
Abstract
Background:
Upper limb lymphedema may be revealed after breast cancer and its treatment. Among different treatment approaches, intermittent pneumatic compression (IPC) therapy and low-level laser therapy (LLLT) are reported as effective modalities in the treatment of postmastectomy upper limb lymphedema (PML). The aim of the current study is to investigate the long-term effectiveness of combined IPC plus LLLT versus IPC therapy alone in patients with PML.
Methods and Results:
The patients were allocated into two groups in this single-blinded, controlled clinical trial. Group I received combined treatment with IPC plus LLLT (n = 21) and group II received only IPC (n = 21). IPC treatment was given 5 sessions per week for 4 weeks (20 sessions). LLLT was also performed 5 sessions per week for 4 weeks (20 sessions). Clinical evaluations were performed before and after the treatment at the 3, 6, and 12-month follow-up visits. According to within-group analysis, statistically significant improvements in the circumference difference (Cdiff) and grip strength were observed in both groups (for Cdiff, p = 0.018 and p = 0.032, respectively; for grip strength, p = 0.001 and p = 0.046, respectively). Visual analog scale values for arm pain and shoulder pain during motion were decreased only in group I.
Conclusion:
Both interventions have positive effects on lymphedema, grip strength, and pain. Long-term effects of combined therapy, especially on pain, are slightly superior to the pneumatic compression alone.
Introduction
Breast cancer is one of the most common types of malignancies in women across the world. Advances in diagnosis and treatment of breast cancer in recent decades have resulted in prolonged survival rates but also yielded some disturbing complications, including secondary arm lymphedema due to cancer-related treatments (surgery and/or radiation therapy). Lymphedema is generally defined as the accumulation of protein-rich interstitial fluid as a result of impaired lymphatic function. Breast cancer-related lymphedema might result from surgical removal of lymph nodes and lymphatic pathways. In addition, soft tissue fibrosis following inflammation, infection, or radiation and chemotherapy may lead to further damage to lymphatic system. Postmastectomy upper limb lymphedema (PML) incidence ranges from 24% to 49% in this group of patients and may occur with minimal or no damage to axillary lymph nodes.1–3
Patients with PML generally experience a variety of problems, including discomfort, heaviness, decreased muscle strength and function, fatigue, and neuropathic pain in the affected arm as well as psychological distress and depression. Increased survival rates of breast cancer patients that is reported is more than 90% in conjunction with the higher incidence of secondary arm lymphedema, and other musculoskeletal complications substantially impact the physical function and affects the quality of life. Additionally, arm lymphedema alone was found to increase overall health care utilization by 30% up to 10 years after the completion of breast cancer treatment.4,5 So, it is essential to start the PML treatment earlier.
Currently, the gold standard treatment for PML is complex decongestive therapy, which is composed of manual lymphatic drainage, daily bandaging, skin care, exercise, and use of compression garments.5–8 It is suggested that treatment modalities that are predominantly administered by health professionals, such as complex decongestive physical therapy, manual lymphatic drainage, laser therapy and pneumatic pump therapy generally yield considerable volume reductions. Pneumatic compression therapy causes the drainage of retained fluid from interstitial zone into the lymphatic vessels by producing a pressure gradient. Low-level laser therapy (LLLT) is reported as an agent which has some positive effects on PML by diminishing surgical scars, reducing the amount of high tissue protein and fluid, encouraging lymphangiogenesis, stimulating lymphatic activity, and stimulating macrophage cells as well as immune system.9–11
Although it has widespread use in clinical settings, there are limited number of studies on pneumatic compression therapy in the treatment of PML, thereby the evidence is poor.9,10,12,13 In contrast, there is a growing number of studies related to LLLT for the treatment of PML.9,11,14–20 LLLT is reported as promising option for the treatment of PML that has moderate-to-strong evidence by the means of effectiveness.20–23
There is only one study in the literature comparing the effects of LLLT and pneumatic compression therapy in patients with PML, 9 but no data were found in the literature evaluating the combined treatment of these modalities in this group of patients. We aimed to compare the short- and long-term effectiveness of combined intermittent pneumatic compression (IPC) plus LLLT versus IPC therapy alone in patients with PML in the current prospective controlled clinical trial.
Materials and Methods
Study population
The study included patients with arm lymphedema who had undergone to modified radical mastectomy with complete axillary dissection and patients who had lymphedema at least for 3 months. Exclusion criteria were as follows: patients who had (i) metastases, (ii) ongoing radiotherapy and/or chemotherapy, (iii) infection such as cellulitis or thrombophlebitis, (iv) venous thrombosis, (v) chronic inflammatory diseases, (vi) severe trauma, (vii) limitation of the range of motion at involved upper extremity joints, (viii) patients who used medications that have impact on body fluid and electrolyte balance, and (ix) patients who had undergone any physical therapy program other than skin care and home exercises directed to the affected arm within the previous 6 months.
Study design and protocol
The current study was a single-blinded, controlled clinical trial. The study was conducted at the Department of Physical Medicine and Rehabilitation in Cukurova University Faculty of Medicine. The study protocol was approved by the Local Ethics Committee of Çukurova University (03/2011-12). Written informed consent was taken from each participant. Also, the current study was conducted in accordance with the principles of the Declaration of Helsinki.
Demographic and clinical evaluation
Demographic characteristics of the study population, including age, education and occupation, duration of lymphedema, date of operation, number of chemotherapy cycles, and radiotherapy period were documented. Symptoms, including the sensations of heaviness, tightness, weakness, paresthesia, and burning, were recorded.
Patients' grip strength was measured by using portable hydraulic dynamometer (Jamar; Sammods Preston, Bolingbrook, IL) and results were documented as kilogram. Measurements were done when patients were seated with the shoulder adducted, elbow flexed at 90°, and forearm in neutral rotation. Three consecutive measurements with 15-second rest intervals were taken and the mean values were recorded. 24
Modified Likert scale, ranging from “no improvement” to “very good improvement,” was used for evaluating global assessment of treatment satisfaction of the patients. Similarly, global assessment of the treatment satisfaction of the physician was also noted. 25 Shoulder pain at rest and during motion and also arm pain were evaluated by using visual analog scale (VAS) of 0–100 mm, ranging from “no pain” to “unbearable pain.” Range of motion degrees of the upper extremity joints were measured with goniometer when patients were in supine position. Symptoms, including the sensations of heaviness, tightness, weakness, paresthesia, and burning, were asked and noted as present or absent. The same physician performed all measurements and evaluations before and after the treatment, as well as at 3rd, 6th, and 12th months after treatment.
Lymphedema evaluation
Affected and unaffected upper limbs of the patients were measured by tape at seven anatomic sites, including axilla, 10 cm proximal and distal to the antecubital fossa, elbow, 5 cm proximal to the wrist, wrist, and mid palm. Lymphedema was described as the difference of more than 2 cm at minimum three out of the seven measured points. 9 The circumference difference (Cdiff) was defined as the difference between the sum of the circumferences of affected and unaffected upper extremities.9,11,26
Intervention
Patients were randomized into two study groups; group I: combined treatment with IPC plus LLLT and group II: IPC treatment alone. Active range of motion, elevation, and pumping exercises were prescribed as home exercises to patients in both groups during the treatment and follow-up periods. Patients were instructed to do these exercises twice daily. No other medical or rehabilitative treatment was allowed during the study period.
IPC treatment was applied with a device (MJS Healthcare Ltd., United Kingdom) generating a pressure of 60 mmHg that is generally recommended in the literature.9,10,27,28 Patients in both groups received 5 IPC treatment sessions per week for 4 weeks (a total of 20 sessions) and each session lasted 60 minutes. Patients in group I received additional laser treatment, with the dosage of 2800 Hz, 1.5 J/cm2 by using Ga-As 904 nm laser device (Electronica Pagani IR27/4). Five laser treatment sessions per week for 4 weeks (a total of 20 sessions) were performed. Each treatment session lasted 20 minutes. Laser was applied at three points on the antecubital fossa and at seven points on the axilla.
Statistical analysis
Statistical analysis was performed by using IBM SPSS version 20.0 (SPSS, Inc., Chicago, IL). Descriptive statistics was performed for analysis of demographic and clinical variables. Continuous variables of the study population were checked for normality using Shapiro–Wilk test. Nonparametric values were given as median and interquartile range. Between-group comparisons of baseline data and continuous variables were analyzed by Mann–Whitney U test. Categorical variables were analyzed by chi-square test. Within-group differences according to time course were performed by repeated measures ANOVA. The generalized estimating equations (GEE) was used to analyze the changes of patients' symptoms within and between groups. Multiple Linear Regression analysis was performed to determine the factors impacting on Cdiff and grip strength. The results were considered as statistically significant when p-values were <0.05.
Results
Seventy-two patients were assessed for eligibility. After applying the exclusion criteria 10 patients were omitted from the study. As a result, 62 patients were randomized into 2 groups. A total of 8 out of 62 patients were lost to follow-up and did not complete the study protocol. Seven patients in group I and five patients in group II did not attend the follow-up visits. Thereby, the results of 21 patients in each group were analyzed (Fig. 1). Median age of patients in group I and group II were 50.0 and 56.0 years, respectively. Demographic variables and baseline data of both groups are given in Table 1. There were no significant differences in these parameters between two groups.
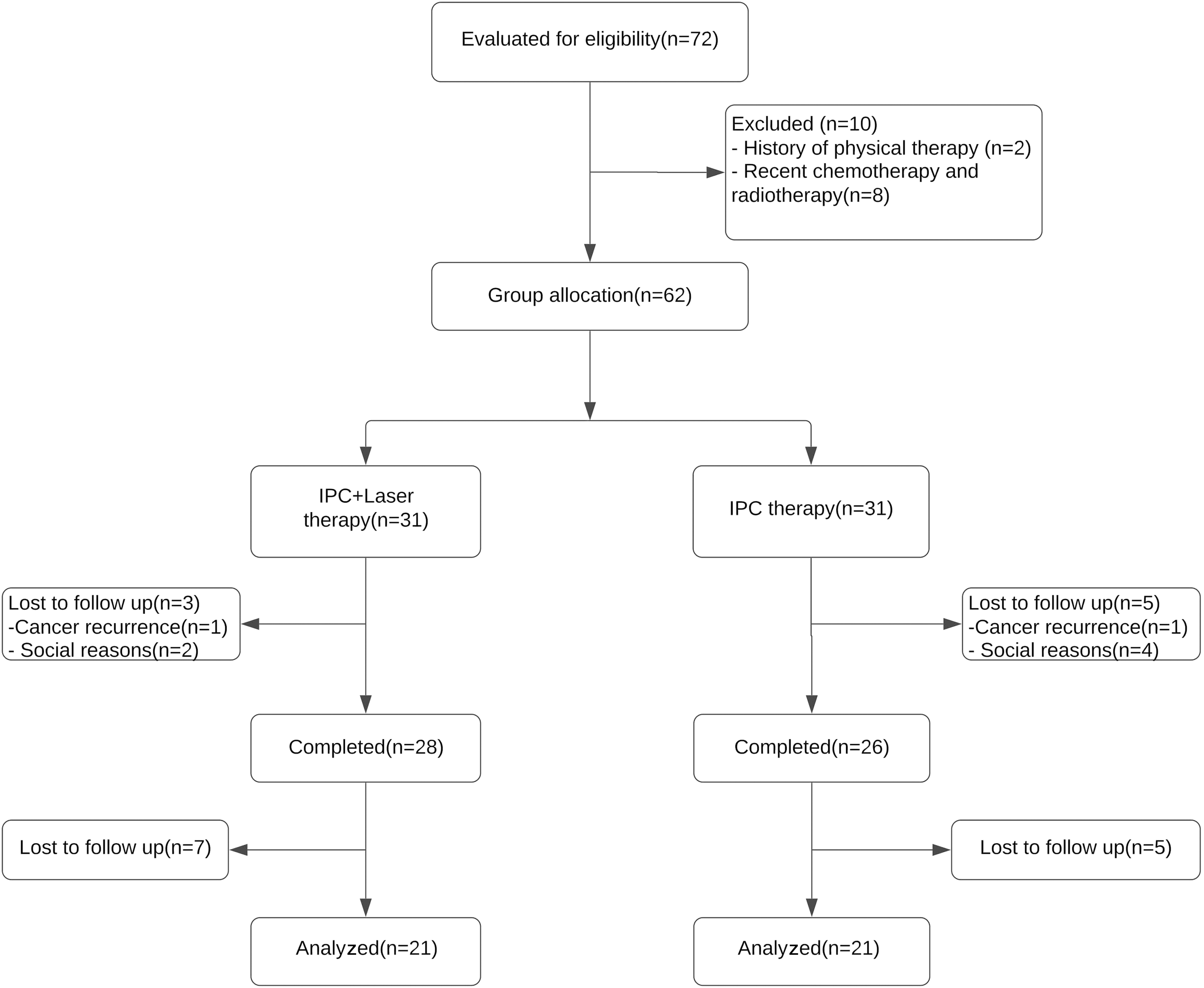
Flowchart of the study population.
Demographic Data of the Study Groups
Values are given as median and interquartile range (Q1–Q3). p-Value for the comparison of between-group, Mann–Whitney U test.
Cdiff values of the patients' in both groups, including pretreatment, posttreatment, and 3rd, 6th, and 12th months follow up visits are shown in Table 2. Within-group differences according to time course yielded statistically significant difference in both groups (p = 0.018 and p = 0.032, respectively). Further analysis revealed that the Cdiff values between pretreatment and posttreatment visits provided a statistically significant improvement within both group I and group II (p = 0.001 and p = 0.025, respectively). The improvement was found to be significant at 3rd months only in group I (p = 0.042), but no statistically significant improvements were found at 6th and 12th months in both groups (Fig. 2).
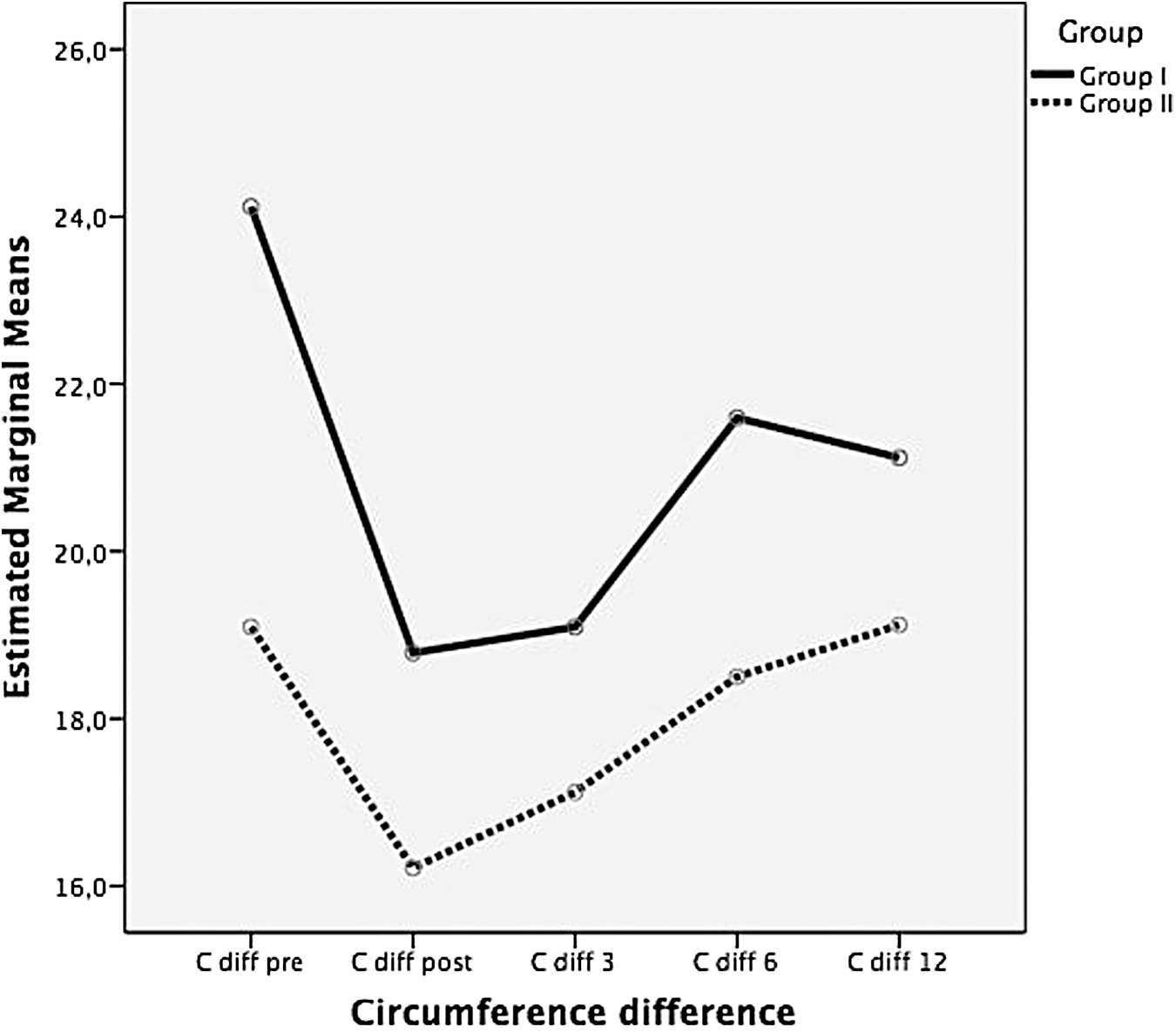
Circumference difference values of patients' according to time course.
The Comparison of Between-Group and Within-Group Values of the Circumference Difference (Cdiff) Grip Strength, and Visual Analog Scale
The bold values represent statistically significance.
Cdiff, difference between the sum of the circumferences of affected and unaffected upper extremities.
Values are given as median and interquartile range (Q1–Q3).
p, p-value for between-group comparisons, Mann–Whitney U test.
pt, p-value for comparisons of within-group differences over the time course, repeated measures ANOVA.
p < 0.05, pairwise comparison.
VAS, visual analog scale.
Within-group differences for grip strength according to time course yielded statistically significant difference in both groups (p = 0.001 and p = 0.046, respectively) (Table 2). Grip strength values of the patients demonstrated a statistically significant improvement in group I as compared with pretreatment and posttreatment visits (p = 0.001). However, there was no statistically significant difference between baseline and posttreatment values in group II (p = 0.747). Comparison of grip strength measurements between pretreatment and third month follow-up visits showed statistically significant increased values in both groups (p = 0.041 and p = 0.006, respectively). No statistically significant improvement was found at the 6th and 12th month visits in both groups (Fig. 3). Additionally, we did not find any variable affecting Cdiff and grip strength according to multiple linear regression analysis.
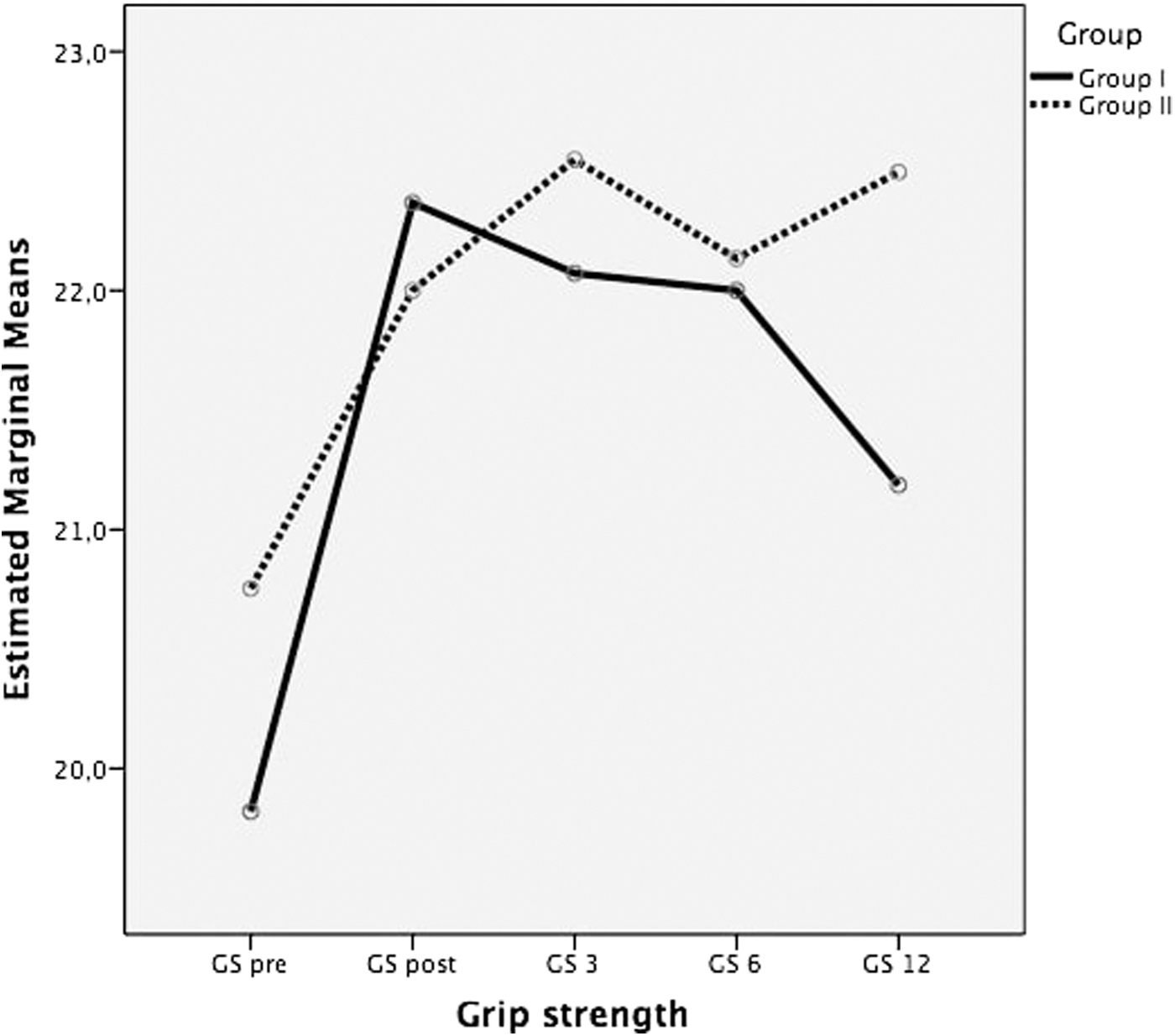
Grip strength values of patients' according to time course.
VAS evaluations of arm pain, shoulder pain at rest, and during motion were analyzed according to time course. Within-group analysis showed no difference in both groups for shoulder pain at rest. However, between-group analysis revealed that shoulder pain scores at rest were lower in group I compared with group II at the 6th and 12th months (p = 0.021 and p = 0.031, respectively). Within-group analysis of shoulder pain during motion and arm pain showed statistically significant difference only in group I (p = 0.001 and p = 0.022, respectively). Pain during motion decreased significantly when compared with pretreatment and posttreatment visits (p = 0.019), as well as follow-up visits (p = 0.038, p = 0.032, and p = 0.016 for the 3rd, 6th, and 12th month evaluations, respectively). There were no statistically significant differences regarding shoulder pain with motion and arm pain between group I and group II (Table 2 and Fig. 4).
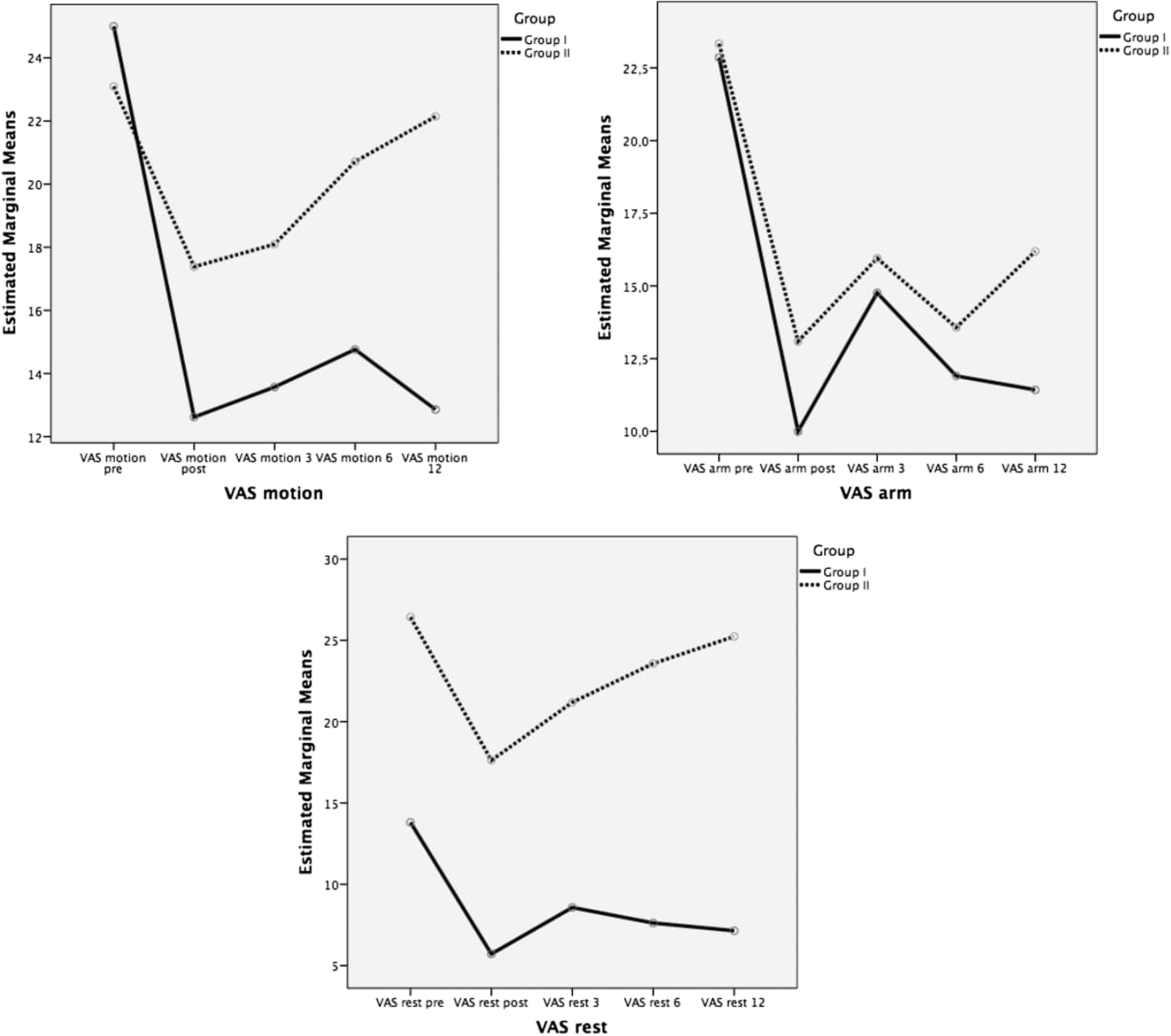
Visual analog scale values of shoulder pain at rest, during motion, and arm pain according to time course.
Scores of the global assessment of treatment satisfaction by the patients were not different between the two groups. Although statistical significance was not found, the satisfaction level of the patients was higher in group I compared with group II. When we compare the scores of global assessment of treatment satisfaction by the physician, percentage of the sum of patients with “no improvement” and “very mild improvement” was 33.3% in group I and 76.2% in group II.
GEE analysis showed that the symptom of weakness was significantly decreased at first and third months in both groups. While the symptom of weakness score was maintained as low in group I, it increased at 6th and 12th months in group II. Nevertheless, the follow-up values did not exceed the first value (p = 0.023) (Fig. 5). There were no statistically significant differences in the rest of the symptoms, including heaviness, tightness, and paresthesia.
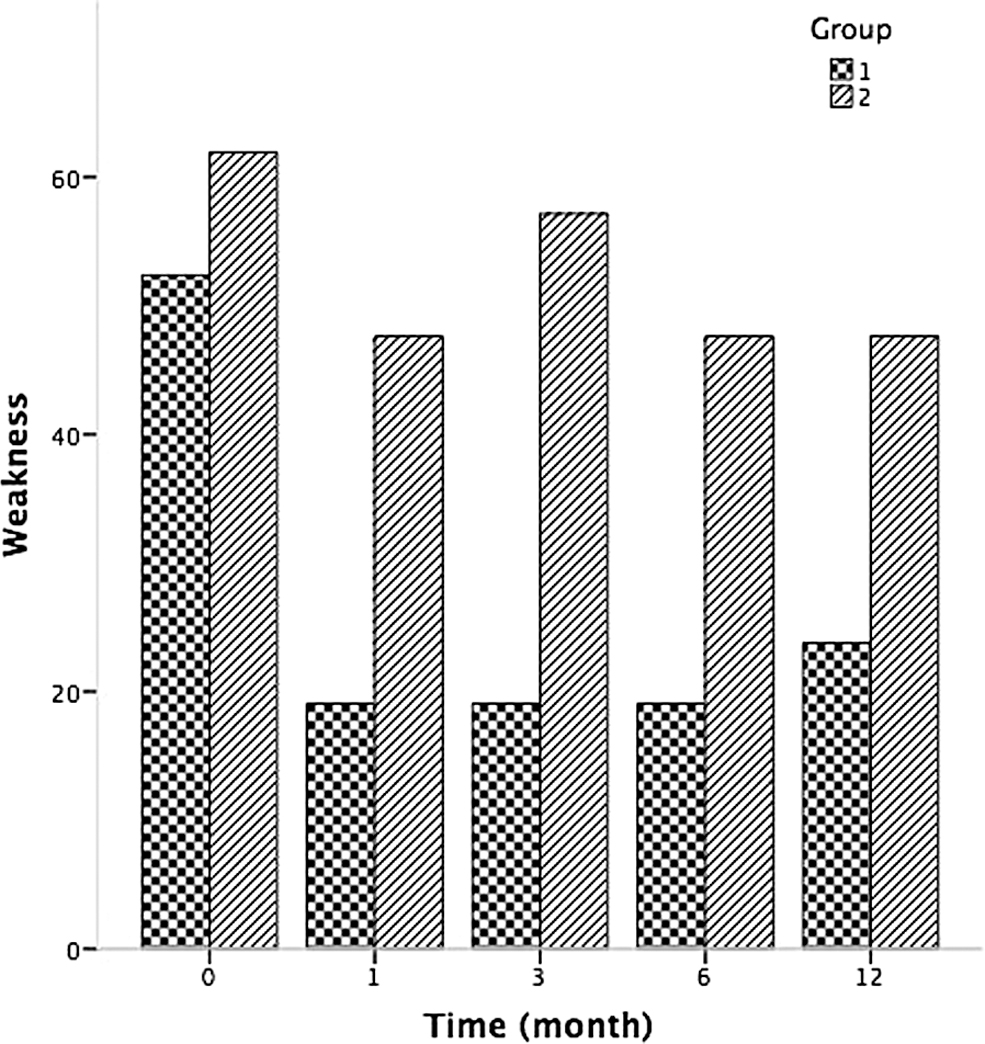
The change of weakness in groups over time. Group I: Combined treatment, group II: Intermittent pneumatic compression treatment.
Discussion
PML is a chronic condition, when untreated it worsens over time, and fluid retention, arm volume, and tissue fibrosis increase. PML cannot be completely cured, and require continuous treatment. The main goals of the management are volume reduction, maintenance of limb size, and prevention of disease progression. To achieve these goals, various physical therapeutic methods are used.9,29
We had previously conducted a study to compare the efficacy of pneumatic compression therapy and LLLT in the treatment of postmastectomy lymphedema and had found beneficial effects of both methods. 9 In the current study, we aimed to compare the long-term effectiveness of combined IPC plus LLLT versus IPC therapy alone, and tried to find whether an additional benefit of combined therapy in patients with PML.
There are a few studies in the literature evaluating the effects of pneumatic compression therapy in the treatment of PML. In a study by Dini et al., 80 patients with PML were randomized either to pneumatic compression or control groups. Patients in the treatment group received a pneumatic compression therapy of five sessions per week for 2 weeks repeated after a 5-week interval. Authors reported greater but not statistically significant reduction in arm circumference in the pneumatic compression group than in the control group. 12 Szuba et al. conducted a two-phase study evaluating the efficacy of pneumatic compression therapy in patients with PML. Authors compared decongestive lymphatic therapy alone and decongestive lymphatic therapy plus IPC therapy. Nineteen patients who continued application of pneumatic compression therapy for 6 months had greater volume reduction in their affected arm. 30
In our previous study, which consisted of the comparison of IPC therapy versus LLLT, we had observed significant reductions of arm circumference at 1st, 3rd, and 6th months but not in the 12th month in patients who had undergone 20 sessions for 4 weeks of pneumatic compression therapy, and we had suggested that pneumatic compression therapy is effective for the reduction of arm lymphedema but was not long lasting. 9 This may be due to the insufficiency of the total treatment period since Szuba et al. observed better results with 6 months application of pneumatic compression therapy. Recently, Tastaban et al. have performed a study and evaluated the effectiveness of complex decongestive treatment alone versus combined complex decongestive therapy and IPC therapy in 76 patients with PML. Authors reported significant excess volume reductions in both groups. Although the percentage excess volume reduction was better in combined treatment group, they found no statistically significant intergroup difference regarding the percentage reduction of excess volume. 13
Alongside the conventional treatment methods of PML, there are some alternative methods, which was mainly classified into the category of physical agent modalities acting through thermal, mechanical, or electromagnetic mechanisms. One of the popular agents, which has been used in the treatment of postmastectomy lymphedema was LLLT and it has been reported as “likely to be effective” for the treatment of this condition. 31 Besides the treatment of various musculoskeletal disorders, LLLT offers a novel option for this indication. Low-level laser has anti-inflammatory and antiedematous actions by reducing prostaglandin synthesis. It also increases lymph vessel diameter, vessel contractility, and lymphatic regeneration as well as the stimulation of phagocytic activity of neutrophils and monocytes. Other important mechanisms, which may be helpful for the reduction of lymphedema are improvement of wound healing, reduction of scar adhesion to underlying tissues, and diminution of the risk of skin infection through its immunostimulatory effect. 9
One of the first studies done by Piller and Thelander included 10 women with PML. Ten patients received 16 sessions of LLLT over 10 weeks and 7 patients followed for 36 months. Authors reported that edema volume was decreased; subjective symptoms, including aches/pains, tightness, heaviness, cramps, sensation of pins/needles, as well as the mobility of the affected arm were improved. Improvement continued until the sixth months. 26
In another study, patients received placebo or one or two cycles of LLLT to the axillary region of their affected arm. Although no significant improvement was reported immediately after any of the treatments, mean affected limb volume was significantly reduced at 1st and 3rd months of follow-up after two cycles of active laser treatment. Authors concluded that two cycles of laser treatment were effective in reducing the volume of the affected arm, extracellular fluid, and tissue hardness in nearly 33% of patients at 3 months after treatment. 11 In our previous study, we had compared the efficacy of pneumatic compression therapy and LLLT in 47 patients with postmastectomy lymphedema and had found significant volume reduction at 1st month as well as 3rd and 6th months follow-up in both groups of patients. Improvement was still significant at 12th months only in LLLT group. Also grip strength was improved in both groups, but the difference between groups was not significant. We had concluded that LLLT had better long-term results and might be a useful modality in the treatment of PML. 9
In the past decade, there are new studies regarding the use of LLLT in this group of patients. Dirican et al. studied short-term effects of LLLT in 17 patients who had PML. They used 2 cycles of LLLT, which consisted of 3 weeks and 9 sessions of application in each in addition to patients' ongoing therapeutic regimen, and found that 14 out of 17 patients had decreased pain with motion by an average 40% and 62.7% after the first and second cycles of LLLT, respectively. Patients also had 54% and 73% volume reduction in the affected arm after the first and second cycles of LLLT, respectively. Authors concluded that LLLT provided additional benefit when used in conjunction with the standard lymphedema treatment and two cycles of LLLT were found to be superior to one cycle of application. Authors suggested further studies evaluating the long-term effects of LLLT in combination with the conventional treatment methods. 19
In the current study, we tried to find out the long-term effects of combined LLLT and IPC therapy in patients with PML. Besides, Baxter et al. reported that, it was feasible to conduct a fully powered randomized controlled trial to test the effectiveness of the additional use of LLLT in the management of breast cancer-related PML. 14 Some other studies with LLLT demonstrated positive results on arm volume, shoulder pain, and mobility together with the improvement of hand grip strength in patients with PML.3,16–18 Kilmartin et al. reported a significant benefit of complementary LLLT for relieving symptoms and improvement of emotional distress but no significant reduction of limb volume in patients with PML. 15 Moderate-strength evidence was reported regarding the use of LLLT in patients with breast cancer-related lymphedema. Greater volume reductions were also reported with treatments consisting of LLLT than the treatments without it.23,32
Increasing clinical use of the LLLT had come into question of safety issue especially over the behavior of tumor cells. There is limited data on the effects of laser emissions on tumor cells. Cialdai et al. conducted an in vitro study on the safety of dual wavelength (808 and 905 nm) near-infrared laser therapy on breast adenocarcinoma cells and reported that, limited to the laser source, treatment conditions and experimental models used, laser radiation did not significantly affect the behavior of human breast adenocarcinoma cells, including their clonogenic efficiency. 31
Limitations of the current study were lack of sham group because of the ethical issues, relatively small number of patients because of long-term follow-up (1 year) as well as the difficulty to find patients who had met the inclusion criteria, and no blindness of patients because of the types of treatment modalities. Nevertheless, this is the first study evaluating the long-term effectiveness of combined pneumatic compression therapy and LLLT in patients with PML.
Conclusion
We have suggested that, both combined IPC and LLLT, and IPC therapy alone had positive effects on the reduction of arm volume, handgrip strength, and pain immediately after the therapy and in short-term period. It seems that long-term effects of combined therapy are slightly superior to IPC therapy alone especially on pain. Although the patient and physician satisfaction levels were better in combined therapy, no significant difference or superiority was found regarding the combined IPC therapy and LLLT over IPC therapy alone. Future studies are needed to assess the efficacy of combined treatment modalities in patients with PML.
Footnotes
Authors' Contributions
Study conception and design: E.K., N.G., and S.B.; Data collection: All authors; Data analysis and interpretation: E.K., N.G., and S.B.; Literature research: E.K., N.G., and S.B.; Writing first draft: E.K.; Revision of first draft: E.K., N.G., S.B., and S.P.; Supervision: All authors; Revision and approval of the final draft: All authors.
Author Disclosure Statement
No competing financial interest exists.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.