
Abstract
Background:
Lymphatic endothelial cells production or modification were closely related to the extracellular matrix (ECM) molecules. The serum hyaluronic acid (HA), laminin (LN), procollagen type III N-peptide (PIIINP), and collagen type IV (CGIV) levels were researched to explore the clinical significance of serum ECM proteins in the diagnosis and differentiation of lymphedema.
Methods:
Fifty-five patients were enrolled. They were divided into primary lymphedema (PLE), secondary lymphedema (SLE), and venous edema (VE) groups. Twenty-two healthy controls were also recruited as normal control (NC). Serum HA, LN, PIIINP, and CGIV levels of all subjects were assessed using chemiluminescence immunoassay. Statistical analysis and receiver operating characteristic (ROC) curves were used to data analysis.
Results:
The serum levels of CGIV were significantly decreased in both PLE and SLE groups compared with those in the NC group. Reduced serum CGIV levels were associated with the severity of lymphedema. The serum levels of CGIV and PIIINP were identified decreased in both PLE and SLE groups compared with those in the VE group. However, the levels of serum HA and LN were not observed significantly changed in both PLE and SLE groups than those in NC or VE group. Furthermore, ROC curve indicated that serum CGIV and PIIINP were capable of providing good diagnostic and differential diagnostic efficacy at the most appropriate cutoff point value.
Conclusion:
The serum levels of CGIV may have clinical significance in the diagnosis of lymphedema. CGIV and PIIINP may play a role in the differentiation of lymphedema from VE.
Introduction
Lymphedema was a chronic progressive disease with a condition of localized fluid accumulation and interstitial swelling. The disease was classified as primary lymphedema (PLE) and secondary lymphedema (SLE). PLE was due to lymphatic dysplasia. SLE resulted from trauma in the lymphatic system, which was most frequently observed after surgery and infections. 1 Limbs were the commonly affected body parts. Interstitial fibrosis and sclerosis accompanied by a large amount of collagen retention could be seen in limb lymphedema.
Current detection methods for limb lymphedema mainly rely on imaging examinations or interventional diagnosis, which are invasive or difficult to popularize. New methods based on serum biomarkers remain challenging. It was reported that the lymphatic endothelial cells (LECs) production or modification were closely related to the extracellular matrix (ECM) molecules. 2 For example, the hypoxia of LECs in lymphedema might alter some ECM protein and regulatory molecules, and thus contribute to fibrosis. 3
Hyaluronic acid (HA), laminin (LN), procollagen type III N-peptide (PIIINP), and collagen type IV (CGIV) were common ECM proteins. This study investigated the serum concentration of HA, LN, PIIINP, and CGIV in limb lymphedema patients and healthy controls to explore the clinical significance of these serum ECM proteins in the diagnosis of lymphedema.
In addition, swelling was the main symptom of limb lymphedema, which also presented in other diseases. Venous edema (VE) caused by valve insufficiency or thrombosis also manifested clinically as limb swelling. The two diseases were easily confused in clinical differentiation. So in the study, the serum levels of HA, LN, PIIINP, and CGIV between lymphedema and VE patients were also analyzed and compared to find whether they can provide a reference for the differentiation of lymphedema and VE.
Materials and Methods
Subjects
This clinical study was approved by the Ethics Committee of the Beijing Shijitan hospital, Capital Medical University. From January 2020 to July 2021, patients with a clinically definite diagnosis of PLE, SLE, and VE caused by valve insufficiency or thrombosis in Shijitan hospital were allocated to each of groups. All the lesions of the patients were located in the upper or lower limbs. There was no obvious chylous reflux in all cases. During the same period, healthy subjects who took part in a physical examination in the same hospital were randomly selected as normal control (NC). The serum levels of the indicators, including alanine transaminase, aspartate transaminase, γ-glutamyl transpeptidase, creatinine, white blood cell, red blood cell and hemoglobin, were no significant differences among the four groups. The detailed materials of these subjects are presented in Table 1.
Subjects Materials Among Primary Lymphedema, Secondary Lymphedema, Venous Edema, and Normal Control Groups
Z values and p values were derived from comparisons among the PLE, SLE, VE, and NC groups.
ALT, alanine transaminase; AST, aspartate transaminase; Cr, creatinine; GGT, γ-glutamyl transpeptadase; HGB, hemoglobin; NC, normal control; PLE, primary lymphedema; RBC, red blood cell; SLE, secondary lymphedema; VE, venous edema; WBC, white blood cell.
Patients with SLE had cervical cancer, endometrial cancer, liposarcoma, bladder cancer, breast cancer, and other cancers. They had received tumor surgery, radiotherapy, or chemotherapy for >5 years. There was no sign of tumor recurrence when they were enrolled. All patients with VE were due to venous valve insufficiency or venous thrombosis. Subjects with acute and chronic diseases such as liver disease, heart and kidney dysfunction, pulmonary fibrosis, diabetes, and pregnancy status were excluded.
To further observe the difference of ECM protein in patients with different degrees of lymphedema, patients with limb lymphedema, including PLE and SLE, were divided into three groups according to the excess volume increase of affected limb compared with the healthy limb. The three groups are assessed as minimal (<20% increase in limb volume), moderate (20%–40% increase), and severe (>40% increase) groups. 4 The detailed materials of these subjects are presented in Table 2.
Subjects Materials Among the Minimal, Moderate, and Severe Groups
Z values and p values were derived from comparisons among the minimal, moderate, and severe groups.
p < 0.05 was accepted as statistically significant difference.
CGIV, collagen type IV.
Serum
The whole blood samples of the subjects recruited were taken in serum separation tubes containing coagulant. After the blood was completely coagulated, they were centrifuged at 3500 rpm for 10 minutes and the supernatants were collected. Then the supernatants were stored in a refrigerator at −80°C.
Analyses
The levels of HA, LN, PIIINP, and CGIV in serum were assayed using chemiluminescence immunoassay in the automatic chemiluminescence analyzer. The analyzer was MAGLUMI 2000 Plus system (Snibe, Biotechnology Co., Ltd., China) employing proprietary reagents. The detection principle of HA was competition method, and the other items were the sandwich method. For data analyses, first, the detection values of the indexes among the PLE, SLE, VE groups and NC groups were compared and analyzed. Second, the indexes with statistical difference between the lymphedema and the healthy were selected and its differences among the minimal, moderate, and severe groups were compared. Third, receiver operating characteristic (ROC) curves were used to evaluate the diagnostic and differential diagnosis ability of some indicators.
Statistical analysis
Statistical analysis was done by the SPSS 25.0. Kruskal–Wallis tests were used to analyze the difference in detection values of HA, LN, CGIV, and PIIINP among different groups. ROC curve was used for evaluating the area under the curve (AUC). p < 0.05 was accepted as statistically significant difference. Non-normally distributed data were represented by M (p25, p75).
Results
Detection data comparison
The detection levels of HA, LN, CGIV, and PIIINP were analyzed among PLE, SLE, VE, and NC groups. After statistical analysis, HA, CGIV, and PIIINP in serum had significant statistical differences among the four groups. There was no significant difference in LN among the four groups. The CGIV levels were lower in both PLE and SLE groups than those in VE or NC group (p < 0.05). PIIINP values were higher in VE group compared with the other three groups (p < 0.05). In addition, there was a significant difference in HA between VE group and NC group, but no significant difference was observed between PLE/SLE group and NC group. The detailed results are shown in Table 3. The different levels of CGIV and PIIINP among four groups are shown in Figure 1.
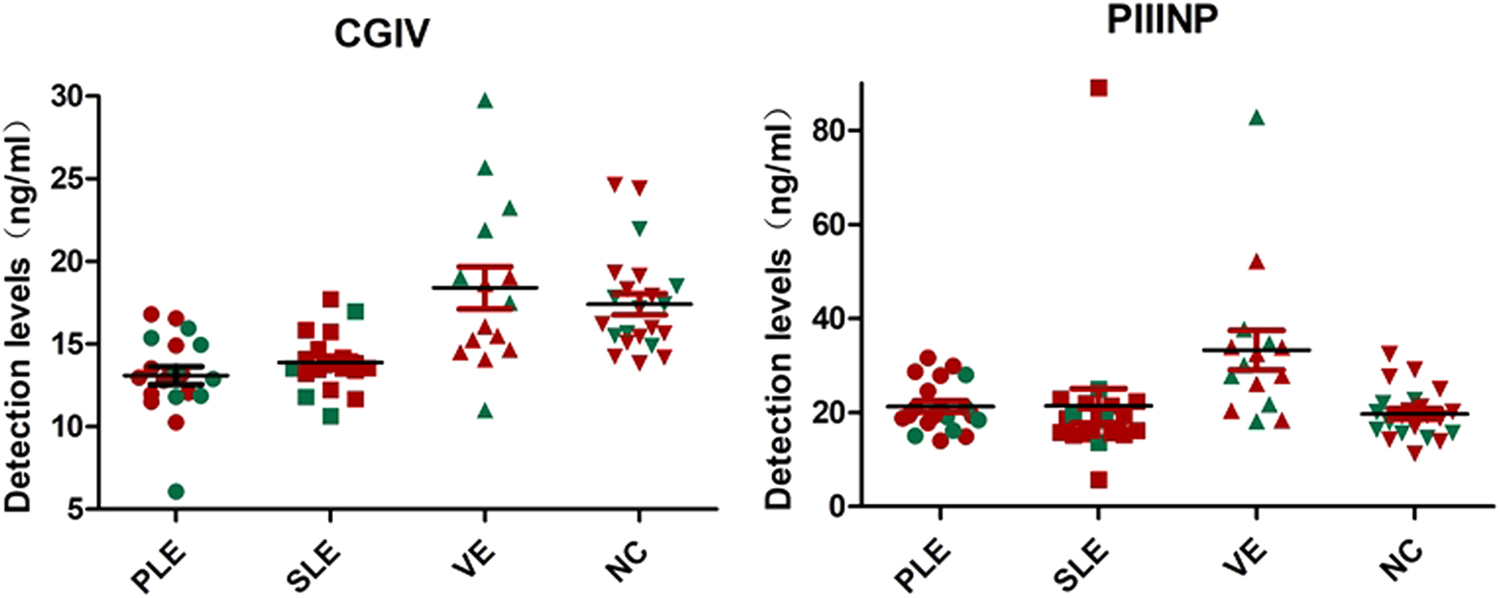
The different detection levels of CGIV, PIIINP among PLE, SLE, VE, and NC groups are shown in figure. Female patient data are marked red, and male patient data are marked green. CGIV, collagen type IV; NC, normal control; PIIINP, procollagen type III N-peptide; PLE, primary lymphedema; SLE, secondary lymphedema; VE, venous edema.
Comparison of the Values of Hyaluronic Acid, Laminin, Procollagen Type III N-Peptide, Collagen Type IV Among Primary Lymphedema, Secondary Lymphedema, Venous Edema, and Normal Control Groups
p < 0.05 was accepted as statistically significant difference. Z values and p values were derived from comparisons among the PLE, SLE, VE, and NC groups.
HA, hyaluronic acid; LN, laminin; PIIINP, procollagen type III N-peptide.
Through the aforementioned analysis, we found that CGIV was significantly lower in both PLE and SLE groups than those in VE or NC group (p < 0.05). For further identifying the correlation of CGIV levels and the severity of lymphedema, the detection values of CGIV among the minimal, moderate, and severe groups were analyzed. The CGIV levels were lower in severe group than that in minimal and moderate group (p < 0.05) (Table 2). No significant difference was found in the minimal and moderate groups. The different detection levels of CGIV among minimal, moderate, and severe groups are shown in Figure 2A. Figure 2B showed the correlation between the CGIV values and the increased volume of the affected limb.

The different detection levels of CGIV among minimal, moderate, and severe groups are shown in
Diagnostic value evaluation
To explore the diagnostic and differentially diagnostic power of the CGIV and PIIINP, ROC curves analysis were performed. The ROC curves, AUCs, the sensitivities, and specificities at the corresponding optimal cutoff values of the indicators are shown in Figures 3–5, respectively.

ROC curves of CGIV for diagnosis PLE/SLE. The cutoff value of indexes with sensitivity and specificity, as well as AUCs, are presented in a separate table. AUC, area under the ROC curve; CI, confidence interval; ROC, receiver operating characteristic.
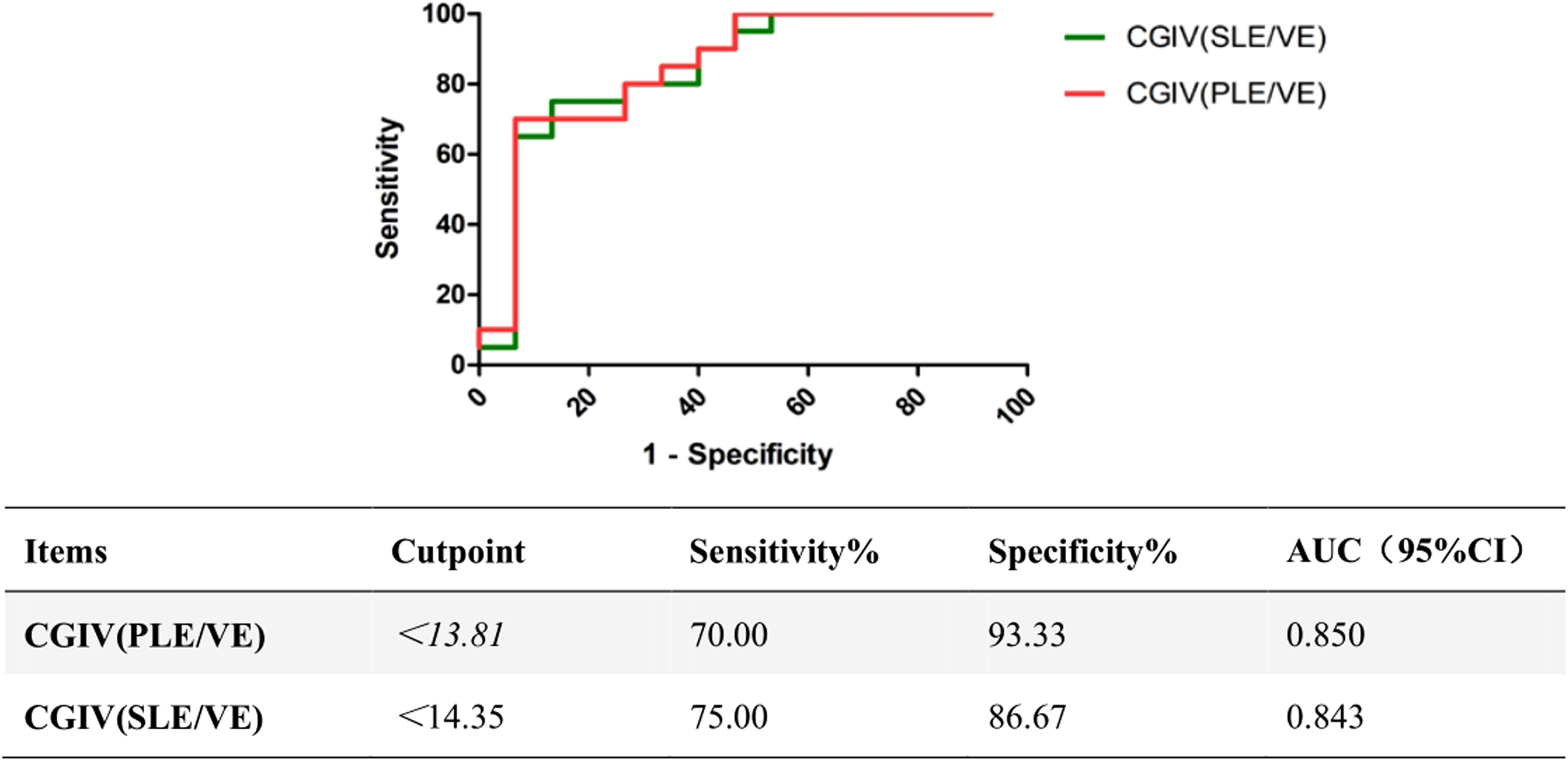
ROC curves of CGIV for differential diagnosis PLE/SLE and VE. The cutoff value of indexes with sensitivity and specificity, as well as AUCs, are presented in a separate table.
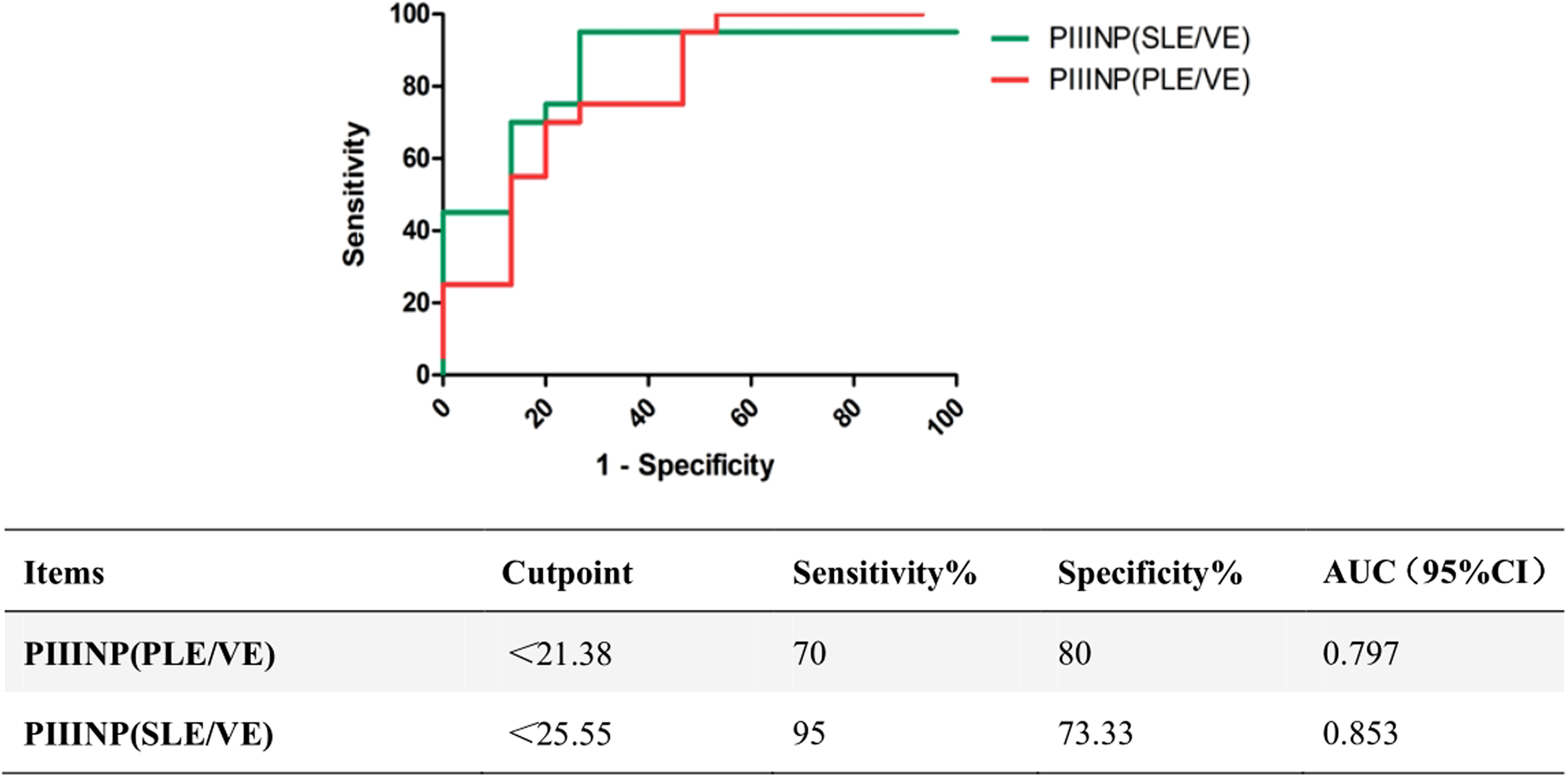
ROC curves of PIIINP for diagnosis differential diagnosis PLE/SLE and VE. The cutoff value of indexes with sensitivity and specificity, as well as AUCs, are presented in a separate table.
As shown in Figure 3, the AUCs of CGIV were 0.900 and 0.889 for patients with PLE and SLE, respectively. At the corresponding optimal cutoff values, the specificities and sensitivities of CGIV to predict PLE reached 100.00% and 70%, for SLE reached 86.36% and 80%, respectively. Then, to explore whether CGIV and PIIINP can distinguish PLE or SLE and VE caused by valve insufficiency or thrombosis, ROC curves analysis were also carried out.
For CGIV, as shown in Figure 4, the AUC was 0.850 for distinguishing PLE and VE caused by valve insufficiency or thrombosis with the 70% sensitivity and 93.3% specificity at the best threshold. The AUC was 0.843 for differentiating SLE and VE with the 75% sensitivity and 86.67% specificity at the best threshold. For PIIINP, as shown in Figure 5, the AUC was 0.797 for distinguishing PLE and VE caused by valve insufficiency or thrombosis with the 70% sensitivity and 80% specificity at the best threshold. The AUC was 0.853 for differentiating SLE and VE with the 95% sensitivity and 73.33% specificity at the best threshold.
Discussion
Lymphedema was swelling caused by lymphatic dysplasia and injury. The affected limbs thicken owing to accumulation of fluid, adipose, and fibrosis. The disease commonly was overlooked, thus resulting in loss of basic limb functions, long-term psychological burden, and bad quality of life. Tissue fibrosis and collagen accumulation were important features in lymphedema, which were characterized by hardening of the tissues with loss of elasticity. The purpose of this study was to explore the clinical value of serum ECM proteins in the diagnosis and differential diagnosis of lymphedema.
CG IV was a main component of the basement membrane that was widespread throughout tissues. Basement membranes could modulate multiple biological processes such as organogenesis, tissue repair, tumor metastasis, and angiogenesis. 5 It had long been recognized that upregulated serum CGIV levels were associated with the liver fibrosis.6,7 The study had reported that patients with interstitial lung disease showed significantly higher serum GCIV levels and it may reflect the disease progression. 8 Elevated serum CGIV levels also had been identified in systemic sclerosis and it may be a useful biomarker to assess the disease severity. 9
In this study, serum levels of CGIV in PLE and SLE groups were lower than those observed in healthy controls. Despite the presence of tissue fibrosis in lymphedema, the concentration of CGIV in serum did not increase, but decreased. Possible explanations were as follows: First, lymphatic vessels played an important role in scavenging proteins from the interstitium although bringing them back to the blood circulation. Owing to dysfunctional or obstructed lymphatic systems, lymphatic circulation was impeded and proteins were accumulated in the interstitium. 10 As an ECM protein, CGIV may deposit in the interstitial tissue of the limb, resulting in a decrease in the blood circulation.
Second, previous study reported that matrix metalloproteinases (MMP)-9 and MMP-2 mRNA were upregulated in lymphedema compared with controls. 11 MMP were zinc-dependent proteases mainly in charge of degradation of ECM components including the interstitial matrix and basement membrane. CGIV as an ECM protein could be degraded by MMP-9 and MMP-2,which belonged to MMP family. 12 In lymphedema, elevated MMP-9 and MMP-2 may lead to increased degradation of CGIV.
This study also found that the levels of serum CGIV in PLE and SLE groups were downregulated than those in VE group. Although the clinical manifestations of lymphedema and VE caused by valve insufficiency or thrombosis were similar, the pathological mechanisms of the two diseases were different. ROC curve analysis founded CGIV may serve as biomarker for differentiation lymphedema and VE.
PIIINP was an N-terminal peptide of type III procollagen. Its increased expression in pulmonary fibrosis was confirmed by animal models and patient studies.13,14 It had been proposed as a biomarker of liver fibrosis that related to the prognosis of patients. 15 Research also identified PIIINP level was elevated in systemic sclerosis, which could provide disease activity information. 16 We founded the level of serum PIIINP was not observed to have significant alteration in PLE and SLE groups than those in NC group, whereas upregulated in VE group.
This indicator may be a potential candidate as a differential diagnosis marker for lymphedema. The efficacy of differential diagnosis and the most appropriate cutoff point value were described in the study. Type III procollagen, as a major protein in blood vessel walls, was increased secretion in vascular wall injury. 17 In this study, whether the increase of serum PIIINP level in VE group was related to vascular wall injury caused by venous valve insufficiency or venous thrombosis need to be further explored.
Conclusion
In conclusion, we found that the concentration of CGIV decreased in the serum of patients with lymphedema, which related to the severity of the disease. The serum levels of CGIV may have clinical significance in the diagnosis of lymphedema. There was a significant difference in serum CGIV and PIIINP levels between lymphedema and VE valve insufficiency or thrombosis. CGIV and PIIINP may play a role in the differentiation of lymphedema from VE. In addition, a small sample was collected in the experiment. A follow-up test would expand the sample size and further verification of the results got in the study.
Footnotes
Acknowledgments
The authors thank the colleagues in the laboratory of Shijitan hospital for their support in the study.
Authors' Contributions
Professor Man Zhang was responsible for the experimental design and technical guidance. Dr. Qian Meng and Dr. Xue Zhang were responsible for the experimental detection, data analysis, and article writing. All authors read and approved the final article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The study was funded by Beijing Key Clinical Specialty Program (2020ZDZK2).