
Abstract
Background:
Methods of conservative management for breast cancer-related lymphedema (BCRL) are burdensome in terms of time, cost, and convenience. In addition, many patients are not candidates for surgical treatment. Preliminary results have demonstrated possible beneficial effects of acupuncture for patients with BCRL. In this small pilot study, we examined the safety and feasibility of an acupuncture randomized control trial (RCT) in this patient cohort, utilizing a battery of standardized clinical and patient-centered outcome measures.
Methods and Results:
Patients with BCRL were randomized 2:1 to the acupuncture (n = 10) or the control (n = 4) group. Patients received acupuncture to the unaffected extremity biweekly for 6 weeks. Feasibility was defined as enrollment ≥80%, completion of ≥9 of 12 acupuncture sessions per person, and ≥75% completion of three of three measurement visits. To inform a future adequately powered RCT, we describe within-group changes in patient-centered outcomes, including circumferential measurements, bioimpedance spectroscopy, perometry, cytokine levels, and patient quality of life. Adverse events were systematically tracked. Fourteen patients completed the study. Of those who received acupuncture (n = 10), 8 completed all 12 acupuncture sessions, and 2 patients completed 11 sessions. Ninety-three percent of all participants completed all three measurement visits. There was no consistent improvement in arm volumes. Inflammatory marker levels had inconclusive fluctuations among both groups. All patients receiving acupuncture demonstrated an improvement in their functional quality-of-life score. No severe adverse events occurred.
Conclusions:
A randomized controlled study of acupuncture for BCRL is feasible. The acupuncture intervention is acceptable in this population, without safety concerns in a small sample and warrants further investigation.
Introduction
Breast cancer-related lymphedema (BCRL) is a potentially debilitating consequence of breast cancer treatment and has limited effective treatment options. Left untreated, BCRL can cause physical, psychosocial, and financial burdens for patients.1,2 In addition, upper extremity lymphedema may become progressive, ultimately affecting daily functioning and increasing risk for life-threatening infections.3,4 Conservative therapies exist; however, such regimens may be uncomfortable, are often time-consuming, and require life-long patient participation to prevent symptom progression. 5 Physiological and ablative surgical interventions for BCRL have gained recognition as interventions to alleviate lymphedema symptoms. However, such procedures are not widely accessible 6 and may not provide a definitive cure. 7 In addition, not all patients with BCRL are surgical candidates. Acupuncture has been proposed as an alternate strategy for the treatment of BCRL.8–10
Previous studies have suggested that acupuncture therapy is generally safe, with limited adverse effects, and with some reports of improvement in symptoms related to BCRL.11–14 Cassileth et al. 8 reported significant reductions in the arm circumferences of those who received acupuncture therapy for BCRL. Yao et al. 10 demonstrated that acupuncture treatment for lymphedema had favorable effects on limb size and shoulder range of motion. However, few existing studies have measured both subjective and objective outcomes, and simultaneously utilized multiple state-of-the art measures such as perometry and bioimpedance spectroscopy or explored underlying physiological changes. Moreover, although some early data have demonstrated benefits from acupuncture for BCRL, the mechanism of action is not well understood.
The goal of this pilot trial was to evaluate the feasibility of an acupuncture randomized control trial (RCT) for BCRL utilizing an expanded battery of objective measures of limb volumes, as well as lymphedema quality-of-life (LYMQOL) scores. To further explore the potential physiological basis underlying the preliminary reports of acupuncture efficacy for lymphedema, we measured changes in specific cytokines 4 before and after treatment to generate hypotheses and inform future study.
Materials and Methods
This proof-of-concept pilot trial was conducted at the Boston Lymphatic Center in coordination with the Cheng-Tsui Integrated Health Center and took place over the course of 19 months (IRB protocol No. 2017P-000433). Both centers are part of Beth Israel Deaconess Medical Center (BIDMC) in Boston, Massachusetts.
Recruitment, study population, and randomization
Patients with a diagnosis of unilateral BCRL were recruited at the Boston Lymphatic Center from April 2018 to November 2019. Patients met diagnostic criteria for BCRL if they presented with symptoms attributable to the disease as determined by a certified lymphedema therapist, and one objective measurement consistent with lymphedema: either an increase in L-Dex of 10 from the patient's preoperative baseline or a relative volume change of 10% or more.
Patients aged ≥18 years who chose to delay or decline lymphatic surgery, or those who were not surgical candidates were eligible to participate in the study. Patients with lymphedema affecting more than one extremity and/or symptoms lasting <6 months before evaluation were excluded. Similarly, patients who were <6 months from their surgical and chemoradiation treatment completion dates for breast cancer were excluded. Patients with clotting disorders (hemophilia, Von Willebrand disease), neutropenia (defined as ≤1500 neutrophils per μL), and spinal instability were also excluded from the study.
The initial target population size for the study was 21 individuals based on pragmatic considerations and a sample size adequate to demonstrate feasibility of study methods. Once written consent was obtained, eligible participants underwent 2:1 randomization to either a 6-week regimen of semiweekly acupuncture treatment (12 total sessions) or continued standard of care treatment without the addition of acupuncture. This randomization process involved a concealed and predesignated envelope system and the 2:1 randomization scheme allowed for increased experience with intervention delivery in the population.
Acupuncture intervention protocol
The study acupuncturist conducted acupuncture sessions twice weekly for 6 weeks (12 sessions total). A single board-certified acupuncturist from the Cheng-Tsui Center for Integrated Health administered all treatment sessions after training in a standardized acupuncture protocol. The standardized protocol involved 11 acupuncture points on the forehead, abdomen, unaffected (nonlymphedematous) extremity, and both lower extremities based on previously published studies. This protocol was intentionally designed to avoid needling affected limb to limit the potential infections and to ease participant's concern. Every study participant received the same standardized protocol at each session (Fig. 1).
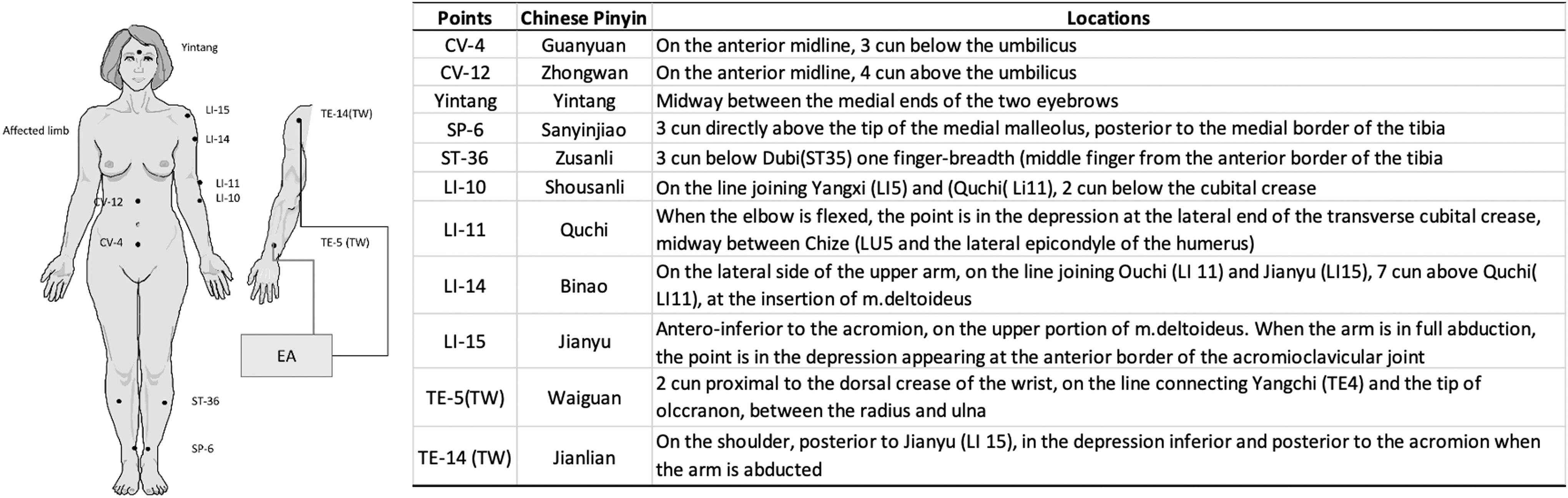
Acupuncture points on the unaffected extremity, torso, head, and lower extremities used for the treatment of breast cancer-related lymphedema.
Following acupuncture best safe practices, the skin was prepared with alcohol over the chosen acupuncture points. Acupuncture needles sizes 0.20 × −0.25 millimeters (mm) and 0.25 × 40 mm, Tai-Chi brand (Lhasa OMS, Inc., Weymouth, MA) were inserted at a depth of 5–15 mm except when applied on the forehead, where the depth was 2–5 mm. On the lower extremities, needles were manually manipulated to obtain De Qi, a sensation of mild heaviness or soreness, at a minimum of two points.
Electroacupuncture was administered to TE-5 (TW) and TE-14 (TW) on the unaffected arm. An infrared heat lamp was placed above the legs and needles remained in place for 30 minutes while the participant was left alone in the room with the lights dimmed. A call bell was made available, and the participant was asked to report any sensations of discomfort. Needles were manipulated before removal, although De Qi sensation was not required. Patients were systematically queried regarding adverse events after each acupuncture session, lymphedema measurement visit, and serology.
Outcome measurements
To assess feasibility, the total number of acupuncture sessions and testing visits completed by each patient were tracked using REDCap electronic data capture tools.15,16 Feasibility was defined as enrollment ≥80%, completion of ≥9 of 12 acupuncture sessions per person, and ≥75% of participants completing all three measurement visits.
All participants were scheduled for lymphedema measurement visits at enrollment, mid-study (at 3 weeks), and at the study completion (6 weeks). All participants were scheduled to undergo measurement visits after the 6th and 12th acupuncture treatment sessions. At each visit, circumferential measurements, bioimpedance spectroscopy (reported as L-Dex score), perometry, and LYMQOL scores were obtained. Cytokine quantification was performed only at enrollment, before starting acupuncture treatment, and after completion of acupuncture treatments (Table 1). An overview of outcomes and study timeline is represented in Table 1. In summary, all clinical lymphedema measurements, questionnaires, and blood tests were done at baseline and 6 weeks. Limb circumferential measures, bioimpedance spectroscopy, and perometry were additionally performed at 3 weeks
Overview of Study Timeline and Assessment of Outcomes
Primary outcome.
The primary clinical outcome was regional change in upper extremity extracellular fluid, evaluated with bioimpedance spectroscopy. An Impedimed L-Dex U400 Device (ImpediMed, Australia) was used to measure whole arm L-Dex scores, which were adjusted for limb dominance. Circumferential measurements of the upper extremities were obtained at every 4 cm along the arms, and volumes were calculated utilizing the truncated cone approximation. 17 Infrared optoelectronic volumetry, or perometry, was utilized as an additional marker of upper extremity volume change. In this technique, patients were in a sitting position with their arm abducted to 90° and the tip of their third finger touching the resting plate of the perometer. Whole arm measurements were taken for 53 mm, from the metacarpophalangeal joints to the axilla. A shadow was casted of the extremity in the horizontal and vertical directions every 3.1 mm. The diameter of the shadow was used to calculate the circumference and subsequent arm volume. 18 All values were entered by a designated member of the research staff in efforts to minimize potential physician or therapist bias.
A validated quality-of-life survey for lymphedema patients (LYMQOL) was administered to patients to assess patient-centered outcomes in four subdomains: appearance, symptoms, mood, and function. 19 To monitor for changes in systemic response, circulating cytokine levels were obtained through serological assessment. Plasma from these samples were assayed for interleukin-10 (IL-10), IL-4, and tissue necrosis factor beta (TNF-B), as these proteins correspond to inflammatory pathway stimulation and are hypothesized to play a role in lymphedema disease burden.4,20
Clinical measurements and administration of quality-of-life questionnaires were conducted by lymphedema physical therapists. Inflammatory cytokines were assayed by an internal laboratory group at BIDMC but independent from both the lymphatic center and the integrated health center. V-PLEX Plus Proinflammatory Panel 1 (Meso Scale Diagnostics, LLC, Rockville, MD) was used to assay levels of IL-10 and IL-4, and V-PLEX Plus Cytokine Panel 1 assay was used to measure levels of TNF-B. Descriptive analysis was performed using Microsoft Excel (2021; Microsoft, Redmond, WA) to evaluate recruitment and retention rates, patient characteristics, and objective changes in lymphedema symptoms.
Results
Seventeen patients were enrolled in the acupuncture study at the Boston Lymphatic Center between April 2018 and November 2019 (Fig. 2). Owing to the coronavirus 2019 pandemic, further enrollment was ceased, and the study ended before achieving the target sample size of 21. Given a target enrollment of 21 patients, the overall enrollment rate was 81%. Two patients withdrew before beginning the study. Fourteen of 15 patients completed the study. One participant withdrew early due to logistical issues involving transportation. All patients were female, with a median age at the time of study enrollment of 66 years (interquartile range [IQR] 57–70) and median body mass index (BMI) of 29 kg/m2 (IQR 25–31). Patient characteristics are presented in Table 2.
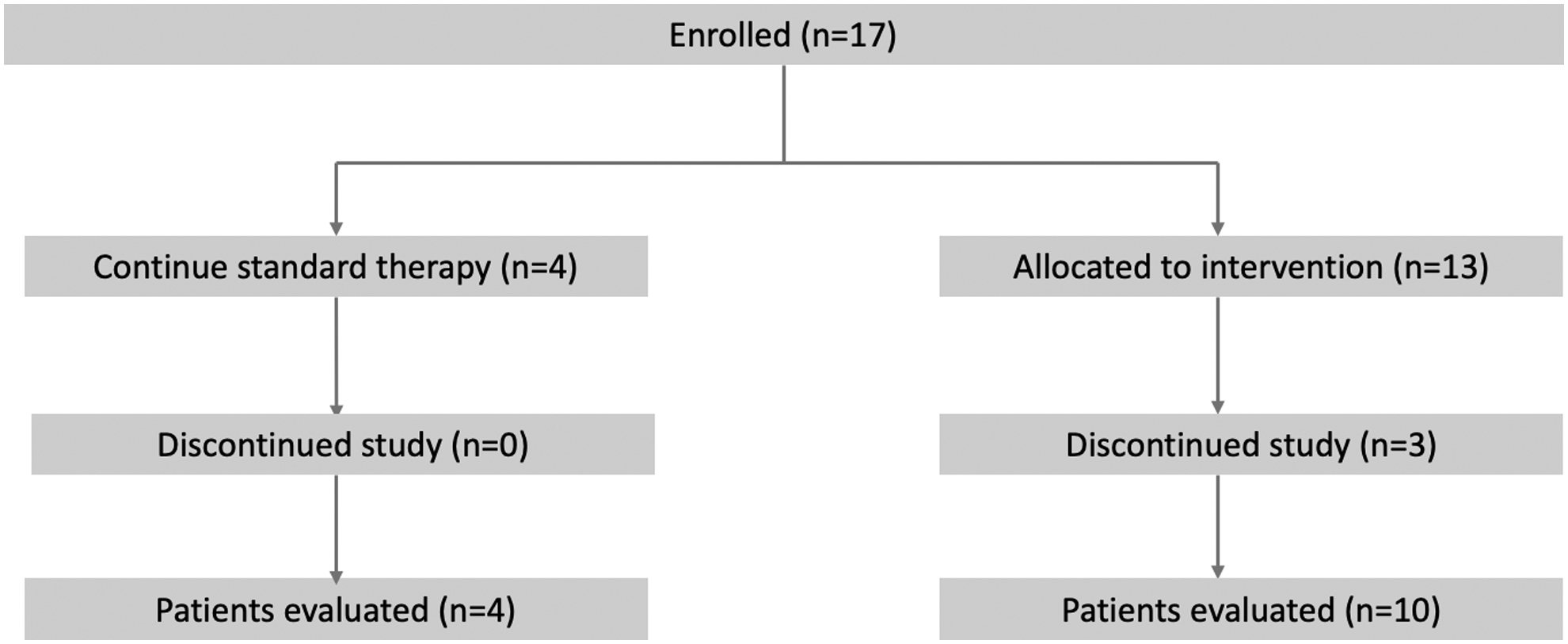
Consort diagram.
Patient Characteristics at the Time of Study Enrollment
BMI, body mass index; IQR, interquartile range.
A total of 118 acupuncture sessions were attended by 10 patients. Eighty percent of patients (n = 8) completed all 12 acupuncture sessions and 20% of patients (n = 2) completed 11 out of 12 visits. Of the 14 patients in the study, 13 (93%) completed all lymphedema measurement visits; 1 participant missed the week 3 measurement visit.
At the study initiation, the median L-DEX score was 46 in the acupuncture group and 27 in the control group. Over the course of the study, there were no consistent changes between the two groups in L-DEX scores, perometry, or limb volumes derived from circumferential measurements (Table 3). Changes in the inflammatory cytokines measured at the start and end of the study period are shown in Table 4. Levels of IL-10 appeared to be higher at end of treatment in the acupuncture group. IL-4 levels were undetectable in all samples and, therefore, were not included in the table.
Clinical Measures of Affected Arm Volumes at Enrollment, Week 3 (Mid-Study) and Week 6 (Study Completion) in Lymphedema Patients Receiving Acupuncture Treatment Versus Standard of Care
Presented as mean (standard deviation); median (quartile 1–quartile 3). Acute changes (pre- and post-treatment) were not being assessed.
Normal range is −10 to 10, Threshold for lymphedema diagnosis is ≥10. L-Dex measurements were adjusted for limb dominance; perometry and circumferential measurements were not adjusted for limb measurements.
Cytokine Levels in Plasma of Lymphedema Patients Obtained at the Start and End of 6 Weeks of Biweekly Acupuncture Treatment Versus Standard of Care
Data are presented as mean; median (range).
IL-10, interleukin 10; TNF-β, tissue necrosis factor beta.
Changes in LYMQOL subdomains are reported in Table 5. A higher score indicates that lymphedema has a greater adverse impact on a patient's quality of life. All patients who received acupuncture treatment reported an improvement in the functional subdomain of the LYMQOL survey. There were varying changes in the appearance, symptoms, and mood subdomains in both the acupuncture group and those who underwent standard treatment. One patient experienced transient bruising at their acupuncture sites, but no other adverse events were reported.
LYMQOL Survey Subdomain Scores at the Start and End of Acupuncture Treatment Versus Standard of Care
Presented as mean; median. A lower score indicated a higher quality of life.
Discussion
Acupuncture intervention for the treatment of BCRL was feasible in this cohort. No significant adverse events were reported.
Overall, the study terms of feasibility were met. The enrollment rate of the study was achieved despite early termination of recruitment efforts for this study due to the coronavirus 2019 (COVID-19) pandemic. Once enrolled, every participant completed at least 9 out of 12 of their scheduled acupuncture sessions, demonstrating adequate compliance with treatment. Despite a rigorous process of monitoring lymphedema symptoms every 3 weeks during the study period, ≥75% of participants completed all three measurement visits, which suggests that patients were generally able and willing to attend surveillance visits, despite requiring multiple methods of limb measurements during visits.
Our findings suggest the possible safety of a standardized acupuncture treatment protocol for lymphedema that did not involve needling the affected upper extremity. Occurrence of adverse events was low, and events were mild when present. Despite previous report of skin infections after acupuncture, 9 there were no reports of infection or other systemic responses, such as fever.
The multimodal objective measures to assess and quantitate symptoms of lymphedema were well-tolerated by patients. Patients could continue their standard therapies simultaneously while receiving acupuncture, allowing them to maintain symptomatic control during the duration of the study. Although we were not powered to detect any significant differences in patient-centered outcome measures, we observed that acupuncture treatment did not have an apparent negative impact on objective measures of lymphedema. Of note, despite randomization, the acupuncture group had more severe symptoms at baseline.
Lymphedema is characterized by a local inflammatory process with progression to fibrosis.4,21 Acupuncture has been suggested to play a role in the balance and regulation of cytokines, including IL-10, IL-4, and TNF-B in various settings of inflammation.22–25 We, therefore, hypothesize that acupuncture may have a similar immunomodulatory effect in the pathogenesis of lymphedema. Although we measured cytokines in this pilot feasibility study, we were underpowered to detect differences between groups.
We observed variable levels of IL-10 and TNF-B measured before and post-treatment and large interindividual variability, which could be related to sources of systemic inflammation independent from lymphedema. Further evaluation in a larger sample and more comprehensive analysis of biomarkers related to the pathophysiology of lymphatic dysfunction, including transforming growth factor beta (TGF-B) and leptin, could be included in future studies. 4 Overall, additional studies are needed to elucidate the possible physiological mechanism by which acupuncture may mitigate symptoms of lymphedema.
In within-group analyses, we observed that all patients who received acupuncture treatment showed improvements in the functional subdomain of their quality-of-life scores. The functional subdomain evaluates the extent to which lymphedema symptoms affect patient daily functioning, involving activities such as housework, occupation-related tasks, dressing oneself, eating, and writing. Results varied within the other subdomains, including appearance, symptoms, and mood. Changes in patient quality-of-life scores warrant further investigation.
This study has several limitations, and we note several lessons learned. Despite the prospective randomization, and perhaps reflective of the small sample size, the treatment and control groups were not well matched in their baseline objective measurements. This inequity hampers comparison of any volumetric responses with acupuncture across the two groups. Another limitation of this study is that we did not apply acupuncture needles to patients' affected (lymphedematous) extremities due to concern for infection from interruption of the cutaneous barrier, and it is unclear how this could potentially limit the effects of treatment. 26 One challenge we faced when using the LYMQOL survey was receiving incomplete surveys. Successful use of this questionnaire may require more specific instructions for completion or use of electronic forms.
Furthermore, the data from the IL-4 levels were discarded as they could not be quantified. This indicates a potential need to further refine our sample processing to ensure that cytokine levels are measured reliably. In addition, BCRL impacts males 27 and our cohort was 100% female, indicating a need to better evaluate the efficacy of this intervention in males with BCRL. Finally, by design, this pilot study was not powered to detect differences in objective and subjective outcomes, or trends in change over time. Although we initially aimed to recruit 21 participants, the COVID-19 pandemic limited our recruitment efforts. Nonetheless, our findings support the feasibility of this study.
Finally, the execution of this pilot trial relied heavily on close contact and physical proximity with the Cheng-Tsui Integrated Health Center. Our research team's relationship with the acupuncture team was critical for scheduling, coordination, and administration of acupuncture sessions.
Conclusions
In this small pilot feasibility study, we found that an RCT for acupuncture therapy for patients with BCRL was feasible and that acupuncture can be further studied for the conservative adjunctive management of lymphedema symptoms. Acupuncture may provide improvements in patients' quality of life, particularly in daily function. Future studies can evaluate objective measures for limb size and the underlying physiological mechanism warrant further investigation.
Footnotes
Acknowledgment
We would like to thank Jessica M. Butler for providing coordination of care and acupuncture for study participants.
Authors' Contributions
Data analysis, writing, and editing by R.F. Conceptualization, study design, methodology, and editing by A.R.J. Conceptualization, study design, methodology, formal analysis, and editing by K.S. Conceptualization, study design, formal analysis, and editing by A.F. Methodology and analysis by C.M. Conceptualization, study design, and editing by L.M. Conceptualization, study design, and methodology by B.N.N.T. Reviewing and editing by S.G.R. Conceptualization, study design, methodology, reviewing, and editing by W.L. and G.Y.Y. Conceptualization, study design, methodology, analysis, reviewing, and editing by D.S. All authors certify that they have participated sufficiently in the study, agree to the submitted version of the article, and bear responsibility for it.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The study was funded by the Osher Center for Integrative Medicine at Harvard Medical School and Brigham and Women's Hospital (Grant #01060174). Rosie Friedman is supported by the 2021 JOBST Lymphatic Research Grant awarded by the Boston Lymphatic Symposium, Inc.