
Abstract
Background:
Female genital lymphedema (FGL) is a challenging disease, and appropriate preoperative evaluation is crucial before surgical treatments. Computed tomography (CT) is expected useful for FGL evaluation, but little is known. This study aimed to clarify characteristic CT findings of FGL with a case report of CT findings-guided lymphaticovenous anastomosis (LVA).
Methods:
Medical charts of secondary lower extremity lymphedema patients who underwent CT and indocyanine green (ICG) lymphography were reviewed. Genital regions with dermal backflow patterns on ICG lymphography were diagnosed as FGL. Prevalence of characteristic CT findings of lymphedema was compared between genitalia regions with and without FGL. A case of genital lymphedema treated with LVA under the guidance of CT findings was presented.
Results:
A total of 51 patients (32 with FGL, and 19 without FGL) were included in this study. Genital ICG included stages 0/I/II/III/IV/V in 19 (37.3%)/5 (9.8%)/11 (21.6%)/9 (17.6%)/7 (13.7%)/0 (0%) cases, respectively. Characteristic CT findings included thick skin in 14 (27.5%), thick fascia in 17 (33.3%), high density of the superficial fat in 11 (21.6%), high density of the deep fat in 13 (25.5%), fluid collection in 8 (15.7%), detectable inguinal lymph node in 42 (82.4%), and honeycomb appearance in 7 regions (13.7%). Between genital regions with and without FGL, there were statistically significant differences in all the characteristic CT findings (p < 0.05).
Conclusions:
Characteristic CT findings of secondary FGL were identified. Preoperative CT evaluation may be useful for selecting appropriate LVA sites for optimal results.
Introduction
Female genital lymphedema (FGL), a part of lower hemi-body lymphedema, is a chronic condition significantly affecting gynecological cancer survivors’ quality of life.1,2 Supermicrosurgical lymphaticovenous anastomosis (LVA) has been reported to be useful for the treatment of FGL, but its therapeutic efficacy is inconsistent because of the lack of optimal preoperative evaluation methods. 2 Evaluation of lymphedema includes various modalities such as lymphoscintigraphy (LSG), magnetic resonance imaging (MRI), indocyanine green (ICG) lymphography, and computed tomography (CT).3–6 LSG is a gold standard for lymphedema evaluation, but it is difficult to evaluate small regions such as the genitalia. 5 MRI allows three-dimensional evaluation of fluid accumulation and fat deposition but requires higher cost and longer time for image acquisition. 6 ICG lymphography is highly sensitive and specific to detect abnormal lymph circulation, which allows pathophysiological severity staging and prediction of prognosis, but has disadvantages of risks related ICG injection and the need for a near-infrared camera for visualization.7,8
Although unable to visualize lymph circulation, CT allows the precise three-dimensional visualization of the anatomical structures and is one of the most common modalities for cancer follow-up. Therefore, in most pelvic cancer survivors, CT is routinely used to follow oncological conditions, which can be also used for the evaluation of FGL without additional procedures. There are previous studies reporting the usefulness of CT images for the diagnosis of lower extremity lymphedema (LEL). 9 Although CT is expected to be useful for the evaluation of FGL, little is known regarding characteristic CT findings of FGL or clinical reports of CT findings applied for surgical treatments of FGL.
This study aimed to clarify characteristic CT findings of secondary FGL by comparing clinical and genital image findings in secondary LEL patients.
Patients and Methods
Medical charts of secondary LEL patients who underwent CT and ICG lymphography from January 2018 to December 2020 were reviewed. Female patients were included to simplify the interpretation of CT and ICG lymphographic findings of the genitalia. Male patients or patients with a past history of genital surgery other than pelvic cancer treatments were excluded. ICG lymphography was performed to evaluate FGL as previously reported. 10 Based on ICG lymphography findings, genital ICG stage was determined (Table 1 and Fig. 1); ICG stage 0 was defined as no FGL (control), whereas ICG stages I–V were defined as FGL.
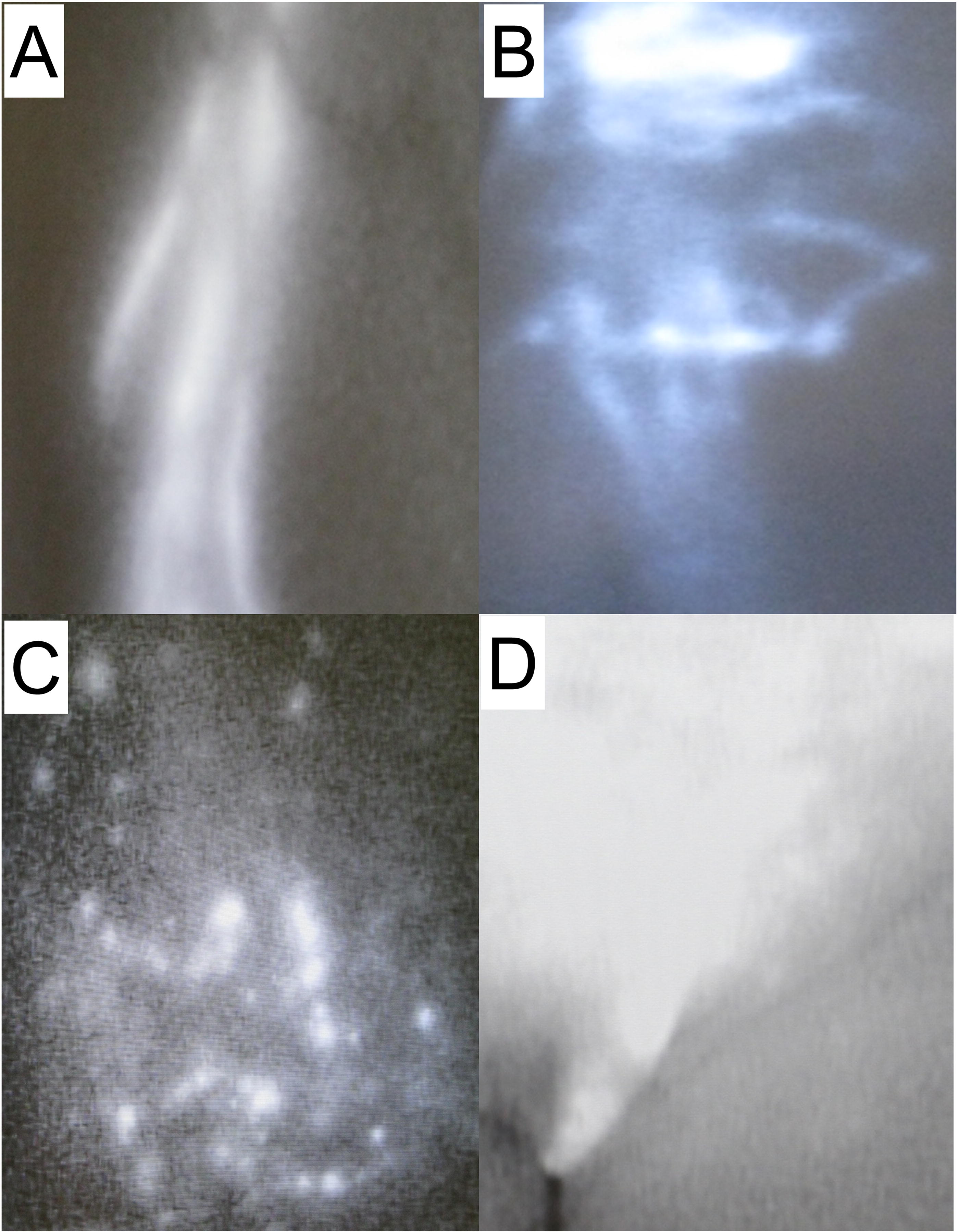
Representative indocyanine green findings; Linear
Indocyanine Green Lymphography Stage for Genital Indocyanine Green Stage
The genitalia is divided into three regions; the lower abdomen, the labia majora, and the labia minora.
ICG, indocyanine green; GL, genital lymphedema.
A CT scan was ordered by an outpatient plastic surgeon to exclude venous or other edema-related diseases in this cohort. CT scan was performed as previously reported; a 16- or 64-slice multidetector CT system (Sensation16, Siemens, Erlangen, Germany) was used for enhanced CT. Scanning parameters were as follows: detector collimation, 0.75 9 16 mm to 0.6 9 64 mm; pitch, 1–1.5; slice thickness, 5 mm; reconstruction interval, 0.7–1.5 mm; X-ray tube voltage, 120 kVp in Brilliance 64 and 100 kVp in the other machines; and effective tube current, 150 mAs. Axial CT images at the upper 5 cm of iliac crest to under 5 cm of ischium were used for GL evaluation. According to previous reports of characteristic CT findings of LEL, the following CT findings were evaluated: thick skin, thick fascia, high density of superficial fat, high density of deep fat, fluid collection, detectable inguinal lymph node detection, and honeycomb appearance (Fig. 2A–G). Thick skin represented thickened dermis of the genital region, thick fascia thickened fascia of the rectus abdominis muscle, high density of the superficial fat/high density of the deep fat increase of genital superficial/deep fat density above/below the superficial fascia, fluid collection homogenous patchy soft tissue opacity of fluid attenuation grossly without distinguishable septa abutting the muscle fascia, detectable inguinal lymph node existence of detectable inguinal lymph nodes, and honeycomb appearance thickened interstitial tissue in the subcutaneous layer crossing each other appearing as polygonal-shaped fat attenuation with peripheral septa-like structures.
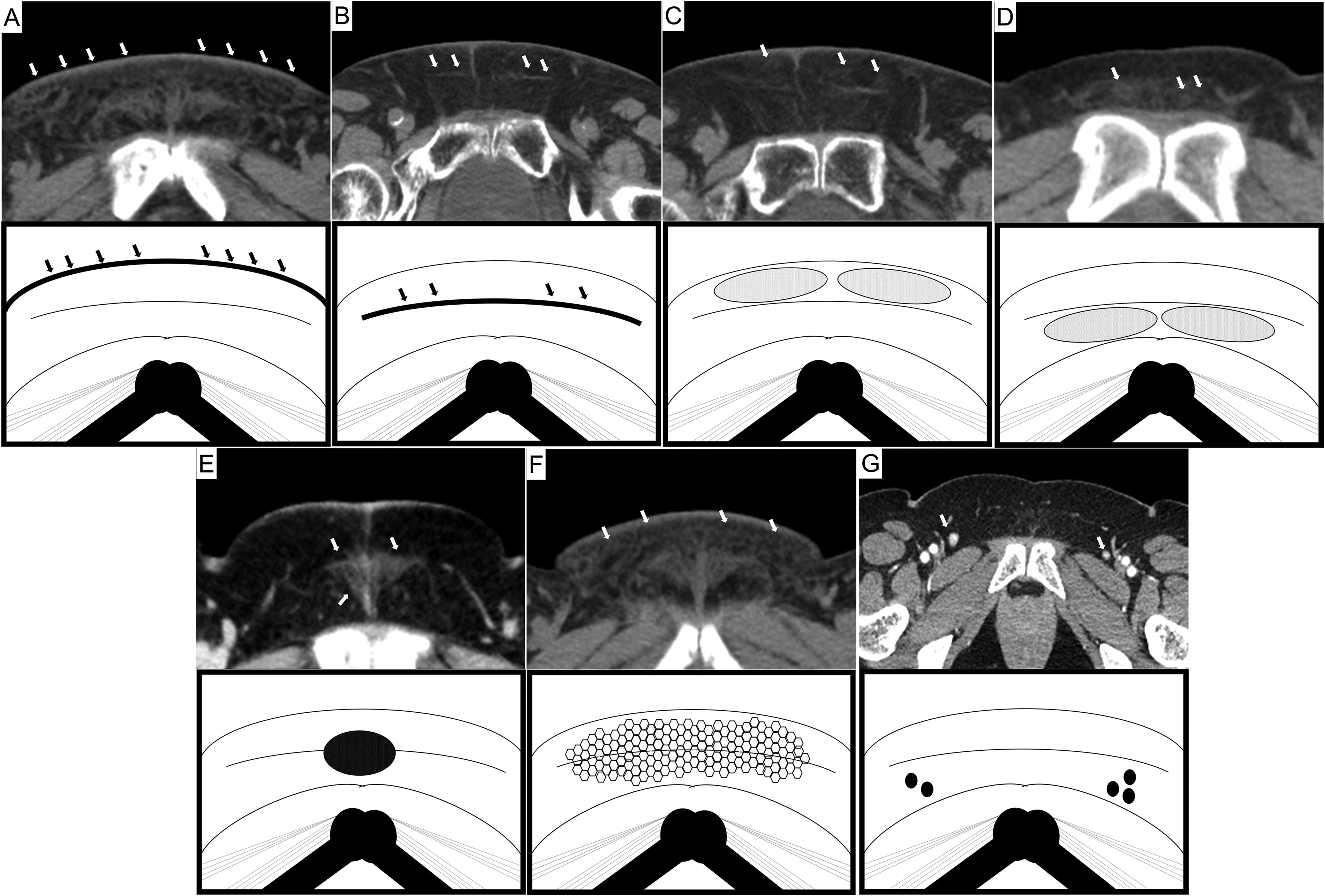
Characteristic computed tomography findings of genital lymphedema; thick skin
Collected data included age, body mass index (BMI), past medical history, etiology of lymphedema, duration of lymphedema, history of lymphedema treatment, LEL index, and findings of CT and ICG lymphography. The prevalence of each genital CT finding was compared between cases with and without FGL by a physician (nonplastic surgeon) who was not involved in the lymphedema clinic. Statistical analyses were done using the chi-square test and Fisher exact probability test. A p value of <0.05 was set as statistical significance. This retrospective observational study was approved by the institutions’ ethical review board.
Results
A total of 51 patients (32 patients with FGL and 19 patients without FGL) were included in this study. Patients’ ages ranged from 34 to 77 years (average, 54.8 years) and BMI ranged from 16.8 to 35.5 kg/m2 (average, 22.95 kg/m2). Past medical history included cellulitis in nine cases (17.6%), diabetes in two cases (3.9%), and deep vein thrombosis in one case (1.9%). All patients were associated with LEL: unilateral LEL in 16 cases (31.4%) and bilateral LEL in 35 cases (68.6%). Etiology of lymphedema included uterine cervical cancer in 30 cases (58.8%), endometrial cancer in 12 cases (23.5%), ovarian cancer in five cases (9.8%), rectal cancer in one (2.0%), peritoneal cancer in one (2.0%), bladder cancer in one case (2.0%), and breast cancer in one (2.0%); systemic metastasis of breast cancer caused secondary lymphedema of the lower hemi-body. Duration of lymphedema ranged from 0 to 240 months (average, 62.2 months). Lymphedema treatments included compression garments in 29 cases (56.9%), manual lymph drainage in three cases (5.9%), and lower extremity LVA in one case (2.0%). The LEL index ranged from 209 to 371 (average, 259.5). ICG lymphography revealed that the genital ICG stages were stage 0 in 19 cases (37.3%), stage I in five cases (9.8%), stage II in 11 cases (21.6%), stage III in nine cases (17.6%), and stage IV in seven cases (13.7%); there was no case of ICG stage V. CT showed positive for thick skin in 14 cases (27.5%), thick fascia in 17 cases (33.3%), high density of the superficial fat in 11 cases (21.6%), high density of the deep fat in 13 cases (25.5%), fluid collection in 8 cases (15.7%), detectable inguinal lymph node in 42 cases (82.4%), and honeycomb appearance in 7 cases (13.7%) (Table 2).
Patient Characteristics
BMI, body mass index; DVT, deep vein thrombosis; LEL, lower extremity lymphedema; ICG, indocyanine green.
Between cases with (32) and without (19) FGL, there were statistically significant differences in thick skin (n = 14 vs. 0; 43.75% vs. 0%, p = 0.0007), thick fascia (n = 17 vs. 2; 53.13% vs. 10.53%, p <= 0.0027), high density of superficial fat (n = 11 vs. 0; 34.38% vs. 0%, p = 0.0037), high density of deep fat (n = 13 vs. 0 40.63% vs. 0%, p = 0.0008), fluid collection (n = 8 vs. 0; 25% vs. 0%, p = 0.0192), detectable inguinal lymph node (n = 23 vs. 19; 71.9% vs. 100%, p = 0.0183), and honeycomb appearance (n = 7 vs. 0; 21.88% vs. 0%, p = 0.037) (Fig. 3A–G).
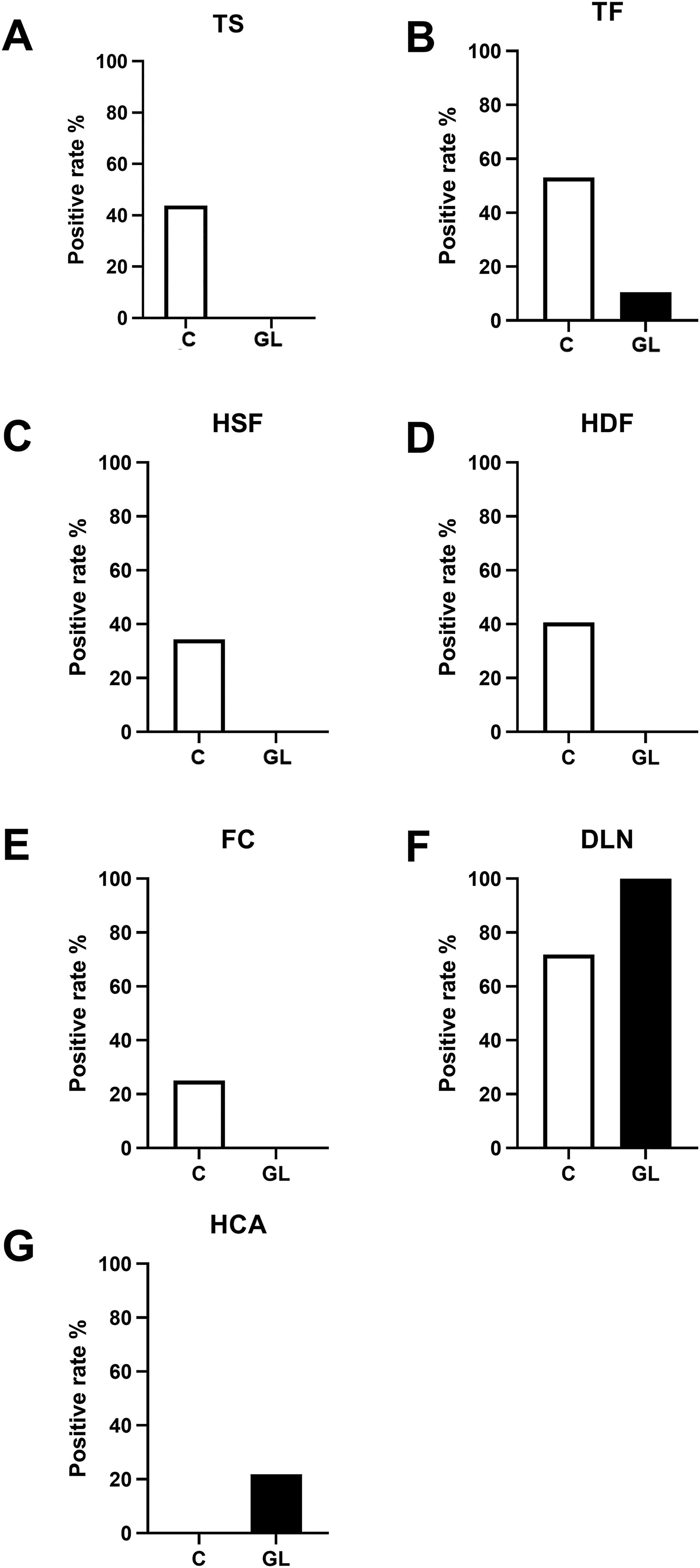
Comparisons of representative computed tomography images in female genital lymphedema (FGL) and control groups. Between cases with and without FGL, there were statistically significant differences in thick skin (TS; 5.3% vs. 40.6%, p = 0.006)
Discussion
This study clarified the characteristic CT findings of FGL, including thick skin, thick fascia, high density of superficial fat, high density of deep fat, detectable inguinal lymph node, fluid collection, and honeycomb appearance. These CT findings of FGL were compatible with those reported in previous studies on LEL.11,12 Previous studies reported various factors associated with FGL, such as past history of lymphocyst or radiation and LEL.2,4,10 However, this study revealed that the CT findings were strongly associated with pathophysiological FGL evaluation based on ICG lymphography findings rather than other factors such as lymphedematous volume of the lower extremity and LEL index. In FGL, lymph fluid is retained in the soft tissue, especially in the dermis and adipose tissue above the muscle. Pathological progression of secondary FGL is considered to result from lymph flow obstruction in the pelvic region and to extend distally toward the genitalia via the inguinal lymph nodes’ dysfunction. 2 When the inguinal lymph nodes become dysfunctional, they are fibrotic and small in size, leading to the CT finding of low detectable inguinal lymph node rate in the FGL group. Lymph fluid is predominantly retained around the deep fat layer, and the retention also extends to the deep fascia and the dermis, which are shown as fluid collection, high density of deep fat, honeycomb appearance, thick fascia, high density of superficial fat, and thick skin on CT. In this study cohort, thick fascia/high density of superficial fat and high density of deep fat/fluid collection/honeycomb appearance were associated with high sensitivity and specificity, respectively; these findings are useful for the diagnosis of FGL based on CT. In particular, honeycomb appearance was observed only in severe cases, 0 in stages I and II, 11.1% in stage III, and 86% in stage IV. To the best of our knowledge, this is the first study to comprehensively analyze the CT features of FGL.
As in this study cohort, most secondary FGL patients have a past history of pelvic malignancy and undergo CT scans periodically as postoperative surveillance. 11 The follow-up CT scan always includes the genital region, which allows screening and evaluation of secondary FGL without additional imaging modality. 13 When the follow-up CT scan shows characteristic FGL findings revealed by this study, further lymph flow evaluations, such as ICG lymphography and LSG, should be considered for accurate diagnosis and severity evaluation of FGL to consider the indication of FGL treatments.2,11,14–16 As FGL is frequently overlooked by a patient and even by medical staffs who care lymphedema and life-long interventions are required once developed, follow-up CT images should be used for screening of FGL following pelvic cancer treatments regardless of subjective genital symptoms.1,13
Another major potential clinical application of CT in FGL management is preoperative evaluation for lymphedema surgery. Although LSG is a gold standard for lymphedema evaluation, its resolution is low not enough to detect early abnormal circulation of a small region such as the genitalia; FGL may be underdiagnosed solely based on LSG findings.5,8,10 Therefore, CT findings, which have been performed during cancer follow-up, can be useful to detect subclinical FG for considering indications of lymphedema surgeries such as LVA. Generally, simple resection and laser therapy are selected as treatments for FGL, but LVA is a challenging option. 17 Even in clinically evident FGL cases, CT findings can be used to consider optimal incision sites for LVA. LVA should be performed where CT shows most lymphedematous findings and another lymph flow imaging such as ICG lymphography shows patent lymph flows. Although only a single case was presented in this study, CT findings may have the potential to be useful for preoperative evaluation for FGL.
A major drawback of CT is artifacts due to artificial materials such as metal implants. 18 In particular, metallic orthopedic implants may hamper the visualization of the genital soft tissues. 19 Although there was no such case included in this study, a patient who underwent total hip arthroplasty would be inappropriate for CT evaluation of FGL. Another concern is exposure to ionized radiation in CT scans. Although not associated with additional ionized radiation exposure in pelvic cancer survivors who undergo routine follow-up CT, CT scan requires additional radiation exposure in primary lymphedema cases where CT is not routinely performed. Therefore, CT evaluation of FGL is the most suitable for patients with a past history of pelvic cancer treatments.
This study has several limitations. The study included only Japanese secondary lymphedema patients with a small sample size. It is yet to be clarified whether the characteristic CT findings, demonstrated in this study, are useful for primary lymphedema cases or other ethnic groups. As the study is a retrospective observational one without follow-up, further studies are required to confirm thresholds to diagnose lymphedema and the usefulness of CT for severity evaluation and prognosis prediction of FGL.
Conclusions
Characteristic CT findings of secondary FGL were identified. Thick fascia/high density of superficial fat and high density of deep fat/fluid collection/honeycomb appearance showed high sensitivity and specificity for diagnosis of FGL. Further studies are required to confirm the usefulness of the CT findings to evaluate the severity and predict prognosis of FGL.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.