
Abstract
Background:
In lymphedema, the accumulation of subcutaneous interstitial fluid is the most characteristic feature. Bioimpedance analysis (BIA) is a promising technique to measure the amount of body components using a noninvasive method. In this study, we determined the clinical significance of BIA parameters in upper limb lymphedema with surgical treatment such as lymphovenous anastomosis or vascularized lymph node transfer.
Methods and Results:
A single-center retrospective study using a multifrequency BIA. Perioperative BIA parameters such as extracellular water ratio or fat-free mass (FFM) ratio and limb volume defined as percentage of excess volume (PEV) were measured. The relationships between the magnitude of change in PEV and BIA parameters during surgery were evaluated. Out of 48 unilateral lymphedema patients, 46 were female and the average age was 55.4 years. PEV and all BIA parameters showed a significant decrease after surgery (p < 0.001). There were significant correlations between ΔPEV and the degree of changes in all BIA parameters. ΔFFM ratio showed the highest correlation with the amount of change in PEV (r = 0.599, p < 0.001).
Conclusion:
BIA parameters correlated well with the volume change after surgery. BIA could be useful as a quick and easy tool for follow-up after lymphedema surgery.
Introduction
Lymphedema is a common debilitating complication of any dysfunction of the lymphatic drainage system.1,2 Upper limb lymphedema reduces the quality of life by negatively affecting the physical, psychological, and emotional well-being of the patients. 2 Upper limb lymphedema develops in more than one out of five breast cancer survivors.3,4 Currently, nonsurgical (conservative) and surgical treatments are being used for upper limb lymphedema patients. Nonsurgical management includes complete decongestive therapy, which includes bandaging, massage, and exercise.1,3 Early detection of breast cancer-related lymphedema and initiation of complete decongestive therapy are effective in managing lymphedema. 5 However, severe cases of lymphedema require surgical treatment because the progression of fibrosis renders conservative treatment ineffective. 6
Surgical treatments for lymphedema include physiological methods, which create new pathways to bypass the damaged lymphatic vessels to improve the flow through the venous system, and debulking methods, which directly remove the accumulated fluid and fat. 7 Lymphaticovenous anastomosis (LVA) and vascularized lymph node transfer (VLNT) do not directly change the composition of the affected limb but promote the absorption of the accumulated fluid by improving the lymphatic flow.
To evaluate the treatment effect of LVA, clinicians have generally used the volume measurement methods; limb circumference measurement, water-displacement plethysmography, and perometer.8,9 However, the limb volume is not solely composed of subcutaneous interstitial fluid. To accurately assess the residual lymphatic function, they applied lymphatic flow assessment methods (lymphoscintigraphy and lymphangiography). In addition, to explore the status of soft tissues, body component assessment methods (bioimpedance analysis [BIA], computed tomography, magnetic resonance imaging, and dual-energy X-ray absorptiometry [DXA]) were used. Among these, BIA is a quick and easy way to measure the status of lymphedema.
BIA is a noninvasive method of estimating the volume and distribution of body water by calculating the impedance, which is composed of resistance and reactance using an alternating current of various frequencies. 10 Several studies have shown that BIA enables early detection with higher sensitivity than conventional circumference measurement in cases undergoing nonsurgical treatment of lymphedema.11–13 Various BIA parameters such as extracellular water (ECW)/intracellular water index and ECW ratio (ECW/total body water [TBW]) are used to assess the degree of lymphedema and show better performance than conventional volume measurement.14–16
The use of BIA in lymphedema for early diagnosis, serial follow-up, and interval change of conservative management has been well studied. However, surgical treatment, due to its own invasive nature, may be associated with changes in the water component of soft tissues such as postoperative swelling, muscle wasting due to immobilization, and fibrosis due to scar tissue. Therefore, the application of BIA to surgical treatments needs to be investigated. As with nonsurgical treatment outcomes, a previous study reported that BIA parameters can sensitively reflect the surgical treatment outcome in lower limb lymphedema. 17 There are few studies using BIA to predict the changes in arm volume after surgical treatment of upper limb lymphedema.18,19 In this study, we aimed to analyze the predictive effect of perioperative BIA parameters in patients undergoing upper limb LVA.
Materials and Methods
Participants
Before data collection, we obtained approval for this study from the Institutional Review Board of Asan Medical Center (No. 2021-0276; Seoul, South Korea). We identified patients with unilateral upper limb lymphedema who underwent LVA at the plastic surgery clinic of Asan Medical Center between January 2018 and September 2020. Inclusion criteria were as follows: (1) aged 18 years or older; (2) unilateral upper limb lymphedema; (3) underwent surgical treatment because conservative treatment was ineffective for more than 2 months; (4) did not undergo reoperation during follow-up; and (5) underwent BIA 6 months before and after surgery. We excluded patients who were lost to follow-up for BIA after the acute phase (postoperative period <3 months), those with bilateral lymphedema, and those who underwent debulking surgery.
Perioperative procedures
All patients with upper limb lymphedema were diagnosed by lymphoscintigraphy prior to surgery. Patients underwent complete decongestive therapy for at least 2 months, and surgical treatment was considered if the effect was insufficient or if the patients wanted a better outcome than conservative treatment. 20 In this paper, we will use “surgical treatment” to refer to treatments that do not directly alter fluid distribution, such as LVA and VLNT, rather than liposuction. Among LVA, axillary scar removal with VLNT and simultaneous breast reconstruction, the surgical technique was selected according to the obstruction level of the lymphatic drainage pathway (patient-specific plan).
To find a suitable surgical technique for each patient, a magnetic resonance lymphangiogram was performed to evaluate the overall condition of lymphatics. Based on this, functioning lymphatics were mapped in the hand dorsum and forearm using indocyanine green lymphangiogram and ultrasonography, and LVA with corresponding lymphatics was performed if there were functioning lymphatics. For LVA, superficial collecting lymphatics located in the deep fat layer were used, which were connected with a vein that was adjacent to the selected lymphatics, was similar in size, and had low venous pressure by side-to-end anastomosis. 21
At the same time, the axillary soft tissue was evaluated to determine the presence of depression and the degree of adherence of soft tissue. In cases of severe scarring, radical scar resection was performed for all axillary scar tissues and VLNT was performed at the dead space caused by this. The VLNT donor site was a superficial circumflex iliac artery perforator flap with one or two lymph nodes. Through this procedure, the effect of LVA was maximized by lowering axillary venous pressure caused by compression of the scar tissue. Lymphangiogenesis was promoted by saving fresh adipose tissue around the flap.
In addition, if the patient did not undergo breast reconstruction after mastectomy, the continuity of the lymphatic drainage pathway was secured by performing simultaneous breast reconstruction with a deep inferior epigastric artery perforator flap. The compression bandage for 30–35 mmHg continued immediately after surgery to the 3-month point. From then on, compression tapering was considered according to the patient’s course.
Baseline characteristics
Electronic medical records were reviewed to assess baseline characteristics (age, sex), anthropometric data (weight, height, body mass index), and lymphedema-related characteristics. Lymphedema-related characteristics included the laterality of involvement, the time interval between BIA and surgery, the type of surgery, the International Society of Lymphology (ISL) stage, history of cellulitis, and etiology. In cases of secondary lymphedema, a history of chemotherapy and radiotherapy was confirmed. The results of lymphoscintigraphy were classified into five stages according to the dermal backflow and lymph node uptake: type 1 (reduced lymph node uptake only), type 2 (restricted proximal dermal backflow), type 3 (proximal and distal dermal backflow), type 4 (restricted distal dermal backflow), and type 5 (absent dermal backflow and lymph node uptake). 22 If accurate information could not be identified, the result was classified as unknown.
Lymphedema measurement
Before and after surgery, the circumferences of the affected side were measured 15 cm above and below the cubital crease at 5 cm intervals. The volume of each segment was calculated using the following formula:
Total arm volume was the summation of each segment. To standardize the differences in an individual’s arm volume, percent excess volume (PEV), which is defined as ([volume of affected limb − volume of unaffected limb]/volume of unaffected limb), was used. The difference of PEV between before and after surgery was defined as ΔPEV.
BIA was measured using a multifrequency bioelectrical impedance analyzer (InBody 720; InBody Co., Ltd., Seoul, Republic of Korea). The BIA results that were measured at the closest to the point of 6 months before and after surgery were selected. The BIA parameters included (1) ECW ratio, calculated as the ratio of ECW to TBW, (2) the single frequency BIA (SFBIA) ratio at 1 kHz of the unaffected limb on the affected limb, and SFBIA ratio at 5 kHz was analyzed in the same way, and (3) the fat-free mass (FFM) ratio, defined as the FFM of the affected limb divided by that of the unaffected limb. In addition, the ECW ratio was defined in two ways; the value of the affected limb as ECW ratio aff and the ratio of the affected limb to the unaffected limb as ECW ratio aff/unaff. As with PEV, the amount of change in the index before and after surgery was defined as ΔFFM ratio, ΔECW ratio aff/unaff, ΔECW ratio aff, ΔSFBIA ratio at 1 kHz, and ΔSFBIA ratio at 5 kHz. In all cases, the ratio of the two sides was used to achieve high objectivity.
Statistical analysis
Statistical analysis in this study was conducted using IBM SPSS Statistics for Windows, version 25 (IBM Corp., Armonk, NY). Baseline characteristics of patients were summarized using mean and standard deviation for descriptive data. The difference between before and after surgery of PEV, FFM ratio, ECW ratio aff/unaff, ECW ratio aff, and SFBIA ratio at 1 kHz, and SFBIA ratio at 5 kHz were first tested by Kolmogorov–Smirnov test and then evaluated by paired t-test for values with normal distribution and by Wilcoxon signed-rank test for those with nonnormal distribution. The relationships between ΔPEV and ΔFFM ratio, ΔECW ratio aff/unaff, ΔECW ratio aff, ΔSFBIA ratio at 1 kHz, and ΔSFBIA ratio at 5 kHz were evaluated by Spearman’s correlation test. Finally, the patients were divided into low-stage (type 1–3) and high-stage (type 4–5) groups according to the type of lymphoscintigraphy. We then assessed whether the two groups had differences in preoperative PEV, FFM ratio, ECW ratio of the affected limb, SFBIA ratio at 1 kHz, SFBIA ratio at 5 kHz, and ΔPEV values by using Mann–Whitney test.
Results
Baseline characteristics
Between January 2018 and September 2020, 189 patients underwent surgical treatment for lymphedema. Among them, 59 patients underwent surgery for unilateral upper limb lymphedema. A total of 48 patients were finally included after excluding three patients who underwent bilateral surgery, two patients who underwent debulking surgery (e.g., liposuction), and six patients who did not undergo BIA assessment at the appropriate time (Fig. 1). Table 1 shows the baseline characteristics of the patients. Of the total patients, 46 (95.8%) were female and the mean age was 55.4 years. Thirty patients underwent LVA alone, and 18 patients additionally underwent VLNT or flap surgery. The mean time for pre- and postoperative BIA assessment was 198.5 days and 191.5 days, respectively. Stage 2 had the largest number of patients (41 patients), and stage 3 had 6 patients.
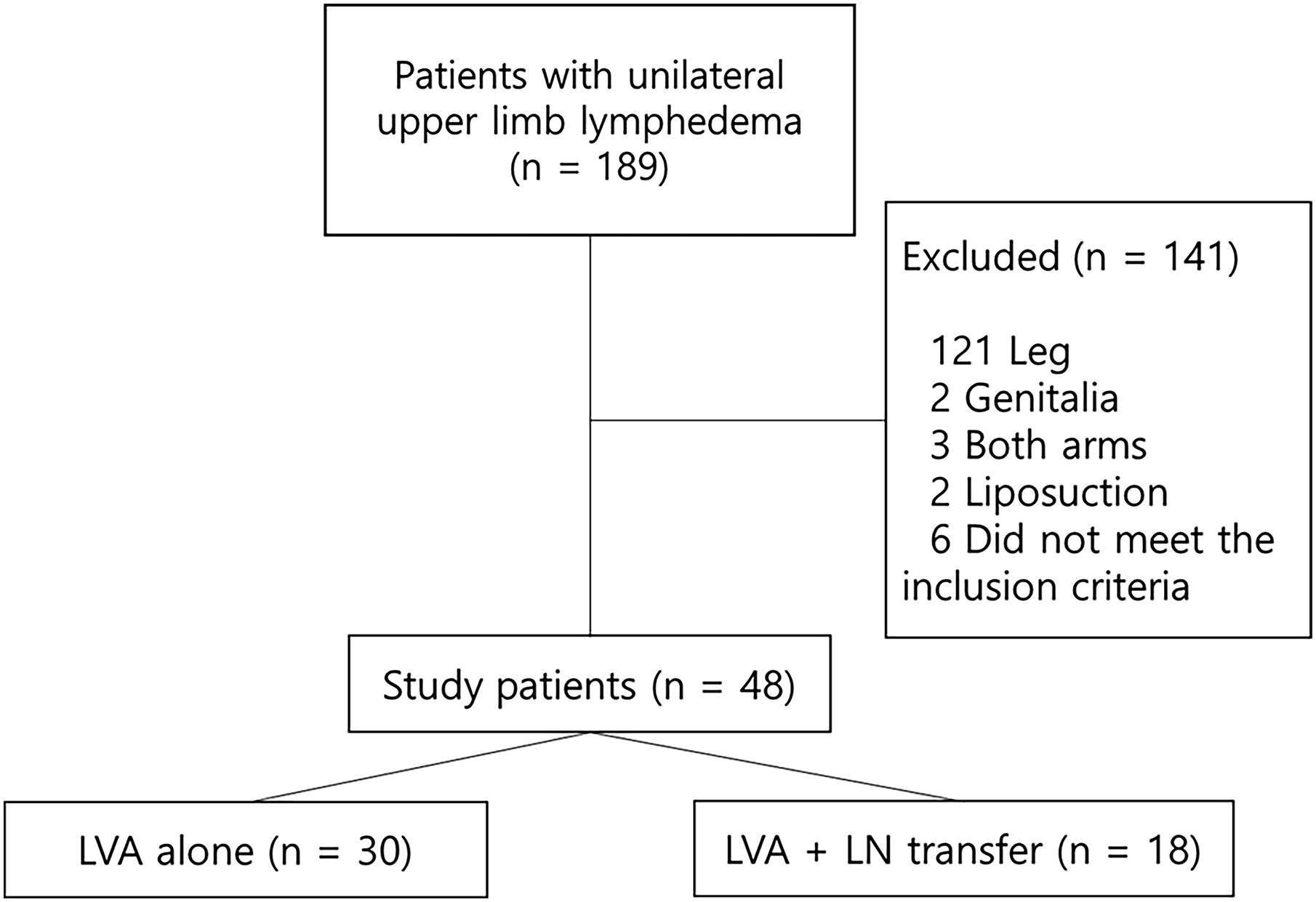
Study population flowchart. LN, lymph node; LVA, lymphovenous anastomosis.
Baseline Characteristics of the Patients
Values are n/N (%) or mean ± standard deviation.
One patient did not undergo lymphoscintigraphy.
BIA, bioimpedance analysis; ISL, International Society of Lymphology; LVA, lymphovenous anastomosis; VLNT, vascularized lymph node transfer.
Bioimpedance parameters
PEV, FFM ratio, ECW ratio aff/unaff, ECW ratio aff, SFBIA ratio at 1 kHz, and SFBIA ratio at 5 kHz were significantly decreased after surgery (Table 2). Also, there were moderate correlations between ΔPEV and the degree of changes in all BIA parameters (Fig. 2). According to the results, the ΔFFM ratio showed the highest correlation with the amount of change in PEV (r = 0.599, p < 0.001).
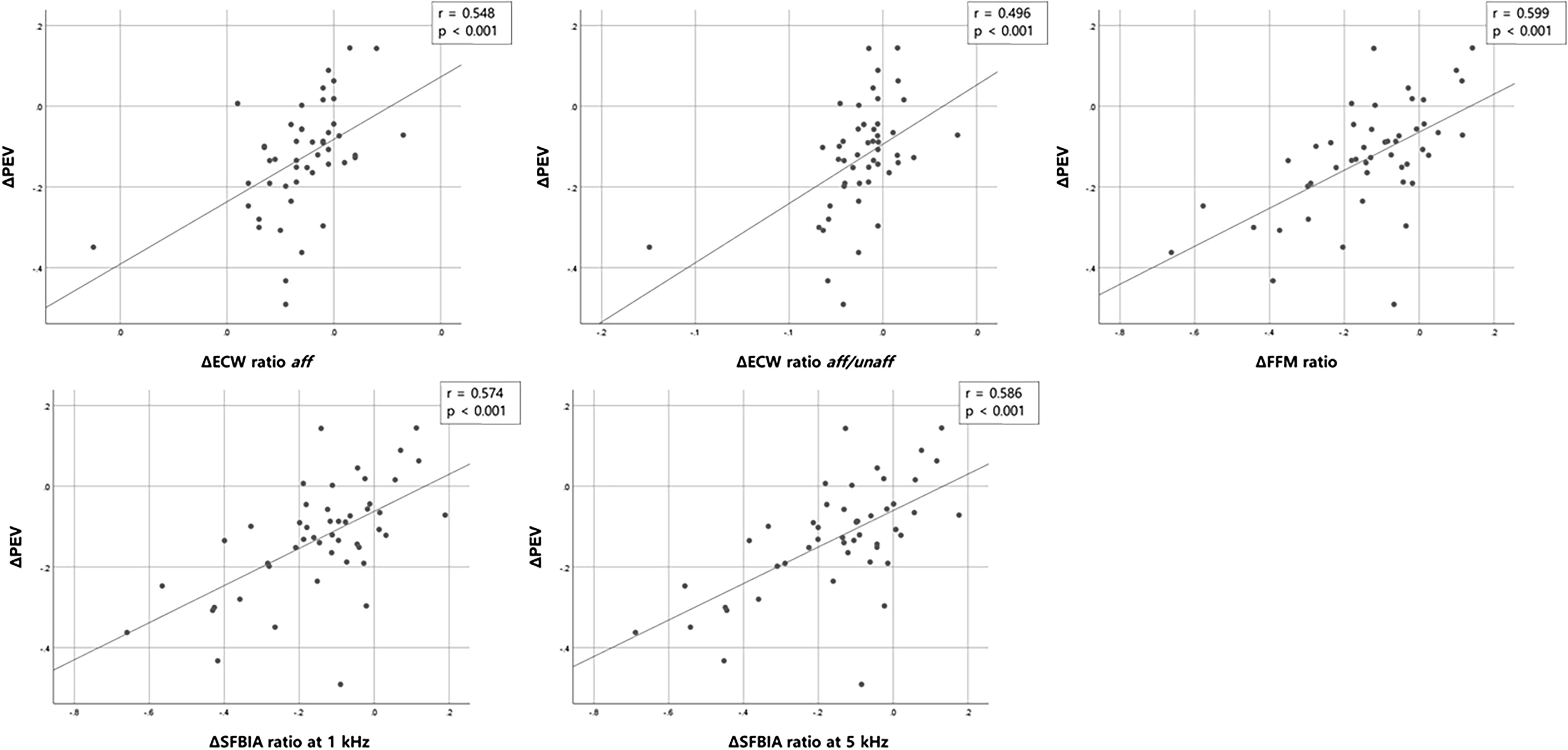
Correlation between ΔPEV and improvements of BIA parameters. BIA, bioimpedance analysis; ECW, extracellular water; FFM, fat-free mass; PEV, percent excess volume; SFBIA, single frequency bioimpedance analysis.
Changes in Lymphedema Parameters After Operation
Values are mean ± standard deviation.
Paired t-test.
Wilcoxon signed-rank test.
aff, affected limb; aff/unaff, affected limb over unaffected limb; ECW, extracellular water; FFM, fat-free mass; PEV, percent excess volume.
After excluding one patient who did not undergo lymphoscintigraphy, 47 patients were divided into the low-stage group (types 1–3; n = 14) and the high-stage group (types 4–5; n = 33). The two groups did not show significant differences in the BIA parameters (Table 3), including the ΔFFM ratio (Fig. 3). In addition, the LVA-only group (n = 30) and the LVA + VLNT group (n = 18) did not show significant differences in the BIA parameters as well (Table 4).
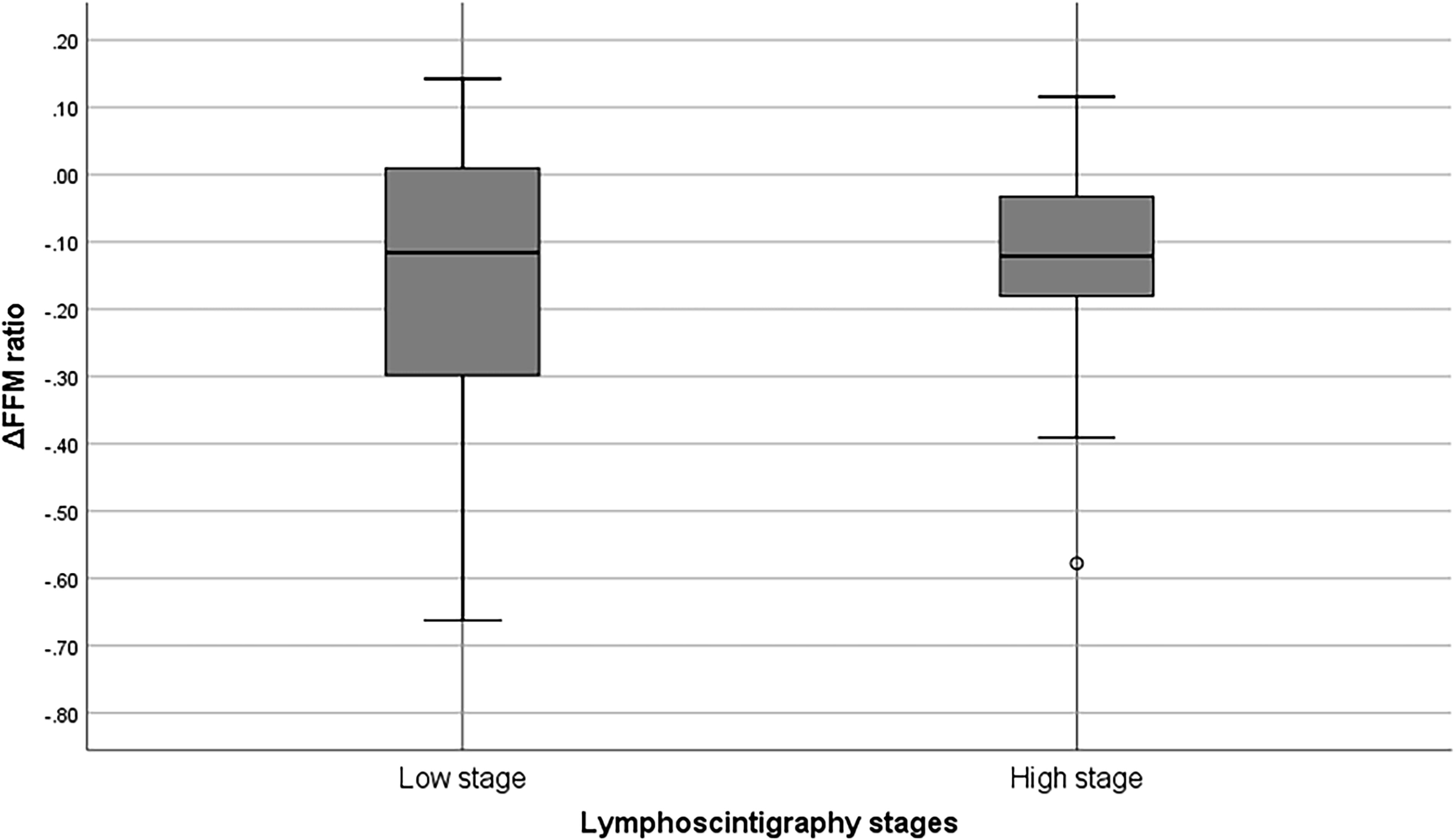
FFM ratio of affected limbs in patients categorized by lymphoscintigraphy stages.
Preoperative Lymphedema Parameters and ΔPEV Between Lymphoscintigraphy Stage Groups
Values are mean ± standard deviation.
Mann–Whitney Test.
SFBIA, single frequency bioimpedance analysis.
Preoperative Lymphedema Parameters and ΔPEV Between Surgical Methods
Values are presented as mean ± SD or as indicated.
*p-Value < 0.05, Mann–Whitney test.
Discussion
We conducted this study to determine whether the lymphatic fluid status could be assessed by BIA parameters before and after surgical treatment in patients with unilateral upper limb lymphedema. We found that all BIA parameters used in this study correlated well with the PEV changes after surgery. This study adds an important piece of evidence on this issue because there have been five reviews on the BIA assessment of surgical treatment and two studies by Yasunaga et al. and Roh et al. for upper limb lymphedema.16–19,23
Our study had several strengths compared with the previous study in that we used multiple single-frequency bioimpedance analysis values (i.e., SFBIA ratio at 1 kHz and SFBIA ratio at 5 kHz) and directly applied the BIA parameter instead of predicted volumes. Furthermore, the patient cohort in our study was larger (48 vs. 19), and the cohort was not only limited to those who received LVA but also included those who underwent additional surgical treatment. In addition, the previous study did not include patients with ISL stage III, whereas 13% of the patients in our study were ISL stage III. This is important because advanced stages of lymphedema have less fluid components and are thus more difficult to be analyzed by BIA. Finally, the previous study analyzed the results based on the indirectly derived limb water volume from the ECW ratio of BIA and suggested that the surgical treatment outcome could be predicted by the preoperative body water volume difference between the affected and unaffected limbs calculated by BIA. 18 In contrast, our study minimized the differences in intersubject variables by employing the ratio of both sides instead of relying on unilateral value. Unilateral value can be influenced by the individual anthropometric data, gravity, or activities such as urination or defecation. In a study similarly conducted in the lower limb, ΔECW ratio aff/unaff was suggested to have the highest predictability. 23 However, in contrast to previous studies, our study showed that ΔFFM ratio had the highest predictability among several BIA parameters.
FFM value in BIA is usually calculated from TBW and hydration fraction (HF), and HF can be affected by lymphedema. 24 As the lymphedema improves, HF normalizes. This causes the overestimated FFM to normalize. Therefore, it can be assumed that the ΔFFM ratio may reflect the improvement in fluid status. 24 In addition, the patient cohort of this study differs from those of previous studies in that there were many advanced lymphedema patients with fibroadipose tissue accumulation, and surgical treatment could be performed without direct removal of adipose tissue. This could be an important confounding factor. Therefore, the explanatory power of the BIA parameter, ECW ratio, representing fluid accumulation may have been limited in this study.
Surgical treatment of lymphedema was previously thought to be less effective in the advanced stage due to the impaired residual functional lymphatic system. 25 However, a recent study suggested that surgical treatment is effective even in the clinically advanced stage. 26 In addition, some studies showed that more severe dermal backflow on lymphoscintigraphy was associated with a better effect of LVA. 27 However, this study did not show significant differences in the BIA parameters when the patients were categorized according to the lymphoscintigraphy type. Considering that lymphoscintigraphy measures lymphatic flow and BIA indicates fluid accumulation status, which is a temporal summation of lymphatic flow, the results could not be reconciled. In addition, our study is the first to analyze the effect of different types of surgical treatment (VLNT and flap surgery) and found that there were no significant differences in the BIA parameters between the surgical groups.
In several studies, BIA was utilized for the diagnosis or assessment of lymphedema as well as serial follow-up for the effectiveness of complete decongestive therapy. 28 However, there was a lack of evidence regarding patients who underwent surgery, which made it difficult for surgeons to quantitatively evaluate the effectiveness of the treatment. The results of this study provide empirical evidence on the usefulness of this objective tool in patients undergoing surgery. They also suggest that serial BIA may facilitate the monitoring of patients’ severity through the assessment of ECW status.
As a limitation of this study, the laterality of the dominant hand was not analyzed due to limited data. It could be a confounding factor in that asymmetrical skeletal muscl mass can lead to differences in water distribution. Also, if radiotherapy had been further analyzed to determine whether nodal irradiation was performed, a more accurate analysis would have been possible; however, in this single-center study, we could not check the records of other hospitals for this information. In addition, long-term outcomes could not be assessed because of the short monitoring period of 6 months. Lastly, we could not evaluate the patients’ functional improvement, symptoms, and quality of life. Further research is needed to overcome the limitations of our study.
Conclusion
In patients with unilateral upper limb lymphedema who underwent LVA, BIA parameters showed moderate correlation with the surgical outcomes. BIA may be useful as a less painful, quick, and accessible tool for surgeons to use in serial follow-up after lymphedema surgery.
Footnotes
Acknowledgments
The authors thank the members of the lymphedema therapist team and lymphedema patients who participated in the study.
Authors’ Contributions
M.G.K.: Conceptualization, data curation, formal analysis, investigation, and writing-original draft. W.C.S.: Conceptualization, investigation, and writing—review and editing. J.G.K.: Conceptualization and methodology. J.P.H.: Conceptualization, methodology, and writing—review and editing. H.S.S.: Conceptualization, methodology, and writing—review and editing. S.A.K.: Conceptualization and investigation. H.Y.C.: Conceptualization and investigation. M.N.G.: Conceptualization and methodology. J.Y.H.: Conceptualization, methodology, project administration, supervision, and writing—review and editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by a grant (No.