
Abstract
Background:
A previous study reported a new ultrasonography (US) measurement technique to evaluate the cross-sectional area (ΔCSA) of lymphedema in the upper extremity. This ΔCSA correlated well with parameters, such as the circumference, volumetry, and bioimpedance analysis (BIA) in healthy people and upper extremity lymphedema patients. This study examined whether a US measurement technique is clinically useful in patients with lymphedema in the lower extremity.
Methods and Results:
Forty patients diagnosed with unilateral lower extremity lymphedema were enrolled in this study. The subjects' leg circumference, BIA, isokinetic strength, and ΔCSA were examined on the same day. The leg circumference was measured at 15 cm above the knee (AK) and below the knee (BK) crease using a tape measure. BIA was performed by a trained physical therapist, and the data of impedance (Z) at 1 and 5 kHz of each side of the lower limbs and extracellular water (ECW) were used. A fully experienced physician measured soft tissue thickness, the distance between the skin and the fascia of the muscle, three times each at the anterior, medial, posterior, and lateral aspects of the bilateral legs by US at 15 cm AK and BK. The amount of soft tissue in the ΔCSA was calculated using the designed formula from the mean values of the thicknesses. Each parameter was calculated as the ratio of the sound side to the lesion side. The Pearson and Spearman correlation coefficients were used to assess the significance of these parameters. The ratio of ΔCSA measured at 15 cm AK and BK showed strong positive correlations with the circumference difference at the same level (rho = 0.790, p = 0.000, and rho = 0.882, p = 0.000, respectively). In addition, it showed moderate or strong correlations with the ratio of Z at 5 and 1 kHz in the BIA of the lower limbs (AK15, r = −0.511, p = 0.001 and r = −0.497, p = 0.001; BK15, r = −0.780, p = 0.000 and r = −0.756, p = 0.000, respectively). Although ECW and body mass index showed weak positive correlations with the ratio of ΔCSA measured at 15 cm BK, there was no significant correlation between the ratio of ΔCSA and the isokinetic muscle strength.
Conclusion:
The ΔCSA results showed moderate-to-strong correlations with other conveniently used methods except for the isokinetic muscle strength. As the US ΔCSA technique could measure lymphedema status with a structural consideration, it could also be recommended as a conventional measurement method in patients with upper and lower extremity lymphedema.
Introduction
Lymphedema is a chronic disease that results in a functional impairment. 1 Trauma, recurrent infections, and chronic venous insufficiency contribute to the development of lymphedema.2–5 Lymphedema of the lower extremities is also related to cancer-related therapeutics and chronic venous insufficiency.6–9 Regardless of the cause, early and accurate diagnosis is a key point to managing lymphedema of the lower extremities. A delayed diagnosis of the disease results in irreversible fibrotic changes to the soft tissue. 10
Several methods, such as tape measure, bioimpedance analysis (BIA), radionuclide lymphoscintigraphy, magnetic resonance lymphangiography, and indocyanine green lymphangiography, have been suggested to evaluate the exact status of lymphedema.11–44 A lymphedematous extremity is most commonly assessed in a clinic setting with a tape measure. 45 The common modality with imaging for diagnosis is indirect radionuclide lymphoscintigraphy, which requires an intradermal or subcutaneous injection of a radiolabeled tracer (99mTc-antimony sulfide colloid or 99mTc-labeled human serum albumin).1,46 Magnetic resonance imaging and computerized axial tomography have clinical utility with objective documentation of the structural changes by lymphedema.47,48 Bioelectric impedance spectroscopy analysis has been considered a cost-effective and reproducible method for evaluating patients suspected of lymphedema. The technique allows a noninvasive quantification of the extracellular fluid in the extremities. 49 Microarray-based transcriptomics of human skin has been developed to identify patients with lymphedema. Such multivariable biomarker panels should sensitively discriminate human lymphedema subjects from normal individuals. 50
Many studies have been published using various measurement tools in patients with upper extremity lymphedema.14–33
On the contrary, evaluating lower limb lymphedema is still challenging, and relatively few studies have been reported compared with those of upper limb lymphedema.12,34–44 Lymphedema and thicker skin of the lower extremity made it difficult to report detailed and good-quality studies owing to their less prevalence.
Ultrasonography (US) has many benefits, including convenience, painless, low economic burden, and no radiation exposure.51,52 A previous study reported a new US measurement technique to evaluate the cross-sectional area (US ΔCSA technique) of the lymphedema in healthy young female participants and patients with upper extremity lymphedema. In the first study, regarding healthy young participants, the intra- and interclass reliability of the measurements for all soft tissue areas was very strong. 53 Strong correlations were observed between ΔCSA, circumference, and volumetry for the above and below elbow-level measurements. 53 The strongest correlation coefficient was observed between volumetry and circumference measurements. 53
In a subsequent study, the method was also applied to patients with upper extremity lymphedema. 54 ΔCSA showed a strong positive correlation with circumference and a moderate negative correlation with Z at 5 Hz. The intra- and interclass coefficients of all US measurements were moderate to excellent. 54 These studies suggested that this new technique could measure the objective and special status of lymphedema in upper extremity lymphedema patients.53,54
There are no reports on the US technique in patients with lower extremity lymphedema. This study examined whether the US ΔCSA technique is also clinically useful in evaluating patients with lymphedema of lower extremities.
Materials and Methods
Subjects
Forty patients diagnosed with lower limb lymphedema, secondary to cancer surgery, and confirmed by clinical examinations and lymphoscintigraphy were recruited. This study included unilateral lower limb lymphedema patients whose circumference differences between the bilateral thighs and lower legs were >2 cm. The exclusion criteria of the participants were as follows: the presence of certain comorbidities requiring acute treatment (recent metastasis of cancer, active infection, such as acute dermatolymphangioadenitis in the affected limb; a history of trauma; primary lymphedema or lymphedema-unrelated cancer; or bilateral lymphedema). The subjects' leg circumference measurements in centimeters, BIA, Biodex, and US were performed on the same day. The stages of lymphedema were classified from 0 to 3 based on the consensus of the International Society of Lymphology in 2013. 55
This study was approved by the Pusan National University Yangsan Hospital Department of Health Institutional Review Board (IRB No. 05-2021-113).
Circumference measurements
The circumferences of both lower extremities were measured at 15 cm above the popliteal crease and below the popliteal crease. A tape measure was used, and care was taken not to apply unnecessary pressure to the leg during the measurement while maintaining a horizontal level. The differences of circumference between the sound and lesion side were collected for analysis.
US ΔCSA technique
A fully experienced physician measured both legs of each subject using a 7.5 MHz transducer (LOGIQ E9; General Electric, Boston, MA). The subjects were asked to lie on a table in the supine position. The physician marked the anterior (a), medial (b), posterior (c), and lateral (d) areas of the patients' legs corresponding to their anatomical sites, such as the rectus femoris, vastus medialis, hamstrings, and vastus lateralis, respectively, at 15 cm above the knee (AK), and the tibialis anterior, medial gastrocnemius, lateral gastrocnemius, and peroneus longus, respectively, at 15 cm below the knee (BK) to measure the desired cross section (Fig. 1). The probe was placed perpendicular to the targeted area with minimal pressure, and sufficient lubricant was applied to avoid contour distortion of the tissue under the transducer. The soft-tissue thickness was measured as the distance between the skin and fascia of the muscle in centimeters.
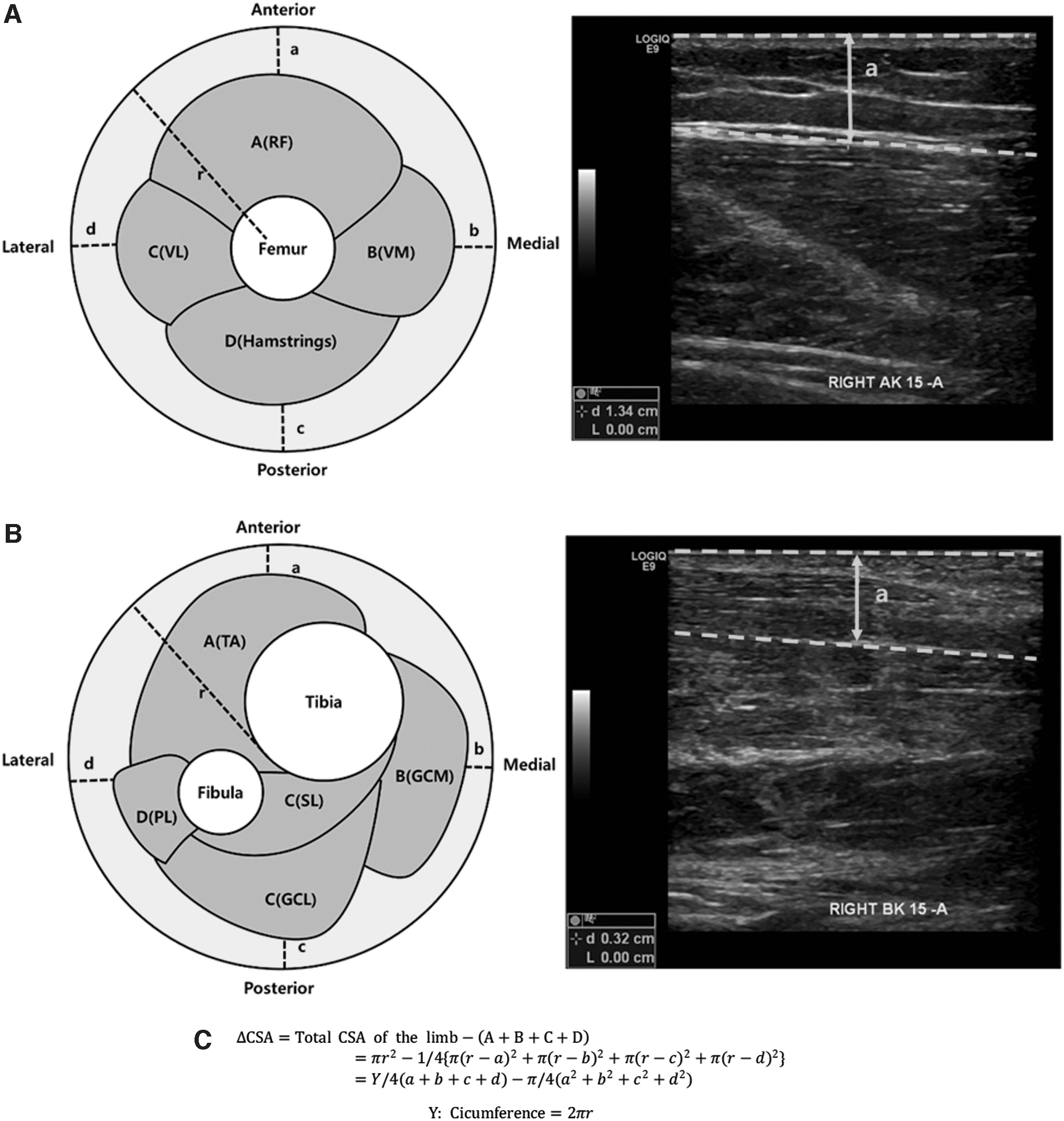
According to the contraction of each subject's muscles of the thigh or lower leg, the mobile structures were considered to be the muscle and fascia distinct from the muscle layers.
Sixteen areas from 15 cm AK and BK of bilateral lower extremities were examined in each participant. At each quadrant, the soft tissue thickness was measured (Fig. 1A—a–d, B—a–d), and the circumference was recorded (Y in Fig. 1C). The total ΔCSA (whole area in Fig. 1A, B) and radius (r in Fig. 1A, B) were determined using the measured circumference of the examined area. The imaginary inner area, consisting of deep structures, including bones and muscles (light red area in Fig. 1A, B), was calculated using the formula suggested in a previous study (Fig. 1C).53,54 The CSA (light yellow area in Fig. 1A, B) was calculated by subtracting the inner area from the total. Each ΔCSA was calculated as the ratio of the sound side to the lesion side.
Bioimpedance analysis
Single-frequency-BIA (InBody S10; Biospace, Seoul, Republic of Korea) was used. The patients were asked to lie on a nonconducting table in the supine position. All jewelry and conductive metal devices likely to affect electric currents were removed. The electrodes were attached to the bilateral wrists and ankles in a tetrapolar arrangement. Impedance (Z) at 1 and 5 kHz in each leg and extracellular water (ECW) were obtained to estimate the amount of extracellular fluid in both arms. The data were calculated as the ratio of the sound side to the lesion side.
Isokinetic muscle strength measurements
An isokinetic dynamometer (System 4 Pro™; Biodex Medical Systems, Inc., New York, USA) was used to measure the peak torque of the bilateral quadriceps and hamstring muscles, respectively. One experienced examiner measured all subjects. Data were calculated as the ratio of the sound side to the lesion side (Biodex ratio).
Data analysis
The continuous variables in this study, except for the biodex ratio of extension and flexion, had a normal distribution according to the Kolmogorov–Smirnov test. The correlations between ΔCSA and other measurements were evaluated using the Pearson's and Spearman's correlation coefficients among these parameters. Data analysis was conducted using SPSS (version 18.0; SPSS, Inc., Chicago, IL) statistical software. A p-value <0.05 was statistically significant.
Results
Demographic data
Five males and 35 females with lower extremity lymphedema participated in the study. The mean age, height, weight, duration, and body mass index (BMI) of the participants were 59.37 ± 10.50 years, 158.22 ± 6.82 cm, 64.16 ± 10.94 kg, 14.06 ± 8.31 months, and 25.03 ± 4.18 kg/m2, respectively (Table 1).
Demographics and Analyzed Data of the Subjects
Mean ± SD or n (%).
AK 15, at 15 cm above the knee; BK 15, at 15 cm below the knee; BIA, bioimpedance analysis; BMI, body mass index; ΔCSA, cross-sectional area; ECW, extracellular water; EXT, knee extension peak torque; FLX, knee flexion peak torque; Z, impedance.
The lesion side was the right in 17 (42.5%) and the left in 23 subjects (57.5%). The stage of the patients was 1 in 35 (87.5%) and 2 in 5 (12.5%); no subject had stage 0 or 3. The mean circumference difference at AK 15 cm was 3.27 ± 3.23 cm, and BK 15 cm was 2.09 ± 2.07 cm. The mean ΔCSA ratio at 15 cm AK was 1.34 ± 0.31 and 15 cm BK was 1.50 ± 0.57. The mean Z at 5 kHz was 0.78 ± 0.19; the mean Z at 1 kHz was 0.78 ± 0.19; the mean ECW was 0.39 ± 0.01; the mean Biodex ratio in extension and flexion was 1.03 ± 0.39 and 1.24 ± 0.91, respectively.
Correlation between ΔCSA and circumference differences
According to Evans' guide, the ratio of ΔCSA measured at 15 cm AK and BK showed strong positive correlations with the circumference differences at the same level (rho = 0.790, p = 0.000, and rho = 0.882, p = 0.000, respectively) (Table 2 and Fig. 2). 56

Correlation Between the Ratio of ΔCSA and Other Parameters
Statistically significant, difference means lesion – sound, ratio means lesion to sound.
Correlation between ΔCSA and BIA parameters
The ratio of ΔCSA measured at 15 cm AK showed moderate or strong correlations with the ratio of Z at 5 and 1 kHz in the BIA of the lower limbs (r = −0.511, p = 0.001; r = −0.497, p = 0.001, respectively). The ratio of ΔCSA measured at 15 cm BK showed strong correlations with the ratio of Z at 5 kHz and 1 kHz in the BIA of lower limbs (r = −0.780, p = 0.000; r = −0.756, p = 0.000, respectively). Weak correlations were observed between the ratio of ΔCSA measured at 15 cm BK and ECW (r = 0.321, p = 0.044) and between ECW and the ratio of ΔCSA measured at 15 cm BK but not at 15 cm AK.
Correlation between ΔCSA and BMI and isokinetic muscle strengths
A weak correlation was noted between the BMI and the ratio of ΔCSA measured at 15 cm BK (r = 0.319, p = 0.045) but not at 15 cm AK. There was no correlation between the ratio of ΔCSA measured at both 15 cm AK and BK and isokinetic muscle strength.
Discussion
Previous studies measured the degree of soft tissue thickness at 10 cm above and below the elbow in healthy young participants and upper extremity lymphedema patients using the newly invented ultrasonographic measurement technique.53,54 A strong correlation was noted between ΔCSA and other parameters, including the circumference in centimeters, volumetry, and BIA. This is a follow-up study, and this US technique could also measure lower extremity lymphedema precisely and objectively. As there have been few attempts to measure lower extremity lymphedema with US, this study could play a pioneering role in this field.
Compared with other methods, such as circumference tape measure or volumetry, this ΔCSA method could reflect the regional lymphedema value considering structural changes. Although the BIA can reflect the structural change of lymphedema, it does not show regional volume changes while reflecting the physiological status of the lymphedema indirectly. In this sense, ΔCSA is one of the ideal methods that show the specific regional structural change directly in patients with lymphedema.
In this study, the ratio of ΔCSA strongly correlated with circumference difference measurements using a tape measure. This means that the US ΔCSA technique could replace the tape measure, which is the most clinical tool. The ratio of ΔCSA at 15 cm AK showed a moderate correlation with the impedances at 1 and 5 kHz, but no correlation with the ECW. The ratio of ΔCSA at 15 cm BK showed a strong correlation with impedances at 1 and 5 kHz, and a weak correlation with ECW. The ratio of ΔCSA at 15 cm BK weakly correlated with the BMI but not with isokinetic strengths of the knee extensors or flexors. No correlation was observed between the ratio of ΔCSA at 15 cm AK and BMI or isokinetic strengths.
Unlike other values, no significant correlation was noted between the ratio of ΔCSA and the isokinetic value. According to previous studies, obesity was significantly related to the severity of lymphedema.57,58 Similarly, the lean body muscle mass was negatively correlated with obesity and possibly negatively correlated with the severity of lymphedema. Based on this point of view, this study hypothesized that muscle strength could be negatively correlated with the severity of lymphedema. Although there was a significant correlation between the ratio of ΔCSA at 15 cm BK and BMI, there was no significant correlation between ΔCSA and isokinetic muscle strengths in our study.
There could be several explanations. Compared with the average dominant knee extensor isokinetic strength at 60° per second (average range 94.32–104.11 Nm with age group 60–64 years), data of this study showed markedly low net values (69.14 ± 26.38 Nm). 59 The reason for the lower value is that lower limb lymphedema limits the activities of daily living, including walking, and may contribute to the general deconditioned state. In this sense, ΔCSA appears to be directly related to obesity or BMI but may not be correlated directly with the muscle strength in patients with lower extremity lymphedema.
This study had several limitations. First, there may have been selection bias regarding the severity of lymphedema. This is meaningful for the early detection of the disease because the study enrolled patients with mild disease. Patients with relatively severe lymphedema (stage 3) were not recruited. Thus, the application of the method requires further research, including stage 3 lymphedema, to increase its clinical utility in severe lymphedema. Thus, there was a weak correlation between ECW and ΔCSA 15 cm BK, which is the dependent part of body weight. If severer cases were recruited, even ΔCSA 15 cm AK correlations could also be observed in the future study.
Second, there was no sample whose leg subcutaneous layer thickness was beyond 4 cm in this study. A previous study reported that if the skin thickness is thicker than 4 cm, the thickness could not be measured precisely because of the resolution of US. If possible, a moderate degree of lymphedema or concomitant obesity people should be included in this US measurement technique.
Third, only the degree of lymphedema was measured at 15 cm AK and BK. Therefore, other areas, such as the dorsum of the foot, ankle, and proximal thigh, could be neglected. Atypical shaped edema or focal edema in the lower extremity was not detected using the US ΔCSA technique. This is a technical limitation of the method, and thorough history taking and physical examination are needed. In addition, hip and abdominal involvement could not be measured. Standardization for this limited area should also be determined in the following study.
Fourth, the distance value could be changed due to the subjective pressure. Although sufficient lubricant is applied to the skin to avoid contour distortion and cautious pressure is given to the patients, the value can vary according to the examiner.
Conclusion
ΔCSA measured using US showed moderate-to-strong correlations with other conveniently used methods in patients with lower extremity lymphedema. As the US ΔCSA technique appears to reflect the status of the lymphedema considering structural change precisely and objectively, it might be an effective measurement in patients with upper and lower extremity lymphedema.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.