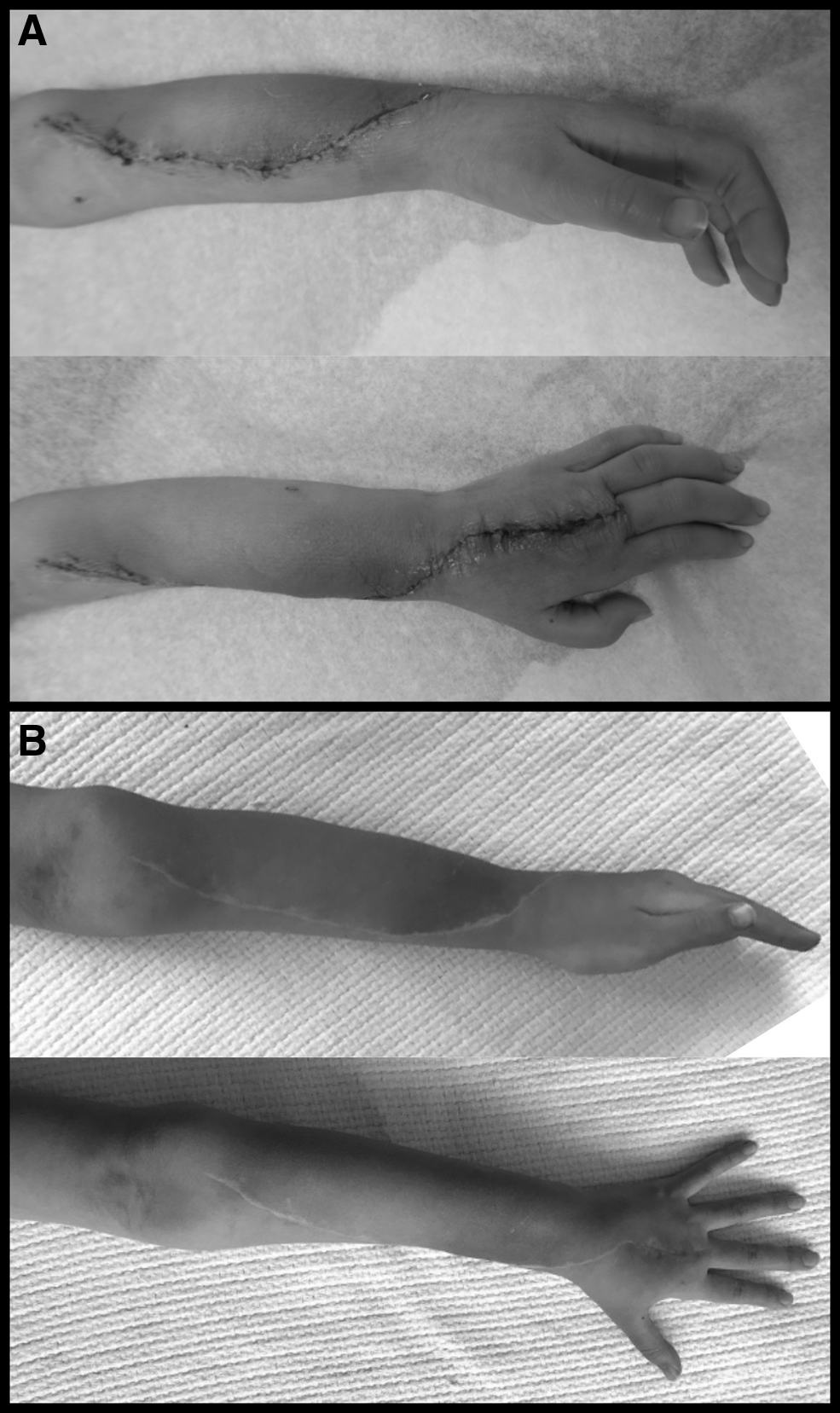
Surgical resection is reserved for isolated and accessible LMs with clear boundaries, in cases of extensive disease, or when nonsurgical therapy provides inadequate results. The decision to pursue complete or partial excision is largely influenced by the goals of surgery, size, anatomic location, characteristics, and extent of infiltration. Generally, mixed and microcystic lesions are more difficult to resect given their infiltrative nature and disregard for anatomical planes. Partial excision may be adequate to improve function, cosmesis, and decrease complications. Complete excision is effective but may be aesthetically unfavorable. 48 Complications such as nerve injury have been reported in 45% of patients undergoing surgical excision of cervicofacial LMs. 38 Other postoperative complications include wound infection, bleeding, and lymph leak. Recurrence rate can be as high as 20%, and persistent disease after resection is ∼30%23,24 likely due to the inability to distinguish borders of microcystic lesions. Figures 7 through 9 show preoperative and postoperative photos of an LM of the upper extremity that was successfully resected.

Intraoperative photos of a left upper extremity mixed micro and macrocystic malformation.

Immediate postoperative photos after single-stage wide excision of LM of the left hand and forearm.
Conclusion
The LMs are rare and variable in presentation. A multidisciplinary approach is necessary to effectively diagnose and manage these patients. Departing from historically descriptive terminology, such a “cystic hygroma,” LMs are now categorized as macro, micro, or mixed cystic lesions based on size. Advances in imaging modalities allow for early diagnosis and more accurate characterization of the lesions. Treatment of LMs can pose a significant challenge to the clinician and should be selected based on LM morphology. New discoveries in the molecular biology of LMs have provided treatment targets and established a role for pharmacotherapy. Although sclerotherapy is an effective and minimally invasive treatment option for LMs, surgical excision still has a role in the treatment of focal lesions. In larger lesions, surgical excision and reconstruction may need to be staged for optimal aesthetic and functional outcomes, 48 and a combination of medical and surgical treatment often provides the best results.
Authorship Confirmation Statement
All people who meet authorship criteria are listed as authors, and all authors certify that they have participated sufficiently in the work to take public responsibility for the content, including participation in the concept, design, analysis, writing, or revision of the article. All people who have made substantial contributions to the work reported in the article but who do not meet the criteria for authorship are named in the Acknowledgements and have given their written permission to be named.
Footnotes
Acknowledgments
The authors are grateful to Naomi Basaca for her participation in their article. Her dedication to the advocacy and education of both patients and physicians is inspiring. The authors are also grateful to John Kauffman, MD, Alison Small, MD, and Melinda Wu, MD for providing images and expertise.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.