
Abstract
Background:
Chylous reflux (CR) in primary lymphedema (PL) of the lower extremities is rare and requires particular diagnostic procedures. This study aimed to determine clinical and lymphoscintigraphic traits for efficient screening.
Methods and Results:
Pediatric patients with PL of lower extremities treated in our institution between January 2020 and December 2023 were reviewed. The medical history, lymphoscintigraphy, non-contrast MR lymphography, and direct lymphangiography were analyzed. Lymphoscintigraphic visual patterns were classified to detect CR. Patients with CR showed significantly higher proportions of childhood symptom onset (65.63% vs. 25.19%, p < 0.01), genital lymphedema (62.50% vs. 19.26%, p < 0.01), and proximal-to-distal swelling (31.25% vs. 8.89%, p < 0.01). Eight patients without skin lesions had milk discharge after acupuncture or skin breakdown. Pattern 4 shows diffused dermal backflow of the leg and an absence of superficial lymphatic drainage, or normal initial cephalad flow with subsequent reflux of tracer into the affected limb. CR showed significantly higher percentages of pattern 4 (87.50% vs. 12.59%, p < 0.01), normal/widened iliac lymphatics (78.13% vs. 11.11%, p < 0.01), and thigh/calf outlining (87.50% vs. 29.63%, p < 0.01). Genital swelling preceding limb swelling and genital radioactivity were more common in the CR group.
Conclusions:
CR tends to occur in childhood initially, begin centrally and progress distally, and involve genitals prior to lower extremities. Milk discharge after acupuncture or skin breakdown is important for screening CR without chylous vesicles. The patterns with typical “profiling of the leg” and normal or widened iliac lymphatic trunks strongly correlate with CR. Genital lymphedema with increased radioactivity indicates CR.
Introduction
Primary lymphoedema (PL) includes sporadic, hereditary, and syndromic forms. The prevalence of PL was reported as 1.15 per 100,000 patients in the pediatric population. 1 PL has characteristic morphological patterns, which are classified as aplasia/hypoplasia (89%) and hyperplasia (including mega lymphatics) (11%).2–4 Hyperplastic iliac and inguinal lymphatic trunks are more numerous or greater in diameter than normal,3,5 which suggests chylous reflux (CR). In 1964, Kinmonth et al. defined chylous reflux syndrome I, which occurs in 14% of patients with primary lymphoedema. 6 Primary CR syndrome can manifest as lymphedema, chylorrhea via lymphocutaneous fistulae, or chylous vaginal leakage.7–9 The lymphoedema associated with CR is rare but complicated and calls for particular diagnostic procedures to ensure appropriate management. 2 Medical practitioners do not commonly identify it. This could result in a protracted interval between the start of symptoms and the accurate diagnosis.
How to screen the patients by history and visual pattern for confirmatory tests (unilateral pedal lymphoscintigraphy, non-contrast MR lymphography (MRL), and trans-pedal lymphangiography) is a problem yet to be elucidated. We present our single-institution study to describe, analyze, and determine the clinical and lymphoscintigraphic features indicating CR in pediatric PL of the lower extremities.
Methods and Materials
Patients
A retrospective observational study was conducted after the institution review board approval. The pediatric patients with PL were admitted to the Department of Lymphatic Surgery, Capital Medical University Affiliated Beijing Shijitan Hospital, from January 2020 to December 2023. The following inclusive criteria were used: 1) primary lymphoedema of lower extremities was diagnosed based on clinical characteristics, lymphoscintigraphy, and MR; 2) the age is ≤18 years. The following exclusive criteria were used: 1) the patients had chylothorax, chylous ascites, chylopericardium, or intestinal lymphangiectasia; 2) non-contrast MRL was not implemented.
We collected data including demographics, clinical presentations, laboratory data, and lymphatic imaging results. They all underwent bipedal 99mTc-DX (Beijing Atomic Technology Co., Ltd.) lymphoscintigraphy (injected into the subcutaneous tissue of the first and fourth interdigital space) 10 and non-contrast MRL. When CR was suggested, unilateral pedal lymphoscintigraphy and trans-pedal lymphangiography with lipiodol (Guerbet, France) were done for diagnosis.
Classification of age at onset
Definition of onset based on developmental age: infancy (birth to 12 months), childhood (1–8 years for girls and 1–9 years for boys), adolescence (9–18 years for female subjects and 10–18 years for male subjects). 11 Age of onset was defined in years and, if the symptoms or signs present before 12 months of age, it was recorded as 0.
Lymphoscintigraphy
Bipedal lymphoscintigraphy is the most frequently used for lymphedema. We classified PL into four visual patterns (Fig. 1) according to visualization of superficial lymphatic vessels in the lower limb, visualization of iliac lymphatic trunks, and accumulation of tracer activity in the thighs and lower legs creating an outline of the leg. In the image of pattern 1 and 2, there is no “profiling of the leg”. But pattern 2 has the drainage of superficial lymphatic vessels and iliac lymphatic trunks. In the image of pattern 3 and 4, there is “profiling of the leg.” Concurrently, pattern 4 has the drainage of iliac lymphatic trunks.
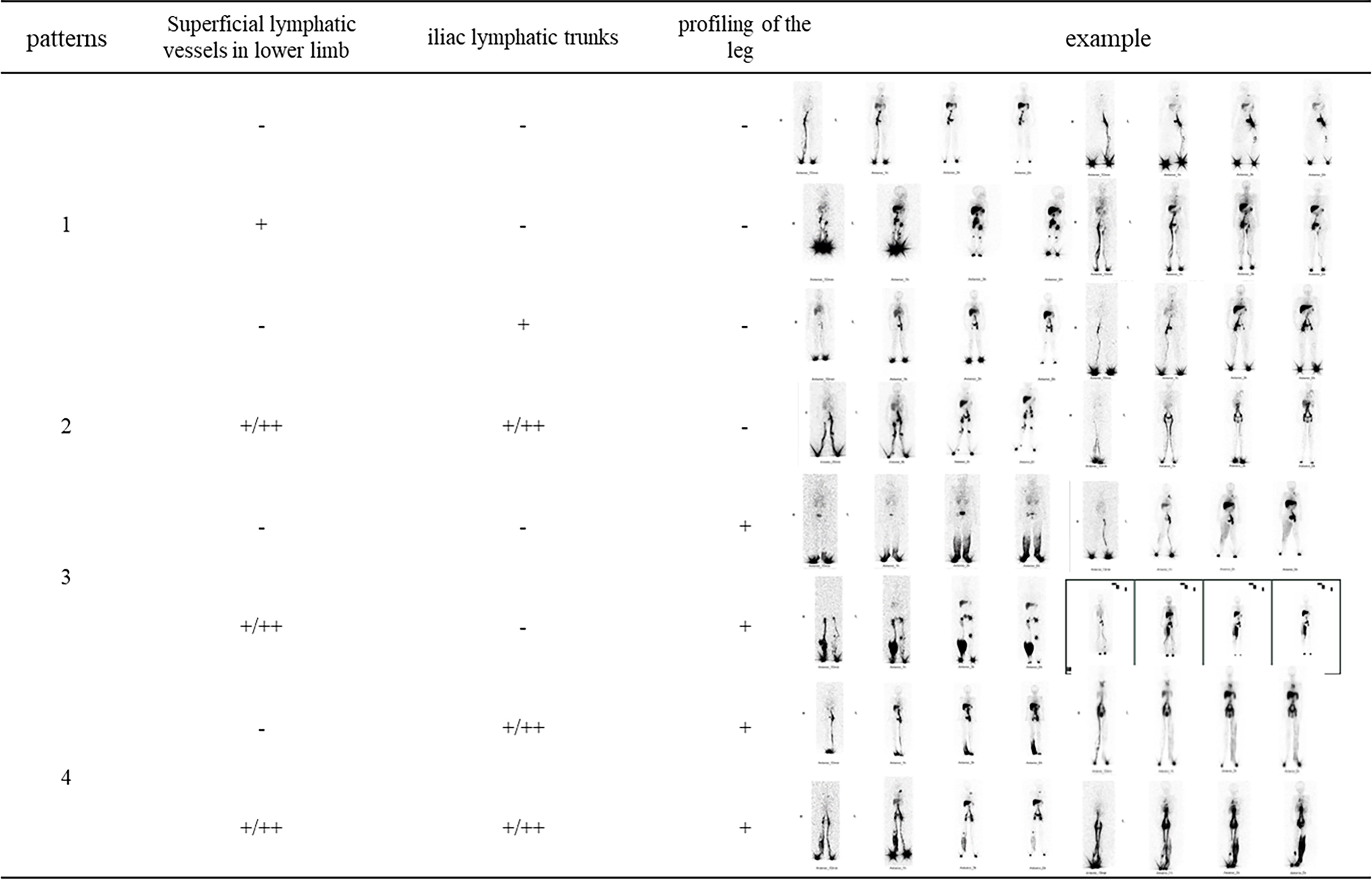
Characteristic visual patterns of lymphoscintigraphy in pediatric primary lymphedema. Pattern 1 and 2 have no “profiling of the leg.” But pattern 2 has the drainage of superficial lymphatic vessels and iliac lymphatic trunks. Patterns 3 and 4 have “profiling of the leg.” But pattern 4 has the drainage of iliac lymphatic trunks.
Statistics
Descriptive statistics [Mean (standard deviations), median (min-max, interquartile range), number and proportions] were used to give an overview of the characteristics of patients. The nonparametric Mann–Whitney U test was used. All statistical analyses were performed using IBM SPSS Statistics for Windows (version 22.0, IBM). A two-tailed value of p < 0.01 was significant.
Results
A total of 167 cases were enrolled (Table 1). There were 19.2% cases (n = 32, male 23 and female 9) who demonstrated PL of the lower limb due to CR. The other 80.8% of cases (n = 135, male 61 and female 74) had no evidence of CR. The median age at onset of patients with CR is 7 (0–14, 4) years, and the mean is 6.88 (SD = 4.09) years. The median age at onset of patients without CR is 6 (0–17, 12) years and the mean is 6.43 (SD = 5.79) years. The median age at onset between the two groups had no significant difference. Compared to group without CR, the proportion of patients whose swelling symptom first appeared in childhood is significantly higher (p < 0.01) (65.63%, 21/32 vs. 25.19%, 34/135), the proportion of patients with genital lymphedema is significantly higher (p < 0.01) (62.50%, 20/32 vs. 19.26%, 26/135), and the proportion of chronic swelling with proximal to distal enlargement is significantly higher (p < 0.01) (31.25%, 10/32 vs. 8.89%, 12/135) in group with CR.
Overview of Characteristics of the Patients
For categorical data, number (%) is provided; for continuous data, median (min-max, interquartile range) is provided.
Typical chylous vesicles or milk oozing was only found in parts of lymphedema associated with CR. Seven patients had chylous vesicles and milk oozing in the lower extremities or genitals. Another eight patients without skin lesions had milk discharge after acupuncture or skin breakdown. Vesicles appeared at the thigh (two cases), shank (one case), foot (one case), or genitals (six cases). Chylous vesicles and milk oozing may occur after edema many years later.
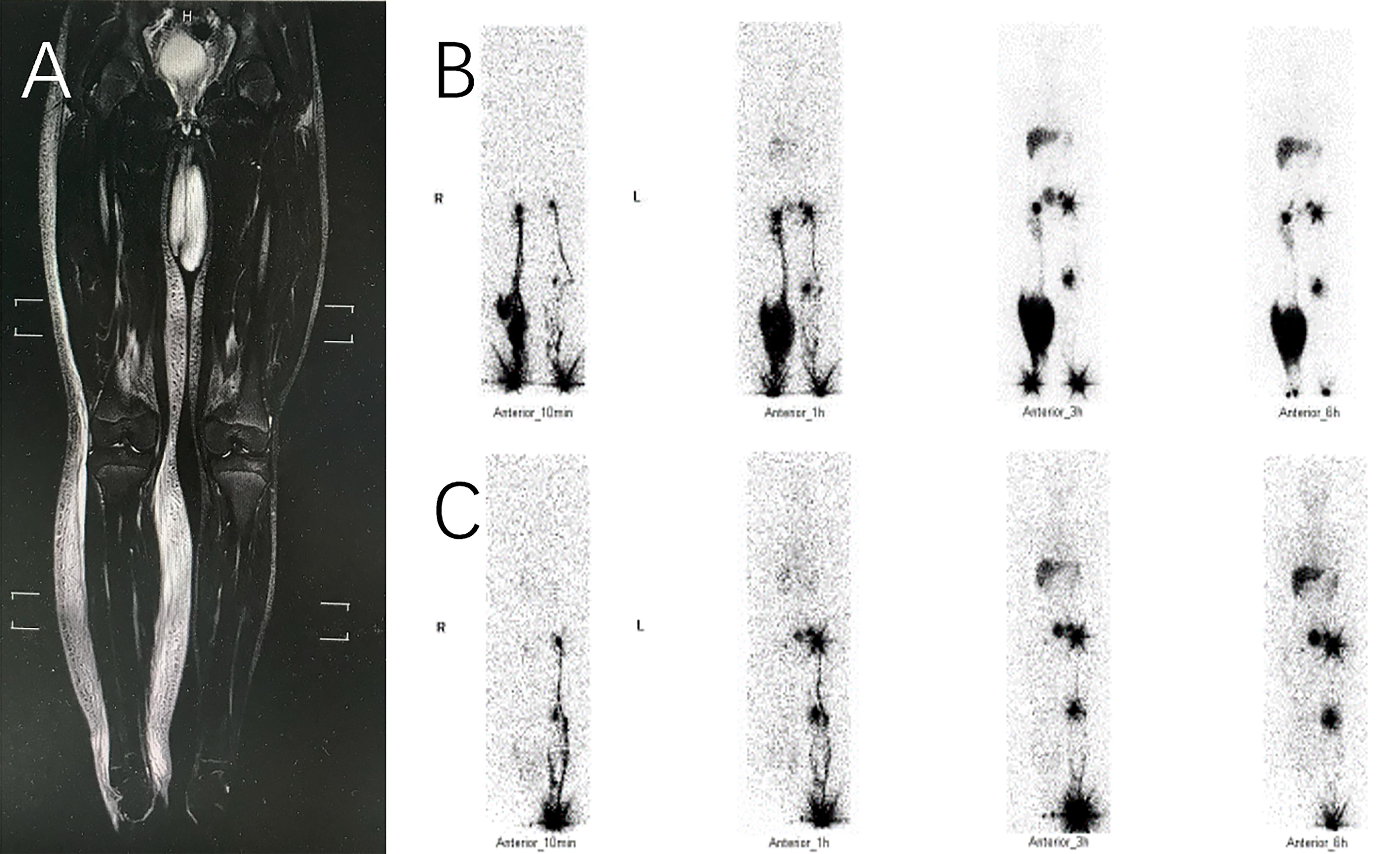
In bipedal lymphoscintigraphy, CR only presented as visual pattern 2 (four cases) and 4 (twenty-eight cases). The patients with pattern 2 had widened iliac lymphatic trunks and MRL showed hyperplastic and malformed lymphatic vessels in the pelvic cavity. The patients with pattern 4 had diffused dermal backflow of the leg and an absence of superficial lymphatic drainage, or normal initial cephalad flow with subsequent reflux of tracer into the affected limb (same as the characteristic lymphoscintigraphic imaging of lymphedema-distichiasis syndrome reported by Sarica et al.). (Fig. 2) Compared to group without CR, the proportion of pattern 4 is significantly higher (p < 0.01) (87.50%, 28/32 vs. 12.59%, 17/135), the proportion of normal or widened iliac lymphatic trunks is significantly higher (p < 0.01) (78.13%, 25/32 vs. 11.11%, 15/135), the proportion of creating an outline of the thigh or calf is significantly higher (p < 0.01) (87.50%, 28/32 vs. 29.63%, 40/135). In the subgroup of creating an outline of the leg, the proportion of normal or widened iliac lymphatic trunks in patients with CR is significantly higher (p < 0.01) (75.00%, 21/28 vs. 15.00%, 6/40). Moreover, the group of non-chylous reflux presented an absence or diminished drainage of superficial lymphatic vessels in the lower extremities.
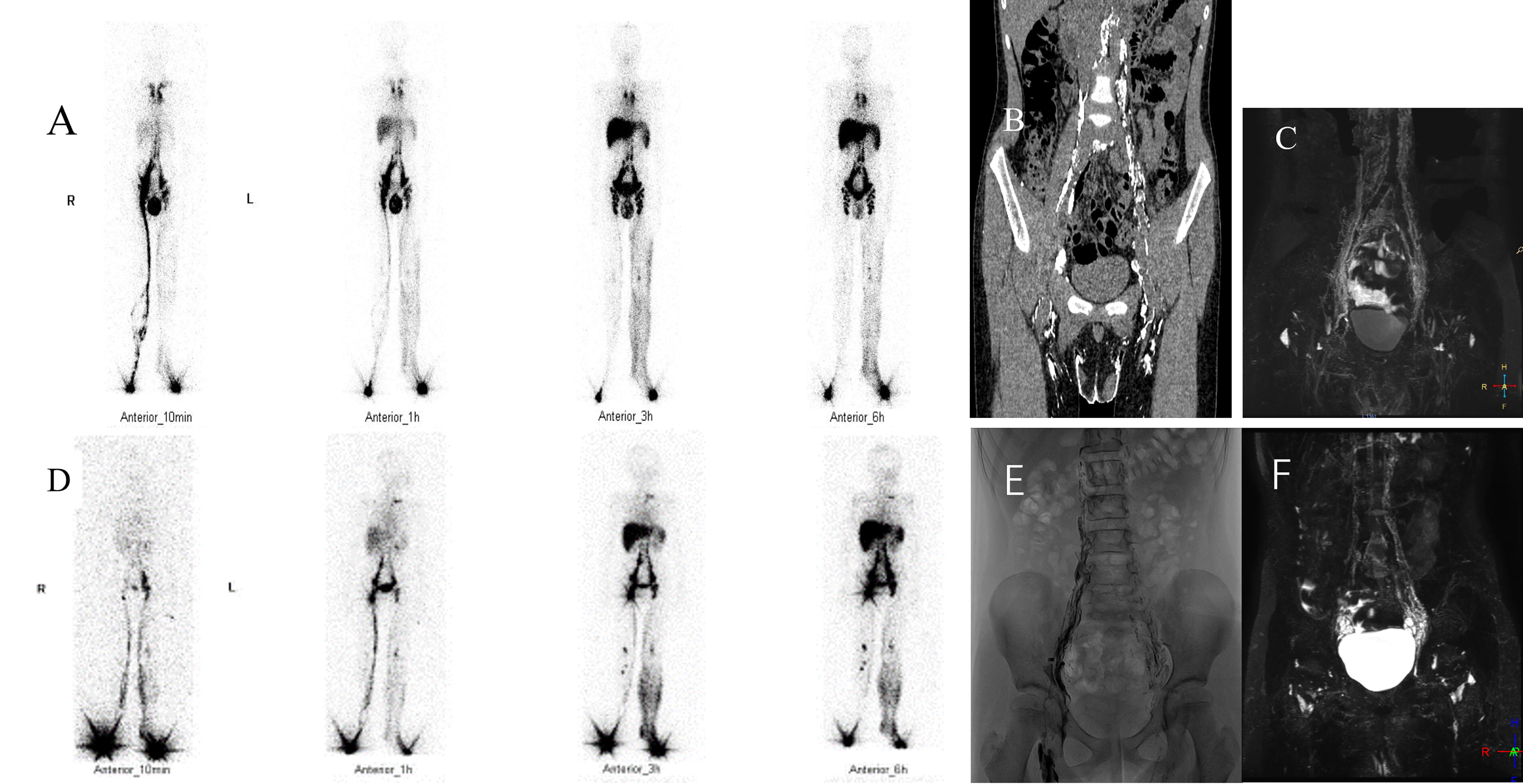
Two cases with chylous reflux presented as visual pattern 4. One case
In the subgroup with genitals involved (Table 2), the percentage of genital swelling before the leg is significantly higher in patients with CR (p < 0.01). In contrast, the percentage of synchronous onset is significantly higher in patients without CR (p < 0.01). All patients with CR had increased radioactivity of the iliac lymphatic trunks and genitals. However, 18.52% (5/27) of cases without CR had genital radioactivity but no lumbar and iliac trunk reflux (Fig. 3).
Patients without chylous reflux had the right leg and scrotum involved
Differentiation of Subgroups with Genital Lymphedema
There were special cases without CR (Fig. 4). The patients showed abnormal lymphoscintigraphy or MRL similar to the CR.
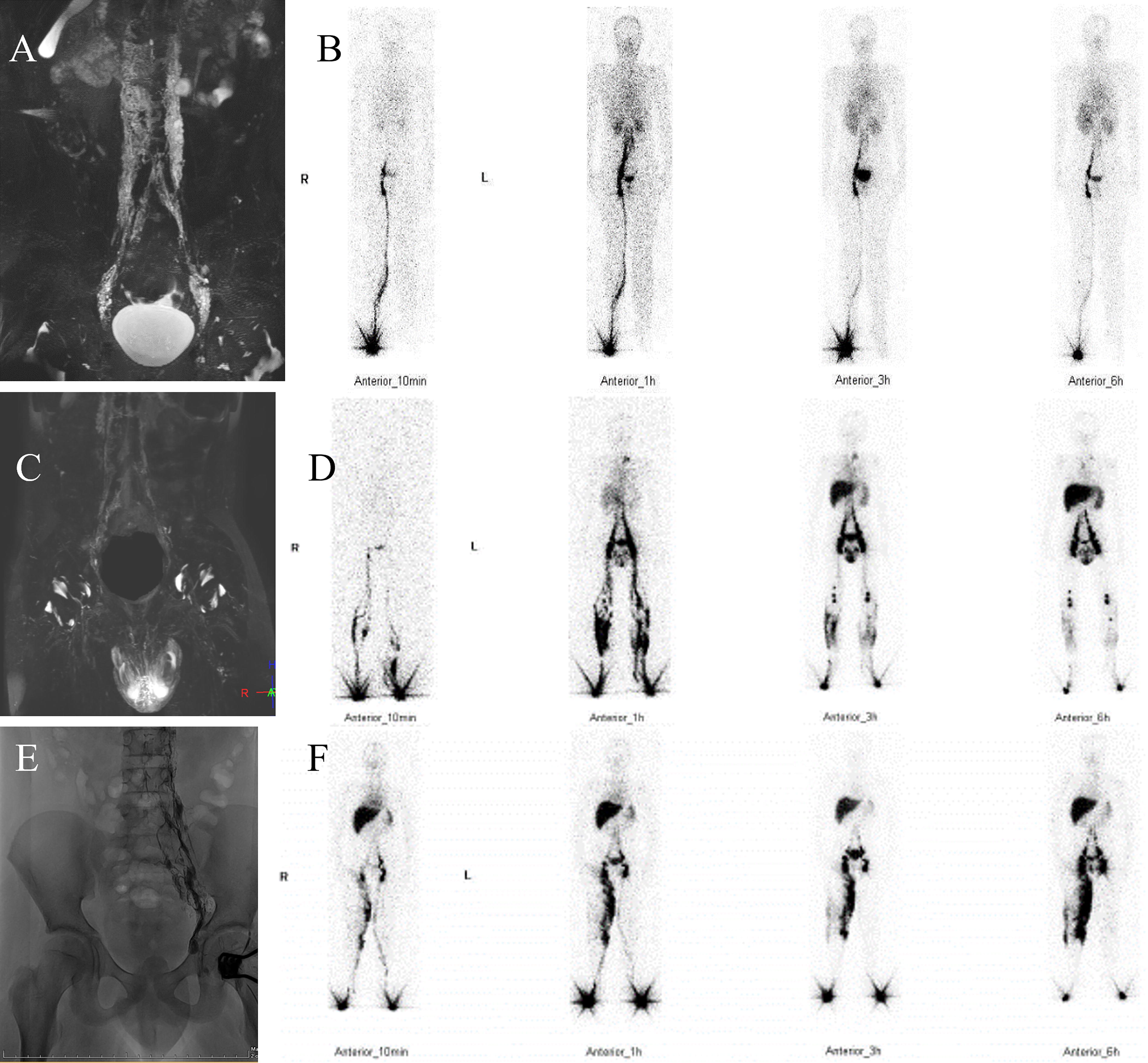
Special cases without chylous reflux. One case had extensive retroperitoneal lymphatic dysplasia
Discussion
CR and non-chylous lymph reflux should be discriminated against. Early recognition and early rational interventions (e.g., low-fat diets and medium-chain triglycerides supplements) improve the prognosis of CR. In part of China, only lymphoscintigraphy can be executed as the primary investigation for swelling extremities. Clarifying the clinical and lymphoscintigraphic differences between CR and hypoplastic PL would be of great benefit for screening.
Some diagnostic features of CR of lower extremities and/or genitals were summarized. Classical symptoms and signs include chylous vesicles in the perineum, scrotum, labia, or legs and intermittent or continuous leakage of milky fluid.9,12 Abnormal lymphoscintigram had been reported, including crossover filling with retrograde backflow, and dermal backflow in the lower extremities.13–15 Reflux of radiotracer through the incompetent lumbar and iliac lymphatics into the other affected extremity or the external genitalia can be shown on 3-hour and 6-hour imaging when the single nonaffected limb is injected.9,16,17 Lymphatic varicosities, large lymphangiectatic lesions, extensive retroperitoneal lymphatic dysplasia, and dilated superficial and deep lymphatic collectors were displayed by non-contrast MRL.14,18
In this research, lymphedema in the lower extremities because of CR tends to occur in childhood initially, begin centrally, and proceed distally. Typical findings could be absent in the early stage of CR associated lymphedema. Delay of chylous vesicles onset after swelling could be observed. Chylous discharge after acupuncture or skin breakdown should be queried during history collection. As reported, genital lymphedema is often observed in patients with lower extremity lymphedema. 19 The patients with genitals involved prior to lower extremities have a higher probability of CR. There was a predominance of males with CR associated lymphedema of the lower extremities. We noticed that some female patients with CR had only chylous vaginal leakage or chylorrhea in the labia.
Visual interpretation of bipedal lymphoscintigraphy is sufficient to provide a reliable diagnosis. Lymph drainage in CR is influenced by orthostasis. The tracer disperses in the distal part of the leg, and the patulous lymphatics in the thigh could not be depicted. 18 Dense retroperitoneal radioactivity with tracer crossover filling and regurgitation into the leg has been reported. 14 Our data were consistent with previous reports. We found characteristic visual patterns 4 could indicate CR. If we observed normal or widened iliac lymphatic channels accompanied by an outline of the thigh or calf, the patients should be scrutinized to rule out CR. Moreover, few patients had genital radioactivity arising from non-chylous inguinoscrotal lymphatic reflux. 20 Genital lymphedema with increased radioactivity also suggests CR. In patients with hyperplastic or malformed retroperitoneal lymphatic vessels, lymph nodes presumably serve as the barriers to backflow. 21
The evidence also suggests a great possibility of CR (not only lymph reflux) as the mechanism for some patients with lymphedema-distichiasis syndrome. Lymphedema-distichiasis syndrome demonstrated hyperplastic lymphatic vessels with prominent dermal backflow in the vicinity of the lower leg and ankle creating ‘‘profiling of the leg.’’22,23 Dermal backflow may be from the shadow of radioactivity in the lymph vessels.18,24 Similar visual patterns majorly appeared in cases with CR. The major limitation of our data is the lack of genetic diagnosis.
In conclusion, some characteristics for screening CR are identified, namely, initial onset in childhood, starting in the upper part of the thigh and extending downwards, affecting genitals prior to lower extremities, and milk discharge after acupuncture or skin breakdown. The patterns with typical “profiling of the leg” and normal or widened iliac lymphatic trunks strongly correlate with CR. Genital lymphedema with increased radioactivity indicates CR.
Footnotes
Authors’ Contributions
Z.L., S.X., W.S.: Conception and design; W.S., S.X., Y.S.: Administrative support; Y.Z., X.L., S.X., Y.S., K.C., J.X., R.A., C.L., C.Z.: Provision of study materials or patients; Z.L., X.L., R.A., C.L., C.Z., Z.Z., P.L.: Collection and assembly of data; Z.L., S.X., W.S.: Data analysis and interpretation; All authors: Article writing; All authors: Final approval of article.
Author Disclosure Statement
The authors declare no conflict of interest and have no competing financial interests.
Funding Information
This study was supported by funds provided to Wenbin Shen from the Capital Medical University Affiliated Beijing Shijitan Hospital Talent Development Program during the 14th Five-Year Plan (No. 2023LJRCSWB).