
Abstract

Keynote Article
Bonet, F., et al. (2022). “CCBE1 in Cardiac Development and Disease.” Front Genet 13: 836694. E-Pub 2022/03/01
The collagen- and calcium-binding EGF-like domains 1 (CCBE1) is a secreted protein extensively described as indispensable for lymphangiogenesis during development enhancing VEGF-C signaling. In human patients, mutations in CCBE1 have been found to cause Hennekam syndrome, an inherited disease characterized by malformation of the lymphatic system that presents a wide variety of symptoms such as primary lymphedema, lymphangiectasia, and heart defects. Importantly, over the last decade, an essential role for CCBE1 during heart development is being uncovered. In mice, Ccbe1 expression was initially detected in distinct cardiac progenitors such as first and second heart field, and the proepicardium. More recently, Ccbe1 expression was identified in the epicardium and sinus venosus (SV) myocardium at E11.5-E13.5, the stage when SV endocardium-derived (VEGF-C dependent) coronary vessels start to form. Concordantly, CCBE1 is required for the correct formation of the coronary vessels and the coronary artery stem in the mouse. Additionally, Ccbe1 was found to be enriched in mouse embryonic stem cells (ESC) and revealed as a new essential gene for the differentiation of ESC-derived early cardiac precursor cell lineages. Here, we bring an up-to-date review on the role of CCBE1 in cardiac development, function, and human disease implications. Finally, we envisage the potential of this molecule's functions from a regenerative medicine perspective, particularly novel therapeutic strategies for heart disease.
Hennekam Syndrome may be due to mutations in the CCBE1, FAT4, or ADAMS3 genes (1,2,3), causing generalized lymphatic dysplasia and occasionally cardiac defects. This manuscript provides a comprehensive review of the role of CCBE1 (Collagen and calcium-binding EGF domain-containing protein in cardiac and cardiac vascular development. The authors provide a comprehensive review of cardiac embryology, referencing recent and historical research in this field. They refer to several studies which provided evidence for the interaction between CCBE1 and VEGF-C, enhancing high-affinity binding with VEGFR-3, citing studies using animal models with knocked down, defective, or blocked CCBE1. They conclude that CCBE1 has the potential to increase cardiac vasculature (neoangiogenesis) in cardiovascular disease. The authors postulate that CCBE1 expressing cells +/− controlled release of rCCBE proteins or small peptides into diseased hearts may lead to enhanced cardiovascular progenitor formation and subsequent myocardial regeneration (Fig. 1).
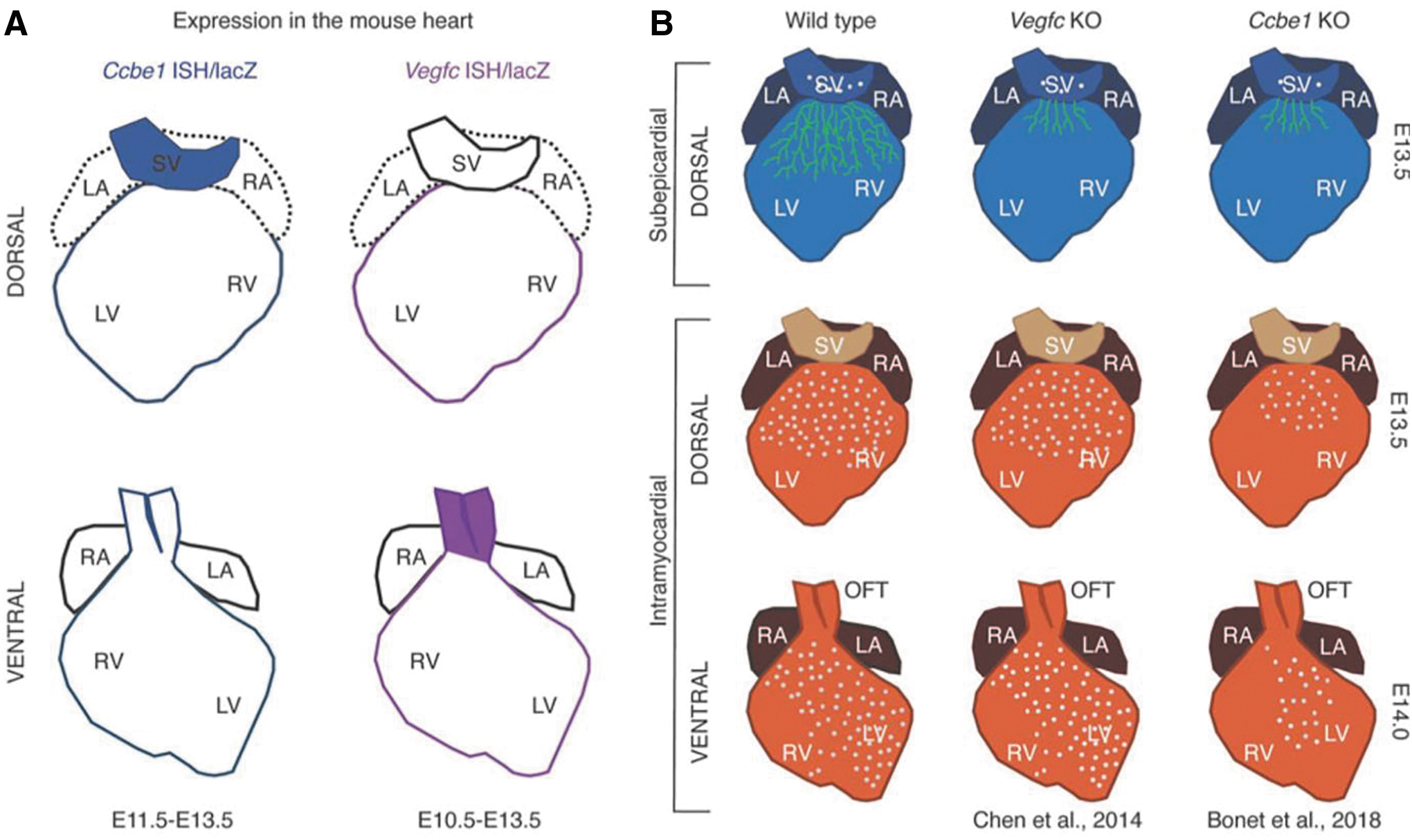
Schematic of Ccbe1 and Vegfc expression and heart phenotypes. A): Ccbe1 and Vegfc expressions are colocalized in the epicardium from E10.5 onward. Ccbe1 expression is also present in the SV (sinus venosus). Vegfc is expressed in the vessel wall of the aorta and pulmonary artery, whereas Ccbe1 is restricted to the aortic epicardium. B): Schematic representation of heart phenotype in Ccbe1 KO vs Vegfc KO mice shows that both mutant lines display underdeveloped dorsal subepicardial coronary vessels, however, Ccbe1 phenotype extends to defective dorsal and ventral intramyocardial vessels. Green draws represent subepicardial vessels. Gray dots represent intramyocardial vessels. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
Basic Science
Johnson, L. A. (2022). “Analyzing Lymphatic Vessel Patterning in Adult Tissue.” Methods Mol Biol 2441: 85–94. E-Pub 2022/02/01
Whole-mount immunostaining allows intact tissue to be surveyed in three dimensions, avoiding the more restricted fields of view provided by visualizing thin sections. This technique is particularly useful for imaging lymphatic and blood networks by high-resolution confocal microscopy, revealing how such vessels are spatially positioned, the subcellular arrangements of individual antigens, and interactions with individual cells within the interstitium or vessel lumen. The purpose of this chapter is to provide a practical guide for obtaining images of lymphatic vessels following immunofluorescence staining, primarily in mouse skin.
Bai, J., et al. (2022). “Angiotensin II Induces Cardiac Edema and Hypertrophic Remodeling through Lymphatic-Dependent Mechanisms.” Oxid Med Cell Longev 2022: 5044046. E-Pub 2022/03/01
Cardiac lymphatic vessel growth (lymphangiogenesis) and integrity play an essential role in maintaining tissue fluid balance. Inhibition of lymphatic lymphangiogenesis is involved in cardiac edema and cardiac remodeling after ischemic injury or pressure overload. However, whether lymphatic vessel integrity is disrupted during angiotensin II- (Ang II-) induced cardiac remodeling remains to be investigated. In this study, cardiac remodeling models were established by Ang II (1000 ng/kg/min) in VEGFR-3 knockdown (Lyve-1(Cre) VEGFR-3(f/-)) and wild-type (VEGFR-3(f/f)) littermates. Our results indicated that Ang II infusion not only induced cardiac lymphangiogenesis and upregulation of VEGF-C and VEGFR-3 expression in the time-dependent manner but also enhanced proteasome activity, MKP5 and VE-cadherin degradation, p38 MAPK activation, and lymphatic vessel hyperpermeability. Moreover, VEGFR-3 knockdown significantly inhibited cardiac lymphangiogenesis in mice, resulting in exacerbation of tissue edema, hypertrophy, fibrosis superoxide production, inflammation, and heart failure (HF). Conversely, administration of epoxomicin (a selective proteasome inhibitor) markedly mitigated Ang II-induced cardiac edema, remodeling, and dysfunction; upregulated MKP5 and VE-cadherin expression; inactivated p38 MAPK; and reduced lymphatic vessel hyperpermeability in WT mice, indicating that inhibition of proteasome activity is required to maintain lymphatic endothelial cell (LEC) integrity. Our results show that both cardiac lymphangiogenesis and lymphatic barrier hyperpermeability are implicated in Ang II-induced adaptive hypertrophic remodeling and dysfunction. Proteasome-mediated hyperpermeability of LEC junctions plays a predominant role in the development of cardiac remodeling. Selective stimulation of lymphangiogenesis or inhibition of proteasome activity may be a potential therapeutic option for treating hypertension-induced cardiac remodeling.
Wei, H., et al. (2022). “CD137L-macrophage induce lymphatic endothelial cells autophagy to promote lymphangiogenesis in renal fibrosis.” Int J Biol Sci 18(3): 1171–1187. E-Pub 2022/02/18
Renal lymphangiogenesis is a new field of international nephrology in recent years and plays an important role in the progression of chronic renal disease. CD137 was originally described as a surface molecule present on activated T and NK cells and detected on hypoxic endothelial cells and inflamed blood vessels, but its function on lymphatic endothelial cells remains unclear. We investigated the relationships among CD137, lymphangiogenesis and macrophages, which are involved in interstitial fibrosis. Similar to other chronic inflammatory diseases, we found lymphangiogenesis and expression of CD137 in the renal tissue of patients with IgA nephropathy. CD137-positive lymphatic vessels were involved in the development process of IgA nephropathy and positively correlated with serum creatinine, serum urea nitrogen, serum uric acid, and urinary 24 h total protein. The expression of these indicators was negatively correlated with eGFR, plasma albumin, and HB. In mouse models of UUO, we verified that CD137 expression was significantly elevated during lymphangiogenesis and that its ligand CD137L was released by macrophages after VEGF-C stimulation in the kidney. In vitro, recombinant CD137L significantly enhanced LEC proliferation, migration and tube formation, and these effects were inhibited by CD137 siRNA. Mechanistically, the CD137L interaction with CD137 induced the transition from LC3-I to LC3-II and the expression of Atg5, Atg7, Atg12 and p62 proteins by activating the PI3K/AKT/mTOR pathway to promote autophagy. Knockdown of Atg5 and Atg7 blocked CD137L-induced autophagy. Thus, we propose that CD137L secretion by macrophages interacts with CD137 on lymphatic endothelial cells to prompt lymphangiogenesis in the kidney, which further drives fibrogenic responses. Our findings suggest that inhibition of the CD137-CD137L pathway is a novel therapeutic approach for obstructive nephropathy.
Yang, Y., et al. (2022). “EGR1 Enhances Lymphangiogenesis via SOX18-Mediated Activation of JAK2/STAT3 Pathway.” Comput Math Methods Med 2022: 6448724. 2 E-Pub 022/02/23
Background: Lymphangiogenesis is a process involved in the pathogenesis of many diseases. Identifying key molecules and pathway targeting this process is critical for lymphatic regeneration-associated disorders. EGR1 is a transcription factor, but its function in lymphangiogenesis is not yet known. This study is aimed at exploring the functional activity and molecular mechanism of EGR1 implicated in lymphangiogenesis. Methods: The CCK-8 method, transwell migration assay, and tube formation assay were used to detect the cell viability, motility, and tube formation of HDLEC cells, respectively. The luciferase reporter assay was applied to detect the impact of EGR1 on SOX18 promoter activity. CHIP assay was used to analyze the direct binding of EGR1 to the SOX18 promoter. qRT-PCR and Western blot analysis were performed to investigate molecules and pathway involved in lymphangiogenesis. Results: The EGR1 ectopic expression markedly increased the cell growth, mobility, tube formation, and the expression of lymphangiogenesis-associated markers (LYVE-1 and PROX1) in HDLEC cells. EGR1 interacted with the SXO18 gene promoter and transcriptionally regulated the SXO18 expression in HDLEC cells. Silencing of SOX18 abrogated the promotional activities of EGR1 on the cell viability, mobility, tube formation, and LYVE-1/PROX1 expression in HDLEC cells. SOX18 overexpression activated JAK/STAT signaling, which resulted in an increase in lymphangiogenesis in HDLEC cells. Conclusions: ERG1 can promote lymphangiogenesis, which is mediated by activating the SOX18/JAK/STAT3 cascade. ERG1 may serve as a promising target for the therapy of lymphatic vessel-related disorders.
Akangire, G., et al. (2022). “EPHB4 Mutation Suppresses PROX1 Expression and Disrupts Lymphatic Development in Neonatal Hydrops.” Pediatrics 149(3). E-Pub 2022/02/19
This case report highlights the importance of screening for mutations in EPHB4 and other genes that regulate lymphatic development in infants with the nonimmune hydrops fetalis.
Duan, M., et al. (2022). “A Facile and Highly Efficient Approach to Obtain a Fluorescent Chromogenic Porous Organic Polymer for Lymphatic Targeting Imaging.” Molecules 27(5). E-Pub 2022/03/11
Porous organic polymers have an open architecture, excellent stability, and tunable structural components, revealing great application potential in the field of fluorescence imaging, but this part of the research is still in its infancy. In this study, we aimed to tailor the physical and chemical characteristics of indocyanine green using sulfonic acid groups and conjugated fragments, and prepared amino-grafted porous polymers. The resulting material had excellent solvent and thermal stability, and possessed a relatively large pore structure with a size of 3.4 nm. Based on the synergistic effect of electrostatic bonding and pi-pi interactions, the fluorescent chromogenic agent, indocyanine green, was tightly incorporated into the pore cavity of POP solids through a one-step immersion method. Accordingly, the fluorescent chromogenic POP demonstrated excellent imaging capabilities in biological experiments. This preparation of fluorescent chromogenic porous organic polymer illustrates a promising application of POP-based solids in both fluorescence imaging and biomedicine applications.
Oliver, G. (2022). “Lymphatic endothelial cell fate specification in the mammalian embryo: An historical perspective.” Dev Biol 482: 44–54. E-Pub 2021/12/17
Development of the mammalian lymphatic vasculature is a stepwise process requiring the specification of lymphatic endothelial cell progenitors in the embryonic veins, and their subsequent budding to give rise to most of the mature lymphatic vasculature. In mice, formation of the lymphatic vascular network starts inside the cardinal vein at around E9.5 when a subpopulation of venous endothelial cells gets committed into the lymphatic lineage by their acquisition of Prox1 expression. Identification of critical genes regulating lymphatic development facilitated the detailed cellular and molecular characterization of some of the cellular and molecular mechanisms regulating the early steps leading to the formation of the mammalian lymphatic vasculature. A better understanding of basic aspects of early lymphatic development, and the availability of novel tools and animal models has been instrumental in the identification of important novel functional roles of this vasculature network.
Syed-Abdul, M. M., et al. (2022). “Lymphatics - not just a chylomicron conduit.” Curr Opin Lipidol. E-Pub 2022/03/09
PURPOSE OF REVIEW: Lymphatics are known to have active, regulated pumping by smooth muscle cells that enhance lymph flow, but whether active regulation of lymphatic pumping contributes significantly to the rate of appearance of chylomicrons (CMs) in the blood circulation (i.e., CM production rate) is not currently known. In this review, we highlight some of the potential mechanisms by which lymphatics may regulate CM production. RECENT FINDINGS: Recent data from our lab and others are beginning to provide clues that suggest a more active role of lymphatics in regulating CM appearance in the circulation through various mechanisms. Potential contributors include apolipoproteins, glucose, glucagon-like peptide-2, and vascular endothelial growth factor-C, but there are likely to be many more. SUMMARY: The digested products of dietary fats absorbed by the small intestine are re-esterified and packaged by enterocytes into large, triglyceride-rich CM particles or stored temporarily in intracellular cytoplasmic lipid droplets. Secreted CMs traverse the lamina propria and are transported via lymphatics and then the blood circulation to liver and extrahepatic tissues, where they are stored or metabolized as a rich energy source. Although indirect data suggest a relationship between lymphatic pumping and CM production, this concept requires more experimental evidence before we can be sure that lymphatic pumping contributes significantly to the rate of CM appearance in the blood circulation.
Kim, H. M., et al. (2022). “Radiofrequency Irradiation Mitigated UV-B-Induced Skin Pigmentation by Increasing Lymphangiogenesis.” Molecules 27(2). E-Pub 2022/01/22
Dermal macrophages containing melanin increase skin pigmentation since dermal melanin removal is slower than epidermal melanin removal. Lymphatic vessels are also involved in melanin clearance. We evaluated whether radiofrequency (RF) irradiation induced an increase in HSP90, which promotes lymphangiogenesis by activating the BRAF/MEK/ERK pathway and decreasing tyrosinase activity, in the UV-B exposed animal model. The HSP90/BRAF/MEK/ERK pathway was upregulated by RF. Tyrosinase activity and the VEGF-C/VEGFR 3/PI3K/pAKT1/2/pERK1/2 pathway, which increase lymphangiogenesis, as well as the expression of the lymphatic endothelial marker LYVE-1, were increased by RF. Additionally, the number of melanin-containing dermal macrophages, the melanin content in the lymph nodes, and melanin deposition in the skin were decreased by RF. In conclusion, RF increased HSP90/BRAF/MEK/ERK expression, which decreased tyrosinase activity and increased lymphangiogenesis to eventually promote the clearance of dermal melanin-containing macrophages, thereby decreasing skin pigmentation.
Juneja, P., et al. (2022). “Revisiting the gut-liver axis: gut lymphatic system in liver cirrhosis and portal hypertension.” Am J Physiol Gastrointest Liver Physiol. E-Pub 2022/02/24
The lymphatic vascular system runs parallel to the blood vascular system, comprising a network of lymphatic vessels and secondary lymphoid organs. The intestinal lymphatic capillaries (lacteals) and the associated collecting vessels in the mesentery form the gut lymphatic system. The gut lymphatic vasculature comprises the longest-studied lymphatic vessel bed and plays a significant role in the uptake and transport of dietary fat, abdominal fluid balance, and gut immunosurveillance. Gut is closely connected to liver through the portal circulation. In several experimental and clinical studies, the ‘gut-liver-axis' has been demonstrated to contribute to the pathogenesis of portal hypertension, liver cirrhosis, and its complications. Given a significant impact of gut health on the liver, in the current review, we highlight ‘gut-liver axis' in context to the circulatory physiology of gut lymphatic vessels. Despite their paramount importance in maintaining fluid and immune homeostasis in the gut, gut lymphatic vessels remain one of the most understudied physiological systems in liver disease pathology. In the current review, we delineate the connections of gut lymphatics with abdominal fluid homeostasis and bacterial translocation in the pathogenesis of liver cirrhosis and portal hypertension. We describe mechanisms and factors that drive gut lymphangiogenesis and lymphatic vessel dysfunction during inflammation. The review also underscores the role of gut lymphatic endothelial cells in regulating gut and liver immunity. We finally discuss the prognostic and therapeutic prospects of studying gut lymphatic vessels in advanced liver cirrhosis.
Pereira de Godoy, J. M., et al. (2021). “Stimulation of Synthesis and Lysis of Extracellular Matrix Proteins in Fibrosis Associated with Lymphedema.” Dermatopathology (Basel) 9(1): 1–10. E-Pub 2022/01/26
Background: Fibrotic diseases pose a problem for overall health due to their chronic, progressive nature; the lack of a cure; and the fact that such conditions are largely refractory to current medical and surgical treatment practices. Objective: The aim of the present study was to report the physiological stimulation of synthesis and lysis of extracellular matrix proteins during the treatment of primary lymphedema. Material and Methods: A clinical trial was conducted involving the analysis of changes in type I and III collagen fibers and elastic fibers as well as the thickness of the epidermis and dermis in 10 histological fields. Samples were taken from the skin before and after intensive treatment using the Godoy Method((R)) and adapted to the treatment of fibrosis in a patient with a clinical diagnosis of lower limb lymphedema. Slides were stained with orcein, hematoxylin and eosin, picrosirius red, and Gomori's reticulin stains. Weibel's multipoint method was used for the morphometric evaluation. The data were compared using the t-test with a 95% confidence interval. Results: Significant changes were detected in all aspects of interest (thickness of the epidermis and dermis, type I and III collagen fibers, and elastic fibers). Conclusion: The present findings demonstrate the physiological stimulation of synthesis and lysis of the main components of an extracellular matrix, such as type I and III collagen fibers and elastic fibers, as well as a reduction in the thickness of the epidermis and dermis in cases of fibrosis through adequate stimulation of the lymphatic system.
Clinical
Hettrick, H. and F. Aviles (2022). “All edema is lymphedema: progressing lymphedema and wound management to an integrated model of care.” Wound Manag Prev 68(1): 8–15. E-Pub 2022/03/10
BACKGROUND: Chronic edema affects millions of people in the United States and worldwide. Edema can result from a variety of diseases, trauma, medications, and other contributing factors; however, all edema is related to lymphatic fluid dysregulation. Additionally, lymphatic impairment and integumentary dysfunction are interrelated, leading to complex clinical presentations that require an integrated medical model of care to maximize outcomes. PURPOSE: This narrative review article will highlight the current evidence that details lymphatic physiology, fluid regulation by the endothelial glycocalyx layer, and the interconnectedness of the vascular and integumentary systems leading to a paradigm shift in our understanding of edema, lymphedema, and chronic wounds. Traditional pedagogy remains siloed with respect to the body systems, whereas current evidence indicates a certain interdependence, particularly between and among the venous, lymphatic, and integumentary systems. METHODS: Comprehensive narrative review of the current and past literature (2010–2021 through PubMed, Google Scholar, MEDLINE Complete, UpToDate) focusing on lymphatic physiology, fluid regulation, the endothelial glycocalyx layer, lymphedema, and venous insufficiency. Review focuses on new evidence supporting the interconnectedness of the systems to support a unified medical management approach. RESULTS: All edema is related to lymphatic dysfunction, whether transient or permanent, thereby creating a lymphedema continuum. Further, lymphatic impairment creates cutaneous regions of skin barrier failure, rendering the skin more susceptible to breakdown and chronic wounds. CONCLUSION: A synthesis of the current evidence suggests an interconnected relationship of the lymphatic, venous, and integumentary systems, highlighting the need for a more integrated medical model of care to provide efficient and comprehensive care and improve patient outcomes.
Lurie, F., et al. (2022). “The American Venous Forum, American Vein and Lymphatic Society and the Society for Vascular Medicine expert opinion consensus on lymphedema diagnosis and treatment.” Phlebology: 2683555211053532. E-Pub 2022/03/09
BACKGROUND: Lymphedema imposes a significant economic and social burden in modern societies. Controversies about its risk factors, diagnosis, and treatment permeate the literature. The goal of this study was to assess experts' opinions on the available literature on lymphedema while following the Delphi methodology. METHODS: In December of 2019, the American Venous Forum created a working group tasked to develop a consensus statement regarding current practices for the diagnosis and treatment of lymphedema. A panel of experts was identified by the working group. The working group then compiled a list of clinical questions, risk factors, diagnosis and evaluation, and treatment of lymphedema. Fifteen questions that met the criteria for consensus were included in the list. Using a modified Delphi methodology, six questions that received between 60% and 80% of the votes were included in the list for the second round of analysis. Consensus was reached whenever >70% agreement was achieved. RESULTS: The panel of experts reached consensus that cancer, infection, chronic venous disease, and surgery are risk factors for secondary lymphedema. Consensus was also reached that clinical examination is adequate for diagnosing lymphedema and that all patients with chronic venous insufficiency (C3–C6) should be treated as lymphedema patients. No consensus was reached regarding routine clinical practice use of radionuclide lymphoscintigraphy as a mandatory diagnostic tool. However, the panel came to consensus regarding the importance of quantifying edema in all patients (93.6% in favor). In terms of treatment, consensus was reached favoring the regular use of compression garments to reduce lymphedema progression (89.4% in favor, 10.6% against; mean score of 79), but the use of Velcro devices as the first line of compression therapy did not reach consensus (59.6% in favor vs 40.4% against; total score of 15). There was agreement that sequential pneumatic compression should be considered as adjuvant therapy in the maintenance phase of treatment (91.5% in favor vs. 8.5% against; mean score of 85), but less so in its initial phases (61.7% in favor vs. 38.3% against; mean score of 27). Most of the panel agreed that manual lymphatic drainage should be a mandatory treatment modality (70.2% in favor), but the panel was split in half regarding the proposal that reductive surgery should be considered for patients with failed conservative treatment. CONCLUSION: This consensus process demonstrated that lymphedema experts agree on the majority of the statements related to risk factors for lymphedema, and the diagnostic workup for lymphedema patients. Less agreement was demonstrated on statements related to treatment of lymphedema. This consensus suggests that variability in lymphedema care is high even among the experts. Developers of future practice guidelines for lymphedema should consider this information, especially in cases of low-level evidence that supports practice patterns with which the majority of experts disagree.
Chen, P. F., et al. (2022). “Complex rearrangements of Y chromosome suggest RPS4Y1 as lymphedema candidate gene.” Taiwan J Obstet Gynecol 61(1): 170–173. E-Pub 2022/02/20
OBJECTIVE: Cystic hygromas are frequently encountered in fetus with Turner syndrome (TS). Nevertheless, identification of genetic loci responsible for the cystic hygroma has been problematic. Here, we tried to elucidate the candidate gene for cystic hygroma through a rare case of complex Y chromosomal rearrangements involving duplication of partial Yq and monosomy of partial Yp. CASE REPORT: A 30-year-old woman, gravida 1 para 0, was diagnosed with fetal cystic hygroma at 12 weeks of gestation. The genetic analysis of the product of conception revealed complex rearrangement of Y chromosome: microdeletion in Yp11.2p11.31 and microduplicatin in Yq11.223q11.23. The deleted region spans about 6.25 Mb and includes 76 genes, including SRY. The duplicated region spans about 4.76 Mb and includes 145 genes. CONCLUSION: From this rare case with non-mosaic complex Y-chromosome rearrangements, we could narrow down Turner stigmata critical region to Yp11.2p11.3. We also propose RPS4Y1 as lymphedema candidate gene.
Ramirez-Suarez, K. I., et al. (2022). “Dynamic contrast-enhanced magnetic resonance lymphangiography.” Pediatr Radiol 52(2): 285–294. E-Pub 2021/04/09
Lymphatic flow disorders include a broad spectrum of abnormalities that can originate in the lymphatic or the venous system. The development of these disorders is multifactorial and is most commonly associated with congenital heart diseases and palliative surgeries that these patients undergo. Central lymphatic disorders might be secondary to traumatic leaks, lymphatic overproduction, conduction abnormalities or lymphedema, and they can progress to perfusion anomalies. Several imaging modalities have been used to visualize the lymphatic system. However, the imaging of central lymphatic flow has always been challenging. Dynamic contrast-enhanced magnetic resonance lymphangiography (DCMRL) allows for visualization of central lymphatic flow disorders and has been recently applied for the assessment of plastic bronchitis, protein-losing enteropathy, chylothorax and chylopericardium, among other lymphatic disorders. The hepatic and mesenteric accesses are innovative and promising techniques for better identification and understanding of these abnormalities. The main objectives of this review are to discuss the physiology and anatomy of the lymphatic system and review the current uses of DCMRL in the diagnosis and management of lymphatic flow disorders.
Horn, S., et al. (2021). “Filarial Lymphedema Patients Are Characterized by Exhausted CD4(+) T Cells.” Front Cell Infect Microbiol 11: 767306. E-Pub 2022/01/25
Worldwide, more than 200 million people are infected with filariae which can cause severe symptoms leading to reduced quality of life and contribute to disability-adjusted life years (DALYs). In particular, lymphatic filariasis (LF) caused by Wuchereria bancrofti can lead to lymphedema (LE) and consequently presents a serious health problem. To understand why only a fraction of the infected individuals develop pathology, it is essential to understand how filariae regulate host immunity. The central role of T cells for immunity against filariae has been shown in several studies. However, there is little knowledge about T cell exhaustion, which causes T cell dysfunction and impaired immune responses, in this group of individuals. Recently, we showed that LE patients from Ghana harbor distinct patterns of exhausted effector and memory CD8(+) T cell subsets. Based on these findings, we now characterized CD4(+) T cell subsets from the same Ghanaian patient cohort by analyzing distinct markers within a 13-colour flow cytometry panel. We revealed that LE patients had increased frequencies of CD4(+) T cells expressing exhaustion-associated receptors such as KLRG-1, TIM-3 and PD-1 compared to healthy endemic normal and W. bancrofti-infected individuals. Moreover, CD4(+) T cells in LE patients were characterized by distinct co-expression patterns of inhibitory receptors. Collectively with the previous findings on CD8(+) T cell exhaustion patterns, the data shown here demonstrates that filarial LE patients harbor distinct subsets of exhausted T cells. Thus, T cell exhaustion patterns in LE patients need attention especially in regards to susceptibility of concomitant infections and should be taken into consideration for LE management measures.
Witte, M. H., et al. (2021). “Human chromosome map of lymphedema-lymphangiogenesis genes: Template for current and future discovery.” Lymphology 54(4): 167–169. E-Pub 2022/01/25
We have created a human chromosomal map of the location of known and candidate genes involved in primary lymphedema (PLE). This should facilitate further discovery and provide a basis for understanding microdeletions which cause lymphedema.
Sudduth, C. L. and A. K. Greene (2022). “Lymphedema and Obesity.” Cold Spring Harb Perspect Med. E-Pub 2022/01/26
Lymphedema results from inadequate lymphatic function. Extreme obesity can cause lower extremity lymphedema, termed “obesity-induced lymphedema (OIL).” OIL is a form of secondary lymphedema that may occur once an individual's body mass index (BMI) exceeds 40. The risk of lymphatic dysfunction increases with elevated BMI and is almost universal once BMI exceeds 60. Obesity has a negative impact on lymphatic density in subcutaneous tissue, lymphatic endothelial cell proliferation, lymphatic leakiness, collecting-vessel pumping capacity, and clearance of macromolecules. Lymphatic fluid unable to be taken up by lymphatic vessels results in increased subcutaneous adipose deposition, fibrosis, and worsening obesity. Individuals with OIL are in an unfavorable cycle of weight gain and lymphatic injury. The fundamental treatment for OIL is weight loss.
Adan, F., et al. (2021). “Non-invasive diagnosis of acquired lymphangiectases using optical coherence tomography.” Skin Res Technol 27(2): 293–295. 2020/10/29
Grunherz, L., et al. (2022). “Preoperative Mapping of Lymphatic Vessels by Multispectral Optoacoustic Tomography.” Lymphat Res Biol. E-Pub 2022/03/02
Background: In lymphatic reconstructive surgery, visualization of lymph vessels is of paramount importance. Indocyanine green (ICG) lymphography is the current gold standard in preoperative lymphatic imaging. However, visualization of lymph vessels is often limited by an overlying dermal backflow of ICG, becoming particularly prominent in advanced lymphedema stages. Multispectral optoacoustic tomography (MSOT) has recently been introduced as a promising noninvasive tool for lymphatic imaging. Methods and Results: A single-center proof-of-concept study with a prospective observational design was conducted at the Department of Plastic Surgery and Hand Surgery of the University Hospital Zurich. Between February 2021 and August 2021, seven patients with different grades of lymphedema were analyzed by the MSOT Acuity system before undergoing lymphovenous anastomosis (LVA). Conventional ICG lymphography served as comparison. MSOT succeeded to accurately depict blood and lymphatic vessels at different locations in six patients, including areas of dermal backflow. The MSOT signal of lymph vessels further correlated well with their macroscopic appearance. Conclusion: We could successfully visualize lymphatic vessels in patients with lymphedema by MSOT and establish the new method for preoperative mapping and selection of incision sites for LVA. Regardless of dermal backflow patterns, MSOT proved to be a valuable approach for identifying and clearly discerning between lymphatic and blood vessels.
Landh, E., et al. (2022). “Prospective nanoparticle treatments for lymphangioleiomyomatosis.” Expert Opin Drug Deliv 19(1): 75–86. E-Pub 2022/01/20
INTRODUCTION: Lymphangioleiomyomatosis (LAM) is a rare lung disease that is characterized by smooth muscle-like cell growth in the lungs. The current available oral treatment rapamycin slows down the disease progression but does not result in a cure. Rapamycin is also limited by its low bioavailability and dose-related adverse side effects. New treatments are, therefore, underway to investigate alternative targets and combination therapies for LAM. In recent years, much focus has been on the development of therapies based on inhaled nanotechnology using carriers to deliver drugs, as it is shown to improve drug solubility, local targeted treatment, and bioavailability. AREAS COVERED: This review, therefore, focuses on future prospective treatments for LAM using nanoparticles and lipid-based nanocarriers, including liposomes, solid lipid nanoparticles, micelles, and polymeric nanoparticles. It also investigates how nanoparticles' physicochemical factors such as size and charge can affect the treatment of both pulmonary and extrapulmonary LAM. EXPERT OPINION: Advanced clinical research is still needed to demonstrate the full potential and drive future commercialization of LAM treatments delivered via inhaled lipid nanobased formulations. If successful, the resultant effects will be seen in the improvement in the life expectancy and life quality of LAM patients.
Masui, K., et al. (2022). “A rare case of intestinal lymphangiectasia induced by pazopanib.” Int Cancer Conf J 11(1): 87–90. E-Pub 2022/02/08
A 62-year-old man underwent left radical nephrectomy for left renal cell carcinoma at our hospital in 1999. At the age of 79 years, he was diagnosed with intra-abdominal disseminations, lung metastases, pancreas metastases, and bilateral femoral muscle metastases during a routine follow-up computed tomography scan. The patient began treatment with pazopanib. Four years later, at the age of 83 years, he developed fever, abdominal pain, and general malaise. Blood samples showed liver dysfunction, hypoalbuminemia, and anemia. Contrast-enhanced computed tomography showed thickening of the small bowel wall with marked edema of the submucosa from the third part of the duodenum to the jejunum, suggesting intestinal lymphangiectasia. The diagnosis of intestinal lymphangiectasia was confirmed by small bowel endoscopy and histological examination. The patient's general condition improved after discontinuation of pazopanib without the need for any active therapeutic interventions. The possibility of intestinal lymphangiectasia should be considered in patients with hypoalbuminemia and general malaise during treatment with multikinase inhibitors.
Nikolakis, D., et al. (2022). “The Role of the Lymphatic System in the Pathogenesis and Treatment of Inflammatory Bowel Disease.” Int J Mol Sci 23(3). E-Pub 2022/02/16
Although the number of therapeutic options for the treatment of inflammatory bowel disease (IBD) has increased in recent years, patients suffer from decreased quality of life due to non-response or loss of response to the currently available treatments. An increased understanding of the disease's etiology could provide novel insights for treatment strategies in IBD. Lymphatic system components are generally linked to immune responses and presumably related to inflammatory diseases pathophysiology. This review aims to summarize findings on immune-mediated mechanisms in lymphoid tissues linked with IBD pathogenesis and (potential) novel treatments. Enhanced innate and adaptive immune responses were observed in mesenteric lymph nodes (MLNs) and other lymphoid structures, such as Peyer's patches, in patients with IBD and in animal models. Furthermore, the phenomenon of lymphatic obstruction in the form of granulomas in MLNs and lymphatic vessels correlates with disease activity. There is also evidence that abnormalities in the lymphatic stromal components and lymph node microbiome are common in IBD and could be exploited therapeutically. Finally, novel agents targeting lymphocyte trafficking have been added to the treatment armamentarium in the field of IBD. Overall, gut-associated lymphoid tissue plays a key role in IBD immunopathogenesis, which could offer novel therapeutic targets.
Kontaridis, M. I., et al. (2022). “The seventh international RASopathies symposium: Pathways to a cure-expanding knowledge, enhancing research, and therapeutic discovery.” Am J Med Genet A. E-Pub 2022/03/11
RASopathies are a group of genetic disorders that are caused by genes that affect the canonical Ras/mitogen-activated protein kinase (MAPK) signaling pathway. Despite tremendous progress in understanding the molecular consequences of these genetic anomalies, little movement has been made in translating these findings to the clinic. This year, the seventh International RASopathies Symposium focused on expanding the research knowledge that we have gained over the years to enhance new discoveries in the field, ones that we hope can lead to effective therapeutic treatments. Indeed, for the first time, research efforts are finally being translated to the clinic, with compassionate use of Ras/MAPK pathway inhibitors for the treatment of RASopathies. This biannual meeting, organized by the RASopathies Network, brought together basic scientists, clinicians, clinician scientists, patients, advocates, and their families, as well as representatives from pharmaceutical companies and the National Institutes of Health. A history of RASopathy gene discovery, identification of new disease genes, and the latest research, both at the bench and in the clinic, were discussed.
Chung, J. H., et al. (2021). “Transient lower extremity lymphedema following COVID-19 vaccination: A case report.” Medicine (Baltimore) 100(48): e28092. E-Pub 2022/01/21
RATIONALE: Complications from COVID-19 vaccines have yet to be sufficiently analyzed because they are rapidly approved without long-term data. In particular, there are no case reports of lymphedema in a healthy patient following vaccination. Herein, we report a patient who underwent transient lymphedema after vaccination with BNT16b2. PATIENT CONCERNS: A 79-year-old woman with pitting edema in both lower legs after administration of a second dose of Pfizer vaccine was referred to our clinic. In the absence of clinical evidence of swelling during the laboratory evaluation, we suspected deep vein thrombosis. However, ultrasonographic findings revealed no evidence of venous thrombosis or varicose veins. DIAGNOSIS: On the basis of lymphoscintigraphy, the patient was diagnosed with transient lymphedema with decreased lymphatic transport in both lower extremities. INTERVENTION: The patient received intensive physiotherapy, including complex decongestive physiotherapy and pneumatic pump compression, to improve the lymphatic circulation. Furthermore, the patient was trained to apply a multilayer compressive bandage to the lower extremities. OUTCOMES: At 2 months follow-up after rehabilitative treatment, the patient's symptoms improved without recurring lymphedema. LESSONS: In the absence of clinical evidence of swelling during laboratory evaluation or ultrasonographic investigations suggesting deep vein thrombosis, we should consider the possibility of lymphatic disorders.
Pan, F., et al. (2022). “Treatment of Postoperative Lymphatic Leakage Applying Transpedal Lymphangiography - Experience in 355 Consecutive Patients.” Rofo. E-Pub 2022/01/27
PURPOSE: Report of experience from a single institution in treating postoperative lymphatic leakage (PLL) applying conventional transpedal lymphangiography (TL). MATERIALS AND METHODS: 453 patients with the initial diagnosis of PLL receiving TL between 03/1993 and 09/2018 were identified in the database. Only patients with confirmed PLL were included in the study. The technical success, safety, and treatment success of TL were evaluated. Independent predictors of TL treatment failure were examined using univariate and multivariate logistic regression analysis. RESULTS: 355 consecutive patients (218 men, 137 women; median age of 62 years) who underwent TL for PLL (e. g., chylothorax) after ineffective conservative treatment were included. The median time between causal surgery and TL was 27 days. The median technical success rate of TL was 88.5%, with a median volume of Lipiodol of 10.0 ml. No complication of TL was recorded. Three groups were defined according to the different clinical courses: group A (41/355, 11.5%) - TL with technical failure; group B (258/355, 72.7%) - “therapeutic” TL alone with technical success; and group C (56/355, 15.8%) - “diagnostic” TL with simultaneously invasive treatment (incl. surgical revision and percutaneous sclerotherapy). Treatment success rate and median time to treatment success were higher in group C than in group B, but without significant differences (64.3% vs. 61.6%, p = 0.710; six vs. five days, p = 0.065). Univariate and multivariate logistic regression analyses for group B confirmed drainage volume (> 500 ml/d) and Lipiodol extravasation as independent predictors of TL clinical failure (odds ratios [ORs] of 2.128 and 2.372 [p = 0.005 and p = 0.003, respectively]). CONCLUSION: TL is technically reliable, safe, and effective in treating PLL. When conservative treatment fails, TL can be regarded as the next treatment option. KEY POINTS:. TL is technically reliable, safe, and effective for treating PLL… When conservative treatment fails, TL can be regarded as the next treatment option… Drainage volume > 500 ml/day is an independent predictor of clinical failure after TL… Lipiodol extravasation is an independent predictor of clinical failure after TL. CITATION FORMAT:. Pan F, Richter GM, Do TD et al. Treatment of Postoperative Lymphatic Leakage Applying Transpedal Lymphangiography - Experience in 355 Consecutive Patients. Fortschr Rontgenstr 2022; DOI: 10.1055/a-1717-2467.
Lee, E., et al. (2022). “Understanding Lymphatic Anatomy and Abnormalities at Imaging.” Radiographics 42(2): 487–505. E-Pub 2022/02/19
Lymphatic abnormalities encompass a wide range of disorders spanning solitary common cystic lymphatic malformations (LMs) to entities involving multiple organ systems such as lymphangioleiomyomatosis. Many of these disorders are rare, yet some, such as secondary lymphedema from the treatment of malignancy (radiation therapy and/or lymph node dissection), affect millions of patients worldwide. Owing to complex and variable anatomy, the lymphatics are not as well understood as other organ systems. Further complicating this is the variability in the description of lymphatic disease processes and their nomenclature in the medical literature. In recent years, medical imaging has begun to facilitate a deeper understanding of the physiology and pathologic processes that involve the lymphatic system. Radiology is playing an important and growing role in the diagnosis and treatment of many lymphatic conditions. The authors describe both normal and common variant lymphatic anatomy. Various imaging modalities including nuclear medicine lymphoscintigraphy, conventional lymphangiography, and MR lymphangiography used in the diagnosis and treatment of lymphatic disorders are highlighted. The authors discuss imaging many of the common and uncommon lymphatic disorders, including primary LMs described by the International Society for the Study of Vascular Anomalies 2018 classification system (microcystic, mixed, and macrocystic LMs; primary lymphedema). Secondary central lymphatic disorders are also detailed, including secondary lymphedema and chylous leaks, as well as lymphatic disorders not otherwise easily classified. The authors aim to provide the reader with an overview of the anatomy, pathology, imaging findings, and treatment of a wide variety of lymphatic conditions. ((c))RSNA, 2022.
Oncology
Hayasaka, H., et al. (2022). “CXCL12 promotes CCR7 ligand-mediated breast cancer cell invasion and migration toward lymphatic vessels.” Cancer Sci. E-Pub 2022/02/09
Chemokines are a family of cytokines that mediate leukocyte trafficking and are involved in tumor cell migration, growth, and progression. Although there is emerging evidence that multiple chemokines are expressed in tumor tissues and that each chemokine induces receptor-mediated signaling, their collaboration to regulate tumor invasion and lymph node metastasis has not been fully elucidated. In this study, we examined the effect of CXCL12 on the CCR7-dependent signaling in MDA-MB-231 human breast cancer cells to determine the role of CXCL12 and CCR7 ligand chemokines in breast cancer metastasis to lymph nodes. CXCL12 enhanced the CCR7-dependent in vitro chemotaxis and cell invasion into collagen gels at suboptimal concentrations of CCL21. CXCL12 promoted CCR7 homodimer formation, ligand binding, CCR7 accumulation into membrane ruffles, and cell response at lower concentrations of CCL19. Immunohistochemistry of MDA-MB-231-derived xenograft tumors revealed that CXCL12 is primarily located in the pericellular matrix surrounding tumor cells, whereas the CCR7 ligand, CCL21, mainly associates with LYVE-1(+) intratumoral and peritumoral lymphatic vessels. In the three-dimensional tumor invasion model with lymph networks, CXCL12 stimulation facilitates breast cancer cell migration to CCL21-reconstituted lymphatic networks. These results indicate that CXCL12/CXCR4 signaling promotes breast cancer cell migration and invasion toward CCR7 ligand-expressing intratumoral lymphatic vessels and supports CCR7 signaling associated with lymph node metastasis.
Peil, J., et al. (2022). “New Therapeutic Approaches for Conjunctival Melanoma-What We Know So Far and Where Therapy Is Potentially Heading: Focus on Lymphatic Vessels and Dendritic Cells.” Int J Mol Sci 23(3). E-Pub 2022/02/16
Conjunctival melanoma (CM) accounts for 5% of all ocular melanomas and arises from malignantly transformed melanocytes in the conjunctival epithelium. Current therapies using surgical excision in combination with chemo- or cryotherapy still have high rates for recurrences and metastatic disease. Lately, novel signal transduction-targeted and immune checkpoint inhibitors like cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) inhibitors, programmed cell death protein-1 (PD-1) receptor inhibitors, BRAF- or MEK-inhibitors for systemic treatment of melanoma have improved the outcome even for unresectable cutaneous melanoma, improving patient survival dramatically. The use of these therapies is now also recommended for CM; however, the immunological background of CM is barely known, underlining the need for research to better understand the immunological basics when treating CM patients with immunomodulatory therapies. Immune checkpoint inhibitors activate tumor defense by interrupting inhibitory interactions between tumor cells and T lymphocytes at the so-called checkpoints. The tumor cells exploit these inhibitory targets on T-cells that are usually used by dendritic cells (DCs). DCs are antigen-presenting cells at the forefront of immune response induction. They contribute to immune tolerance and immune defense but in the case of tumor development, immune tolerance is often prevalent. Enhancing the immune response via DCs, interfering with the lymphatic pathways during immune cell migration and tumor development and specifically targeting tumor cells is a major therapeutic opportunity for many tumor entities including CM. This review summarizes the current knowledge on the function of lymphatic vessels in tumor growth and immune cell transport and continues to compare DC subsets in CM with related melanomas, such as cutaneous melanoma and mucosal melanoma.
Meilani, E., et al. (2022). “Psychometric Properties of Quality of Life Questionnaires for Patients with Breast Cancer-Related Lymphedema: A Systematic Review.” Int J Environ Res Public Health 19(5). E-Pub 2022/03/11
BACKGROUNDS: Assessing quality of life (QoL) using a well-developed and validated questionnaire is an essential part of a breast cancer-related lymphedema (BCRL) treatment. However, a QoL questionnaire with the best psychometric properties is so far unknown. The aim of this systematic review is to evaluate the psychometric properties of the questionnaires measuring the QoL of patients with BCRL. METHODS: A thorough search was performed to identify published studies in electronic databases such as Medline (via Ovid), EBSCOhost, PubMed, Scopus, and Web of Science, on 8 February 2022, by using search terms as follows: ‘quality of life’; ‘breast cancer’; ‘upper limb’; ‘lymphedema’; ‘questionnaire’; and ‘measurement properties.’ Two reviewers conducted article selection, data extraction, and quality assessment independently. The third reviewer helped solve any possible disagreements between the two reviewers. The COSMIN checklist and manual were used to assess the quality of included studies. RESULTS: A total of nineteen articles with nine questionnaires were included and assessed using the COSMIN Risk of Bias checklist. Most studies only assessed content validity, structural validity, internal consistency, reliability, and construct validity. Lymph-ICF-UL showed the most ‘sufficient’ and ‘high’ quality of evidence ratings for its measurement properties. CONCLUSION: The most appropriate questionnaire for use based on our assessment is Lymph-ICF-UL.
Weinstein, B., et al. (2022). “Reverse Lymphatic Mapping and Immediate Microsurgical Lymphatic Reconstruction Reduces Early Risk of Breast Cancer-Related Lymphedema.” Plast Reconstr Surg. E-Pub 2022/03/08
BACKGROUND: Breast cancer-related lymphedema is a progressive disease that poses tremendous physical, psychosocial, and financial burden on patients. Immediate lymphaticovenular anastomosis at the time of axillary lymph node dissection is emerging as a potential therapeutic paradigm to decrease the incidence of breast cancer-related lymphedema in high-risk patients. METHODS: Eighty-one consecutive patients underwent reverse lymphatic mapping and, when feasible, supermicrosurgical immediate lymphaticovenular anastomosis at the time of axillary lymph node dissection at a tertiary care cancer center. Patients were followed prospectively in a multidisciplinary lymphedema clinic (plastic surgery, certified lymphatic therapy, dietary, case management) at 3-month intervals with clinical examination, circumferential limb girth measurements, and bioimpedance spectroscopy. An institutional control cohort was assessed for the presence of objectively diagnosed and treated breast cancer-related lymphedema. Data were analyzed by a university statistician. RESULTS: Seventy-eight patients met inclusion, and 66 underwent immediate lymphaticovenular anastomosis. Mean follow-up was 250 days. When compared to a retrospective control group, the rate of lymphedema in patients who underwent immediate lymphaticovenular anastomosis was significantly lower (6 percent versus 44 percent; p < 0.0001). Patients with 6-month follow-up treated with combined adjuvant radiation therapy and chemotherapy had significantly greater risk of developing breast cancer-related lymphedema (p = 0.04) compared to those without combined adjuvant therapy. Arborized anastomotic technique had a statistically shorter operative time than end-to-end anastomosis (p = 0.005). CONCLUSIONS: This series of consecutive patients demonstrate a 6 percent incidence of early-onset breast cancer-related lymphedema with immediate lymphaticovenular anastomosis and an increased risk in those undergoing combined adjuvant treatment. These early data represent an encouraging and substantial decrease of breast cancer-related lymphedema in high-risk patients. CLINICAL QUESTION/LEVEL OF EVIDENCE: Therapeutic, III.
Vascular Anomalies
Peng, K., et al. (2022). “ALKBH5 promotes the progression of infantile hemangioma through regulating the NEAT1/miR-378b/FOSL1 axis.” Mol Cell Biochem. E-Pub 2022/02/20
Our work aims to investigate long non-coding RNA (lncRNA) N6-methyladenosine (m(6)A) modification and its role in infantile hemangioma (IH). The mRNA and protein expression levels were assessed using quantitative real-time polymerase chain reaction, western blot and immunohistochemistry. Me-RIP assay was performed to evaluate lncRNA NEAT1 m(6)A levels. Cell proliferation, migration and invasion were evaluated using cell counting kit-8 assay, transwell migration and invasion assay, respectively. Photo-activatable ribonucleoside-enhanced crosslinking and immunoprecipitation assay was conducted to verify the binding relationship between lncRNA nuclear paraspeckle assembly transcript 1 (NEAT1) and ALKBH5 (an RNA demethylase). The binding relationship between lncRNA NEAT1, microRNA (miR)-378b and FOS-like antigen 1 (FOSL1) was verified using dual-luciferase reporter gene assay and/or RNA immunoprecipitation assay. ALKBH5, lncRNA NEAT1 and FOLS1 expression was elevated in IH tissues, while miR-378b was downregulated. ALKBH5 knockdown suppressed cell proliferation, migration and invasion of IH cells, while promoting cell apoptosis. ALKBH5 promoted lncRNA NEAT1 expression by reducing the m(6)A modification of lncRNA NEAT1. In addition, miR-378b was the target of lncRNA NEAT1, and its overexpression reversed the promotion effect of lncRNA NEAT1 overexpression on IH cell tumor-like behaviors. Moreover, FOLS1 was the target of miR-378b, and its overexpression reversed the inhibitory effect of miR-378b overexpression on IH cell tumor-like behaviors in vitro. ALKBH5 might have great potential as therapeutic target for IH, since ALKBH5 silencing suppressed IH progression by regulation of the NEAT1/miR-378b/FOSL1 axis.
da Fontoura Galvao, G., et al. (2021). “Association of Variants in FCGR2A, PTPN2, and GM-CSF with Cerebral Cavernous Malformation: Potential Biomarkers for a Symptomatic Disease.” Curr Neurovasc Res 18(2): 172–180. E-Pub 2021/06/05
BACKGROUND: Cerebral Cavernous Malformations (CCM) predispose patients to a lifetime risk of seizures and symptomatic hemorrhage. Only a small percentage of people affected will develop clinical symptoms and the molecular mechanisms underlying lesional activity remain unclear. We analyzed a panel of Single Nucleotide Polymorphisms (SNPs) in CCM patients. We looked for plasmatic inflammatory cytokines, checking for a pattern of plasma expression heterogeneity and any correlation with genetic variations identified with different CCM clinical phenotypes. METHODS: This was a case-control study from a long-term follow-up cohort including 23 CCM patients, of which 16 were symptomatic, and 7 were asymptomatic. A 200-SNP panel was considered through next-generation sequencing and 18 different plasma molecules were assessed through a suspension array system. RESULTS: Fcgamma receptor IIa rs1801274 (FCGR2A) and protein tyrosine phosphatase non-receptor type 2 rs72872125 PTPN2 were statistically different between groups. Patients who had a combination of the presence of FCGR2A and the absence of PTPN2 also had symptoms earlier in life. The combination of genetic polymorphisms and serum level of GM-CSF showed the best diagnostic biomarker to distinguish symptomatic patients as formulated: [0.296*(FCGR2A)] + [-0.788*(PTPN2)] + [-0.107*(GM-CSF)]. CONCLUSION: We have shown that SNPs in inflammation genes might be related to a symptomatic phenotype in CCM. We also demonstrated that a formula based on two of these polymorphisms (FCGR2A+ and PTPN2+) is possibly capable of predicting a symptomatic phenotype during a patient's lifetime.
Sun, Y., et al. (2022). “Cell-free DNA from plasma as a promising alternative for detection of gene mutations in patients with Maffucci syndrome.” Hereditas 159(1): 4. E-Pub 2022/01/20
Maffucci syndrome (MS, OMIM 166000) is an extremely unusual, nonhereditary, multisystemic disorder that is characterized with multiple enchondromas and vascular lesions, most of which are spindle cell hemangiomas. Complications of MS, such as bone deformities and dysfunction caused by enchondromas, usually increase during childhood and adolescence. Malignant transformation of enchondromas and other malignancies are the most severe complications. MS is caused by somatic mosaic IDH1/2 mutations, 65% of which are the IDH1 p.Arg132Cys variant. Due to its rarity, there is no international consensus for the most appropriate treatment option of MS.Here, we report a case of a female patient presenting with multiple enchondromas and spindle cell hemangiomas (SCHs) on bilateral hand and feet diagnosed as MS. A detailed clinical, pathological and genetic diagnosis of MS was rendered. Integrative Genomics Viewer (IGV) visualization of next-generation sequencing (NGS) data revealed the consistent detection of the low-frequency somatic IDH1 p.Arg132Cys mutation between SCH tissue and cystic blood-derived cfDNA. This is the first successful molecular diagnosis of MS complicated with SCH utilizing minimally invasive cfDNA techniques. We suggest that cfDNA sequencing could potentially be used as an alternative, reliable and sensitive method to identify molecular information for genetic diagnosis and for future targeted therapies of MS.
Allen-Rhoades, W., et al. (2022). “Cellular Variant of Kaposiform Lymphangiomatosis: A Report of Three Cases, Expanding the Morphologic and Molecular Genetic Spectrum of this Rare Entity.” Hum Pathol. E-Pub 2022/02/25
Kaposiform lymphangiomatosis (KLA) is a very rare form of generalized lymphatic anomaly, consisting of a diffuse proliferation of abnormal, dilated lymphatics and small fascicles of hemosiderin-laden spindled lymphatic endothelial cells. KLA occurs in children and young adults and may present with multicentric disease, pleural and pericardial effusions, and life-threatening coagulopathy. Genetically, KLA most often harbor somatic activating mutations in NRAS. We recently encountered 3 cases of KLA with cellular features, resembling kaposiform hemangioendothelioma (KHE) and studied their clinicopathologic, radiologic and molecular genetic features. The patients (1 male, 2 females; ages 2 years, 2 months, 4 years) presented with multicentric disease involving skin, soft tissue, bone and spleen, and thrombocytopenia/coagulopathy. Advanced imaging studies confirmed multicentric disease. Biopsies (skin, soft tissue, bone, spleen) demonstrated both conventional KLA and much more cellular foci, consisting of sheets, nodules, glomeruloid structures, and “sieve-like” arrays of lymphatic endothelial cells (positive for CD31 and D2-40). Cellular areas superficially resembled KHE but displayed more epithelioid cytology and lacked surrounding hyaline fibrosis and minute platelet aggregates. Molecular genetic studies demonstrated NRAS c.181C>A p.Q61K (Gln61Lys) in 2 specimens from one patient and HRAS p.A59_Q61delinsGGSIL in another. Two patients were treated with sirolimus; all are currently alive with stable disease. We conclude that cellular morphology in KLA, a previously undescribed feature, does not appear to be associated with clinical features, site of disease, mutation type, response to sirolimus, or outcome. Although cellular KLA may mimic KHE, there are sufficient clinical, morphologic, and genetic differences such that these are likely unrelated diseases.
Swerdlin, R. F., et al. (2022). “Coagulopathy and related complications following sclerotherapy of congenital venous malformations.” Pediatr Blood Cancer: e29610. E-Pub 2022/03/03
BACKGROUND: Congenital venous malformations (VMs) are low-flow vascular anomalies that can cause coagulation abnormalities. This phenomenon, referred to as localized intravascular coagulopathy (LIC), is characterized by elevated D-dimer, hypofibrinogenemia, and/or thrombocytopenia. Increased risk for LIC includes patients with an extensive VM, multifocal VM, and Klippel-Trenaunay and CLOVES syndromes. Peri-procedural anticoagulation has been given to prevent complications from LIC in patients undergoing surgical/interventional procedures; however, the rate of clinically relevant complications from sclerotherapy is largely unknown. The purpose of this study is to describe a single-institution's incidence of LIC in patients with VMs and coagulopathy-related complications following sclerotherapy. DESIGN/METHODS: Retrospective chart review of patients, 0–21 years of age, with VM who underwent sclerotherapy without peri-procedural anticoagulation and had coagulation profiles evaluated within 1 month prior to sclerotherapy. DATA COLLECTED: diagnosis type (high vs. low risk for LIC), coagulation profile (including PT/PTT, D-dimer, fibrinogen, and platelet count), sclerosant used, and post-procedure outcomes. Coagulopathy-related complications included clinically relevant bleeding, deep vein thrombosis (DVT), and pulmonary embolism (PE). RESULTS: N = 138 patients; 59.4% were female. The most common location of VM was the lower extremity (47.8%; 66/138). Of patients with high-risk VMs (29/138 [21%]), 11/29 (37.9%) had laboratory values consistent with LIC, whereas 5% (5/109) of low-risk VMs had LIC. In sum, 492 sclerotherapy procedures were performed with no complications of bleeding, DVT, or PE. CONCLUSION: Patients undergoing sclerotherapy for VM with abnormal coagulation profiles may not require peri-procedural low molecular weight heparin (LMWH). Further studies are needed to precisely define which patients would benefit from anticoagulation.
Khanna, G. (2022). “Editorial Comment: Key Concepts of Complex Lymphatic Malformations.” AJR Am J Roentgenol. 2022/01/27
Rana, I., et al. (2021). “Expanding the spectrum of Gorham Stout disease exploring a single center pediatric case series.” Lymphology 54(4): 182–194. E-Pub 2022/01/25
Gorham-Stout Disease (GSD), also named vanishing bone disease, is an ultrarare condition characterized by progressive osteolysis with intraosseous lymphatic vessel proliferation and bone cortical loss. So far, about 300 cases have been reported. It may occur at any age but more commonly affects children and young adults. The aim of this study is to retrospectively review our internal patient series and to hypothesize a diagnostic-therapeutic protocol for earlier diagnosis and treatment. Clinical datasets from our center were examined to identify all GSD patients for collection and analysis. We identified 9 pediatric cases and performed a retrospective case-series review to examine and document both diagnosis and treatment. We found that delay in diagnosis after first symptoms played a critical role in determining morbidity and that multidisciplinary care is key for proper diagnosis and treatment. Our study provides additional insight to improve the critical challenge of early diagnosis and highlights a multidisciplinary treatment approach for the most appropriate management of patients with rare GSD disease. Although GSD is an ultrarare disease, physicians should keep in mind the main clinical features since neglected cases may result in potentially fatal complications.
Lee, S. Y., et al. (2022). “Genetic and Molecular Determinants of Lymphatic Malformations: Potential Targets for Therapy.” J Dev Biol 10(1). E-Pub 2022/03/01
Lymphatic malformations are fluid-filled congenital defects of lymphatic channels occurring in 1 in 6000 to 16,000 patients. There are various types, and they often exist in conjunction with other congenital anomalies and vascular malformations. Great strides have been made in understanding these malformations in recent years. This review summarize known molecular and embryological precursors for lymphangiogenesis. Gene mutations and dysregulations implicated in pathogenesis of lymphatic malformations are discussed. Finally, we touch on current and developing therapies with special attention on targeted biotherapeutics.
Scherschinski, L., et al. (2022). “Genetics and Emerging Therapies for Brain Arteriovenous Malformations.” World Neurosurg 159: 327–337. E-Pub 2022/03/09
Brain arteriovenous malformations (AVMs) are characterized by a high-pressure, low-resistance vascular nidus created by direct shunting of blood from feeding arteries into arterialized veins, bypassing intervening capillaries. AVMs pose a risk of spontaneous rupture because the vessel walls are continuously exposed to increased shear stress and abnormal flow phenomena, which lead to vessel wall inflammation and distinct morphologic changes. The annual rupture rate is estimated at 2%, and once an AVM ruptures, the risk of rerupture increases 5-fold. The ability of AVMs to grow, regress, recur, and undergo remodeling shows their dynamic nature. Identifying the underlying cellular and molecular pathways of AVMs not only helps us understand their natural physiology but also allows us to directly block vital pathways, thus preventing AVM development and progression. Management of AVMs is challenging and often necessitates a multidisciplinary approach, including neurosurgical, endovascular, and radiosurgical expertise. Because many of these procedures are invasive, carry a risk of inciting hemorrhage, or are controversial, the demand for pharmacologic treatment options is increasing. In this review, we introduce novel findings of cellular and molecular AVM physiology and highlight key signaling mediators that are potential targets for AVM treatment. Furthermore, we give an overview of syndromes associated with hereditary and nonhereditary AVM formation and discuss causative genetic alterations.
Mahajan, P., et al. (2022). “The Genetics of Vascular Birthmarks.” Clin Dermatol. E-Pub 2022/02/20
One in ten infants are born with a vascular birthmark each year. Some vascular birthmarks, such as infantile hemangiomas, are common, while vascular malformations, such as capillary, lymphatic, venous, and arteriovenous malformations, are less so. Diagnosing uncommon vascular birthmarks can be challenging, given the phenotypic heterogeneity and overlap amongst these lesions. Both sporadic and germline variants have been detected in various genes associated with vascular birthmarks. Identification of these genetic variants offers insight into both diagnosis and underlying molecular pathways and can be fundamental in the discovery of novel therapeutic approaches. The PIK3/AKT/mTOR and RAS/MEK/ERK signaling pathways, which mediate cell growth and angiogenesis, are activated secondary to genetic variations in vascular malformations. Somatic variants in TEK (TIE2) and PIK3CA cause venous malformations. Variants in PIK3CA also cause lymphatic malformations as well as a number of overgrowth syndromes associated with vascular anomalies. Variants in GNAQ and GNA11 have been identified in both so-called “congenital” hemangiomas and capillary malformations. RASA1 and EPHB4 variants are associated with capillary malformation-arteriovenous malformation syndrome. This review discusses the genetics of vascular birthmarks including the various phenotypes, genetic variants, pathogenesis, associated syndromes, and new diagnostic techniques.
Mussa, A., et al. (2022). “Genotypes and phenotypes heterogeneity in PIK3CA-related overgrowth spectrum and overlapping conditions: 150 novel patients and systematic review of 1007 patients with PIK3CA pathogenetic variants.” J Med Genet. E-Pub 2022/03/09
BACKGROUND: Postzygotic activating PIK3CA variants cause several phenotypes within the PIK3CA-related overgrowth spectrum (PROS). Variant strength, mosaicism level, specific tissue involvement and overlapping disorders are responsible for disease heterogeneity. We explored these factors in 150 novel patients and in an expanded cohort of 1007 PIK3CA-mutated patients, analysing our new data with previous literature to give a comprehensive picture. METHODS: We performed ultradeep targeted next-generation sequencing (NGS) on DNA from skin biopsy, buccal swab or blood using a panel including phosphatidylinositol 3-kinase/AKT/mammalian target of rapamycin pathway genes and GNAQ, GNA11, RASA1 and TEK. Additionally, 914 patients previously reported were systematically reviewed. RESULTS: 93 of our 150 patients had PIK3CA pathogenetic variants. The merged PROS cohort showed that PIK3CA variants span thorough all gene domains, some were exclusively associated with specific PROS phenotypes: weakly activating variants were associated with central nervous system (CNS) involvement, and strongly activating variants with extra-CNS phenotypes. Among the 57 with a wild-type PIK3CA allele, 11 patients with overgrowth and vascular malformations overlapping PROS had variants in GNAQ, GNA11, RASA1 or TEK. CONCLUSION: We confirm that (1) molecular diagnostic yield increases when multiple tissues are tested and by enriching NGS panels with genes of overlapping ‘vascular’ phenotypes; (2) strongly activating PIK3CA variants are found in affected tissue, rarely in blood: conversely, weakly activating mutations more common in blood; (3) weakly activating variants correlate with CNS involvement, strong variants are more common in cases without; (4) patients with vascular malformations overlapping those of PROS can harbour variants in genes other than PIK3CA.
Sasaki, M., et al. (2022). “Introduction of Mutant GNAQ into Endothelial Cells Induces a Vascular Malformation Phenotype with Therapeutic Response to Imatinib.” Cancers (Basel) 14(2). E-Pub 2022/01/22
GNAQ is mutated in vascular and melanocytic lesions, including vascular malformations and nevi. No in vivo model of GNAQ activation in endothelial cells has previously been described. We introduce mutant GNAQ into a murine endothelial cell line, MS1. The resultant transduced cells exhibit a novel phenotype in vivo, with extensive vasoformative endothelial cells forming aberrant lumens similar to those seen in vascular malformations. ATAC-seq analysis reveals activation of c-Kit in the novel vascular malformations. We demonstrate that c-Kit is expressed in authentic human Sturge-Weber vascular malformations, indicating a novel druggable target for Sturge-Weber syndrome. Since c-Kit is targeted by the FDA-approved drug imatinib, we tested the ability of imatinib on the phenotype of the vascular malformations in vivo. Imatinib treated vascular malformations are significantly smaller and have decreased supporting stromal cells surrounding the lumen. Imatinib may be useful in the treatment of human vascular malformations that express c-Kit, including Sturge-Weber syndrome.
Carli, D., et al. (2021). “Kaposiform hemangioendothelioma further broadens the phenotype of PIK3CA-related overgrowth spectrum.” Clin Genet 100(5): 624–627. E-Pub 2021/08/18
Kaposiform hemangioendothelioma (KHE) is a rare locally aggressive mixed vascular tumor, with typical onset in early childhood and characterized by progressive angio- and lymphangiogenesis. Its etiopathogenesis and molecular bases are still unclear. Here, we report the first case of congenital KHE harboring a PIK3CA mosaic pathogenic variant (c.323G > A, p.Arg108His) in a boy with very subtle PIK3CA-related overgrowth spectrum (PROS) features. This finding provides insights into the pathophysiology of KHE, offering targeted therapeutic options by inhibition of the PI3K/Akt/mTOR pathway. We propose the inclusion of this mixed lymphatic and vascular anomaly within the PROS.
Homayun-Sepehr, N., et al. (2021). “KRAS-driven model of Gorham-Stout disease effectively treated with trametinib.” JCI Insight 6(15). E-Pub 2021/06/23
Gorham-Stout disease (GSD) is a sporadically occurring lymphatic disorder. Patients with GSD develop ectopic lymphatics in bone, gradually lose bone, and can have life-threatening complications, such as chylothorax. The etiology of GSD is poorly understood, and current treatments for this disease are inadequate for most patients. To explore the pathogenesis of GSD, we performed targeted high-throughput sequencing with samples from a patient with GSD and identified an activating somatic mutation in KRAS (p.G12V). To characterize the effect of hyperactive KRAS signaling on lymphatic development, we expressed an active form of KRAS (p.G12D) in murine lymphatics (iLECKras mice). We found that iLECKras mice developed lymphatics in bone, which is a hallmark of GSD. We also found that lymphatic valve development and maintenance was altered in iLECKras mice. Because most iLECKras mice developed chylothorax and died before they had significant bone disease, we analyzed the effect of trametinib (an FDA-approved MEK1/2 inhibitor) on lymphatic valve regression in iLECKras mice. Notably, we found that trametinib suppressed this phenotype in iLECKras mice. Together, our results demonstrate that somatic activating mutations in KRAS can be associated with GSD and reveal that hyperactive KRAS signaling stimulates the formation of lymphatics in bone and impairs the development of lymphatic valves. These findings provide insight into the pathogenesis of GSD and suggest that trametinib could be an effective treatment for GSD.
Snyder, E., et al. (2022). “Lymphatic Anomalies in Children: Update on Imaging Diagnosis, Genetics and Treatment.” AJR Am J Roentgenol. E-Pub 2022/01/20
Lymphatic anomalies comprise a spectrum of disorders ranging from common localized microcystic and macrocystic lymphatic malformations (LMs) to rare complex lymphatic anomalies, including generalized lymphatic anomaly, Kaposiform lymphangiomatosis, central conducting lymphatic anomaly, and Gorham-Stout disease. Imaging diagnosis of cystic LMs is generally straightforward, but complex lymphatic anomalies, particularly those with multi-organ involvement or diffuse disease, may be more challenging to diagnose. Complex lymphatic anomalies are rare but associated with high morbidity. Imaging plays an important role in their diagnosis, and radiologists may be the first clinicians to suggest the diagnosis. Furthermore, radiologists are regularly involved in management given the frequent need for image-guided interventions. For these reasons, it is crucial for radiologists to be familiar with the spectrum of entities comprising complex lymphatic anomalies and their typical imaging findings. In this article, we review the imaging findings of lymphatic anomalies, including LMs and complex lymphatic anomalies. We discuss characteristic imaging findings, multimodality imaging techniques used for evaluation, pearls and pitfalls in diagnosis, and potential complications. We also review recently discovered genetic changes underlying lymphatic anomaly development and the advent of new molecularly targeted therapies.
Venugopal, V. and S. Sumi (2022). “Molecular Biomarkers and Drug Targets in Brain Arteriovenous and Cavernous Malformations: Where Are We?” Stroke 53(1): 279–289. E-Pub 2021/11/18
Vascular malformations of the brain (VMB) comprise abnormal development of blood vessels. A small fraction of VMBs causes hemorrhages with neurological morbidity and risk of mortality in patients. Most often, they are symptomatically silent and are detected at advanced stages of disease progression. The most common forms of VMBs are arteriovenous and cavernous malformations in the brain. Radiopathological features of these diseases are complex with high phenotypic variability. Early detection of these malformations followed by preclusion of severe neurological deficits such as hemorrhage and stroke is crucial in the clinical management of patients with VMBs. The technological advances in high-throughput omics platforms have currently infused a zest in translational research in VMBs. Besides finding novel biomarkers and therapeutic targets, these studies have withal contributed significantly to the understanding of the etiopathogenesis of VMBs. Here we discuss the recent advances in predictive and prognostic biomarker research in sporadic and familial arteriovenous malformations as well as cerebral cavernous malformations. Furthermore, we analyze the clinical applicability of protein and noncoding RNA-based molecular-targeted therapies which may have a potentially key role in disease management.
Wang, K., et al. (2022). “Mutational spectrum of syndromic genes in sporadic brain arteriovenous malformation.” Chin Neurosurg J 8(1): 4. E-Pub 2022/02/26
BACKGROUND: Brain arteriovenous malformations (BAVMs) are abnormal vessels that are apt to rupture, causing life-threatening intracranial hemorrhage (ICH). The estimated prevalence of BAVMs is 0.05% among otherwise healthy individuals. In this study, we aim to investigate the mutational spectrum of syndromic genes in sporadic BAVM. METHODS: We recruited a cohort of 150 patients with BAVM and performed whole-exome sequencing on their peripheral blood DNA. To explore the mutational spectrum of syndromic genes in sporadic brain arteriovenous malformation, we selected six genes according to the Online Mendelian Inheritance in Man (OMIM) and literature. All variants in the six candidate genes were extracted and underwent filtering for qualifying variants. RESULTS: There are a total of four patients with rare variants in hereditary hemorrhagic telangiectasia-related genes. In addition, we identified two patients have the variant of RASA1 gene in our database, which are also rare mutations that are absent from population databases. However, we did not find any patients with GNAQ mutations in our database. CONCLUSIONS: In conclusion, we demonstrated that variants in syndromic vascular malformations play important roles in the etiology of sporadic BAVM.
Seebauer, C. T., et al. (2022). “Non-beta blocker enantiomers of propranolol and atenolol inhibit vasculogenesis in infantile hemangioma.” J Clin Invest 132(3). E-Pub 2021/12/08
Propranolol and atenolol, current therapies for problematic infantile hemangioma (IH), are composed of R(+) and S(-) enantiomers: the R(+) enantiomer is largely devoid of beta blocker activity. We investigated the effect of R(+) enantiomers of propranolol and atenolol on the formation of IH-like blood vessels from hemangioma stem cells (HemSCs) in a murine xenograft model. Both R(+) enantiomers inhibited HemSC vessel formation in vivo. In vitro, similar to R(+) propranolol, both atenolol and its R(+) enantiomer inhibited HemSC to endothelial cell differentiation. As our previous work implicated the transcription factor sex-determining region Y (SRY) box transcription factor 18 (SOX18) in propranolol-mediated inhibition of HemSC to endothelial differentiation, we tested in parallel a known SOX18 small-molecule inhibitor (Sm4) and show that this compound inhibited HemSC vessel formation in vivo with efficacy similar to that seen with the R(+) enantiomers. We next examined how R(+) propranolol alters SOX18 transcriptional activity. Using a suite of biochemical, biophysical, and quantitative molecular imaging assays, we show that R(+) propranolol directly interfered with SOX18 target gene trans-activation, disrupted SOX18-chromatin binding dynamics, and reduced SOX18 dimer formation. We propose that the R(+) enantiomers of widely used beta blockers could be repurposed to increase the efficiency of current IH treatment and lower adverse associated side effects.
Byrne, A. B., et al. (2022). “Pathogenic variants in MDFIC cause recessive central conducting lymphatic anomaly with lymphedema.” Sci Transl Med 14(634): eabm4869. E-Pub 2022/03/03
Central conducting lymphatic anomaly (CCLA), characterized by the dysfunction of core collecting lymphatic vessels including the thoracic duct and cisterna chyli, and presenting as chylothorax, pleural effusions, chylous ascites, and lymphedema, is a severe disorder often resulting in fetal or perinatal demise. Although pathogenic variants in RAS/mitogen activated protein kinase (MAPK) signaling pathway components have been documented in some patients with CCLA, the genetic etiology of the disorder remains uncharacterized in most cases. Here, we identified biallelic pathogenic variants in MDFIC, encoding the MyoD family inhibitor domain containing protein, in seven individuals with CCLA from six independent families. Clinical manifestations of affected fetuses and children included nonimmune hydrops fetalis (NIHF), pleural and pericardial effusions, and lymphedema. Generation of a mouse model of human MDFIC truncation variants revealed that homozygous mutant mice died perinatally exhibiting chylothorax. The lymphatic vasculature of homozygous Mdfic mutant mice was profoundly mispatterned and exhibited major defects in lymphatic vessel valve development. Mechanistically, we determined that MDFIC controls collective cell migration, an important early event during the formation of lymphatic vessel valves, by regulating integrin beta1 activation and the interaction between lymphatic endothelial cells and their surrounding extracellular matrix. Our work identifies MDFIC variants underlying human lymphatic disease and reveals a crucial, previously unrecognized role for MDFIC in the lymphatic vasculature. Ultimately, understanding the genetic and mechanistic basis of CCLA will facilitate the development and implementation of new therapeutic approaches to effectively treat this complex disease.
Twist, J., et al. (2022). “Propranolol therapy for hemangiomas in infants with neonatal abstinence syndrome may produce intolerable side effects.” Pediatr Dermatol. E-Pub 2022/02/19
We report three infants with infantile hemangioma who experienced severe agitation and diarrhea following propranolol administration. Propranolol, a non-selective beta-adrenergic receptor blocker, is the first-line treatment for infantile hemangiomas. All three infants were exposed to opioids in utero and experienced neonatal abstinence syndrome at birth. We hypothesize that chronic opioid exposure in utero may cause protracted upregulation of beta2-adrenergic receptors in the central nervous system, resulting in increased susceptibility to adverse reactions to propranolol.
Ji, Y., et al. (2022). “Sirolimus plus prednisolone vs sirolimus monotherapy for kaposiform hemangioendothelioma: a randomized clinical trial.” Blood 139(11): 1619–1630. E-Pub 2022/01/15
The Kasabach-Merritt phenomenon (KMP) in kaposiform hemangioendothelioma (KHE) is characterized by life-threatening thrombocytopenia and consumptive coagulopathy. This study compared the efficacy and safety of sirolimus plus prednisolone vs sirolimus monotherapy as treatment strategies for KHE with KMP in the largest cohort to date. Participants were randomized to receive either sirolimus in combination with a short course of prednisolone or sirolimus monotherapy for at least 12 months. The primary outcome was defined as achievement of a durable platelet response (platelet count >100 × 109/L) at week 4. Participants completed efficacy assessments 2 years after the initial treatment. At week 4, a durable platelet response was achieved by 35 of 37 patients given sirolimus and prednisolone compared with 24 of 36 patients given sirolimus monotherapy (difference 27.9%; 95% confidence interval, 10.0–44.7). Compared with the sirolimus monotherapy group, the combination treatment group showed improvements in terms of measures of durable platelet responses at all points during the initial 3-week treatment period, median platelet counts during weeks 1 to 4, increased numbers of patients achieving fibrinogen stabilization at week 4, and objective lesion responses at month 12. Patients receiving combination therapy had fewer blood transfusions and a lower total incidence of disease sequelae than patients receiving sirolimus alone. The frequencies of total adverse events and grade 3–4 adverse events during treatment were similar in both groups. The responses seen in patients with KHE with KMP were profound and encouraging, suggesting that sirolimus plus prednisolone should be considered a valid treatment of KHE with KMP. This trial was registered at www.clinicaltrials.gov as #NCT03188068.
El Sissy, F. N., et al. (2022). “Somatic mutational landscape of extracranial arteriovenous malformations and phenotypic correlations.” J Eur Acad Dermatol Venereol. E-Pub 2022/03/04
BACKGROUND: Somatic genetic variants may be the cause of extracranial arteriovenous malformations, but few studies have explored these genetic anomalies, and no genotype-phenotype correlations have been identified. OBJECTIVES: The aim of the study was to characterize the somatic genetic landscape of extracranial arteriovenous malformations and correlate these findings with the phenotypic characteristics of these lesions. METHODS: This study included twenty-three patients with extracranial arteriovenous malformations that were confirmed clinically and treated by surgical resection, and for whom frozen tissue samples were available. Targeted next-generation sequencing analysis of tissues was performed using a gene panel that included vascular disease-related genes and tumour-related genes. RESULTS: We identified a pathogenic variant in 18 out of 23 samples (78.3%). Pathogenic variants were mainly located in MAP2K1 (n = 7) and KRAS (n = 6), and more rarely in BRAF (n = 2) and RASA1 (n = 3). KRAS variants were significantly (P < 0.005) associated with severe extended facial arteriovenous malformations, for which relapse after surgical resection is frequently observed, while MAP2K1 variants were significantly (P < 0.005) associated with less severe, limited arteriovenous malformations located on the lips. CONCLUSIONS: Our study highlights a high prevalence of pathogenic somatic variants, predominantly in MAP2K1 and KRAS, in extracranial arteriovenous malformations. In addition, our study identifies for the first time a correlation between the genotype, clinical severity and angiographic characteristics of extracranial arteriovenous malformations. The RAS/MAPK variants identified in this study are known to be associated with malignant tumours for which targeted therapies have already been developed. Thus, identification of these somatic variants could lead to new therapeutic options to improve the management of patients with extracranial arteriovenous malformations.
Vedmurthy, P., et al. (2022). “Study protocol: retrospectively mining multisite clinical data to presymptomatically predict seizure onset for individual patients with Sturge-Weber.” BMJ Open 12(2): e053103. E-Pub 2022/02/06
INTRODUCTION: Secondary analysis of hospital-hosted clinical data can save time and cost compared with prospective clinical trials for neuroimaging biomarker development. We present such a study for Sturge-Weber syndrome (SWS), a rare neurovascular disorder that affects 1 in 20 000–50 000 newborns. Children with SWS are at risk for developing neurocognitive deficit by school age. A critical period for early intervention is before 2 years of age, but early diagnostic and prognostic biomarkers are lacking. We aim to retrospectively mine clinical data for SWS at two national centres to develop presymptomatic biomarkers. METHODS AND ANALYSIS: We will retrospectively collect clinical, MRI and neurocognitive outcome data for patients with SWS who underwent brain MRI before 2 years of age at two national SWS care centres. Expert review of clinical records and MRI quality control will be used to refine the cohort. The merged multisite data will be used to develop algorithms for abnormality detection, lesion-symptom mapping to identify neural substrate and machine learning to predict individual outcomes (presence or absence of seizures) by 2 years of age. Presymptomatic treatment in 0–2 years and before seizure onset may delay or prevent the onset of seizures by 2 years of age, and thereby improve neurocognitive outcomes. The proposed work, if successful, will be one of the largest and most comprehensive multisite databases for the presymptomatic phase of this rare disease. ETHICS AND DISSEMINATION: This study involves human participants and was approved by Boston Children's Hospital Institutional Review Board: IRB-P00014482 and IRB-P00025916 Johns Hopkins School of Medicine Institutional Review Board: NA_00043846. Participants gave informed consent to participate in the study before taking part. The Institutional Review Boards at Kennedy Krieger Institute and Boston Children's Hospital approval have been obtained at each site to retrospectively study this data. Results will be disseminated by presentations, publication and sharing of algorithms generated.
Bernhard, S. M., et al. (2022). “A systematic review of the safety and efficacy of currently used treatment modalities in the treatment of patients with PIK3CA-related overgrowth spectrum.” J Vasc Surg Venous Lymphat Disord 10(2): 527–538 e522. E-Pub 2021/08/07
BACKGROUND: PIK3CA (activating mutations of the p110alpha subunit of phosphatidylinositol 3-kinases)-related overgrowth spectrums (PROS) include a variety of clinical presentations that are associated with hypertrophy of different parts of the body. We performed a systematic literature review to assess the current treatment options and their efficacy and safety for PROS. METHODS: A literature search was performed in Embase, MEDLINE (Ovid), Web of Science Core Collection, Cochrane Central Register of Controlled Trials, ClinicalTrials.gov, and Google Scholar to retrieve studies on the treatment of hypertrophy in PROS. Randomized controlled trials, cohort studies, and case series with >/ = 10 patients were included in the present review. The titles, abstracts, and full text were assessed by two reviewers independently. The risk of bias was assessed using the Newcastle-Ottawa scale. RESULTS: We included 16 studies of the treatment of hypertrophy in PROS patients, 13 (81.3%) from clinical retrospective studies and 3 (13.7%) from prospective cohort studies. The risk of bias grade was low for 2, medium for 12, and high for 2 studies. Of the 16 studies, 13 reported on surgical treatment and 3 reported pharmacologic treatment using phosphatidylinositol-3-kinase (PI3K)/mammalian target of rapamycin (mTOR) pathway inhibitors in PROS patients. In 3 studies, PROS was defined by a mutation in the PIK3CA gene, and 13 studies relied on a clinical definition of PROS. Surgical therapy was beneficial for a specific subgroup of PROS (macrodactyly). However, little has been reported concerning surgery and the potential benefits for other PROS entities. The reported side effects after surgical therapy were mostly prolonged wound healing or scarring. PI3K/mTOR pathway inhibition was beneficial in patients with PROS by reducing hypertrophy and systemic symptoms. The adverse effects reported included infection, changes in blood count, liver enzymes, and metabolic measures. CONCLUSIONS: Surgery is a locally limited treatment option for specific types of PROS. A promising treatment option for PROS is pharmacologic PIK3CA inhibition. However, the level of evidence on the treatment of overgrowth in PROS patients is limited.
Schrenk, S. and E. Boscolo (2022). “A transcription factor is the target of propranolol treatment in infantile hemangioma.” J Clin Invest 132(3). E-Pub 2022/02/02
Propranolol is a nonselective beta-adrenergic receptor (AR) blocker that has been the first-line therapy for problematic infantile hemangioma (IH), the most frequent childhood vascular tumor. Although IHs are benign and eventually regress spontaneously, at least 15% of patients require treatment. Despite the extensive use of propranolol for IH treatment, its mode of action remains unclear. In this issue of the JCI, Seebauer et al. investigated the cellular and molecular consequences of propranolol treatment on IH vascular tumor formation in a murine model of IH. The efficacy of propranolol was independent of its beta-AR blocker activity and was attributable to the direct targeting of the transcription factor SOX18, which, in turn, reduced hemangioma blood vessel formation. We believe these results will guide clinical translation for the use of more efficient and safer therapies for IH and possibly for other vascular anomalies in which SOX18 plays a role.
Morin, G., et al. (2022). “Treatment of two infants with PIK3CA-related overgrowth spectrum by alpelisib.” J Exp Med 219(3). E-Pub 2022/01/27
PIK3CA-related overgrowth spectrum (PROS) includes rare genetic conditions due to gain-of-function mutations in the PIK3CA gene. There is no approved medical therapy for patients with PROS, and alpelisib, an approved PIK3CA inhibitor in oncology, showed promising results in preclinical models and in patients. Here, we report for the first time the outcome of two infants with PROS having life-threatening conditions treated with alpelisib (25 mg) and monitored with pharmacokinetics. Patient 1 was an 8-mo-old girl with voluminous vascular malformation. Patient 2 was a 9-mo-old boy presenting with asymmetrical body overgrowth and right hemimegalencephaly with West syndrome. After 12 mo of follow-up, alpelisib treatment was associated with improvement in signs and symptoms, morphological lesions and vascular anomalies in the two patients. No adverse events were reported during the study. In this case series, pharmacological inhibition of PIK3CA with low-dose alpelisib was feasible and associated with clinical improvements, including a smaller size of associated complex tissue malformations and good tolerability.
Meyer-Mueller, C., et al. (2022). “Worsening ulceration of infantile hemangioma after initiation or escalation of propranolol.” Pediatr Dermatol. E-Pub 2022/02/19
For infantile hemangiomas (IH) requiring treatment, including those in high-risk locations or in the setting of ulceration, oral propranolol is first-line therapy. Here, we present three cases of infantile hemangioma with worsening ulceration following initiation or escalation of oral propranolol at standard doses.