
Abstract
Introduction:
We report the usefulness of a tapered cutting needle, which has a polyhedral tip similar to that of a square needle and transitions to a round tip in the middle, for super-microsurgery.
Methods:
We have performed more than 500 lymphaticovenular anastomoses (LVAs) using tapered cutting needles. Therefore, we investigated the caliber of the anastomosed lymphatic vessels and veins, characteristics of the lymphatic vessels, the time required to perform the anastomosis, damage to the lymphatic vessels and veins during anastomosis, and patency of 30 recently performed consecutive anastomoses.
Results:
The mean caliber of the anastomosed lymphatic vessels was 0.68 mm (range, 0.4–1.2 mm), and the mean caliber of the veins was 0.87 mm (range, 0.5–1.5 mm). Regarding the progression of fibrosis, 14 cases were classified as no degeneration, 13 cases were classified as mild degeneration, 2 cases were classified as moderate degeneration, and 1 case was classified as severe degeneration. The average time required to perform the anastomosis was 10.53 minutes (range, 8–13 minutes). No cases of lymphatic or venous injury or laceration occurred during the anastomosis procedure. After the anastomosis was created, intraoperative patency was observed in all patients.
Conclusion:
The tapered cutting needle is useful for LVAs because of its excellent thread-ability and protective properties for blood vessels. Furthermore, the tapered cutting needle is useful for short anastomoses, regardless of the diameter or condition of the lymphatic vessels. In the future, the tapered cutting needle is expected to become the needle of choice for LVAs.
Introduction
The lymphaticovenular anastomosis (LVA) is the most versatile surgical treatment for lymphedema. The LVA reduces edema and is associated with various surgical effects, such as the prevention of cellulitis,1,2 reduction of chronic inflammatory lesions that occur in the affected limbs of patients with advanced lymphedema and genital acquired lymphangiectasia. 3 It has been reported that 20%–50% of patients who undergo axillary or pelvic lymph node dissection for breast cancer or gynecological cancer, respectively, develop secondary lymphedema. In addition, the incidence is even higher in patients who have undergone radiotherapy or chemotherapy. Previously, we performed histological examinations after creating the LVA using animal models and investigated the key points of postoperative long-term patency and effective surgical outcomes.4–6 Furthermore, we clarified that intraluminal exposure of subintimal tissue at the anastomotic site is the main cause of anastomotic occlusion. Additionally, we performed the LVA in elderly patients older than 70 years, which has been rarely reported, 7 and described the concept of a preventive LVA before the onset of lymph edema 8 and combined therapy with an LVA for high-stage patients. 9 We have reported the usefulness of the LVA for patients with various backgrounds.10–12 Moreover, a meta-analysis examined the relationship between the number of anastomoses and anastomotic style of the LVA and surgical efficacy. 13
However, the lymphatic vessels and small veins used for the LVA generally have a diameter smaller than 1 mm and require a more delicate surgical technique than that used during normal microsurgery, which is usually performed during free flap transfer. Conical cutting needles have been reported to increase the efficiency of LVA.14,15 In LVA, it is necessary to perform anastomosis with less countertraction than in conventional microsurgery. Therefore, a needle thread with high thread penetrability is useful. In this time, we report the usefulness of a tapered cutting needle (Figs. 1 and 2), which has a polyhedral tip similar to that of a square needle and transitions to a round tip in the middle, for super-microsurgery.
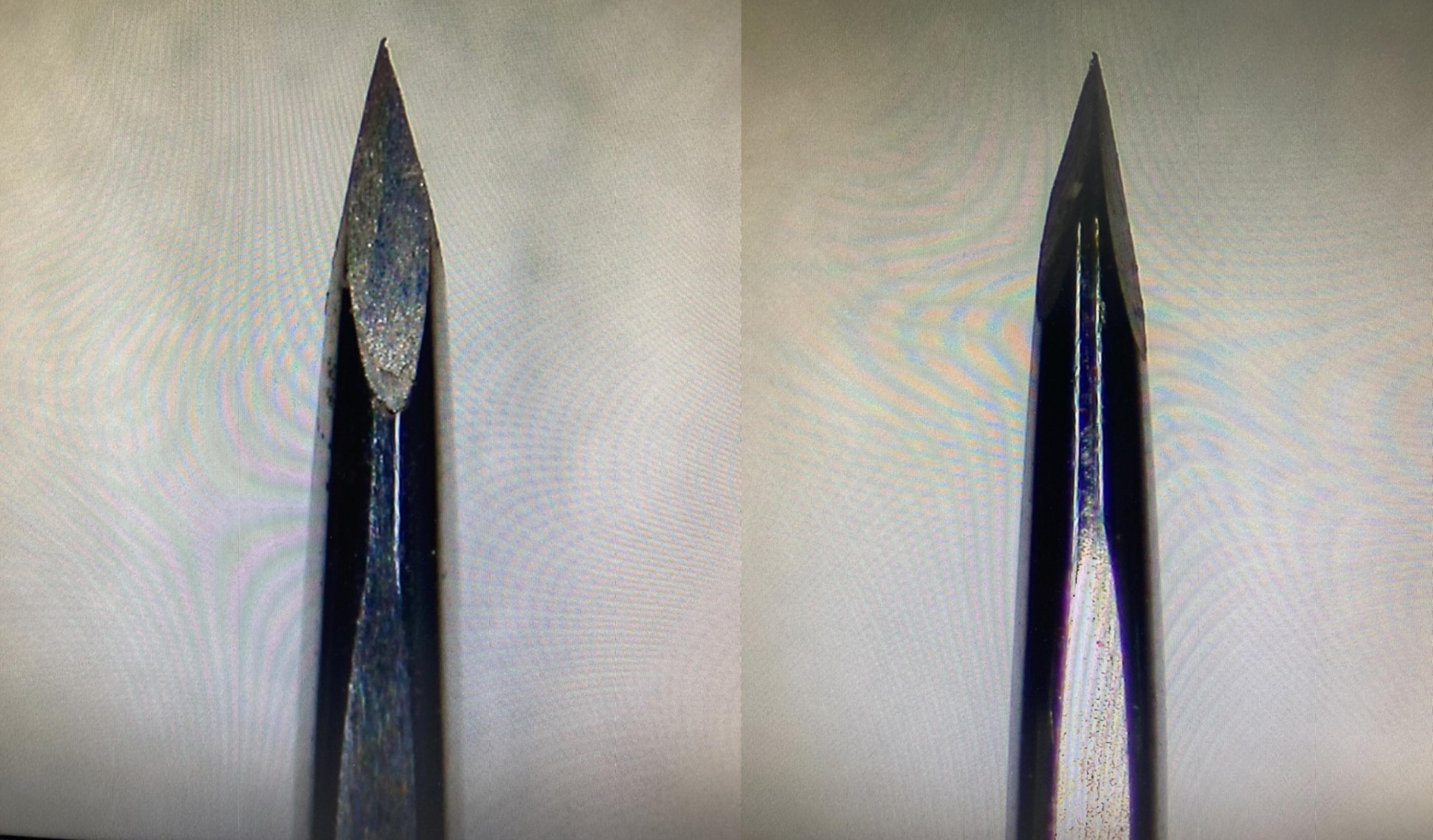
Tapered cutting needle tip. The tip is multifaceted and sharp.

Transition from the tip to the body of the tapered cutting needle. A smooth transition from the sharp to the circular area is observed.
Material and Methods
This study was performed under a protocol approved by the Toyama University Hospital ethics committee. Informed patient consent was deemed unnecessary for this study and was therefore not obtained. We have performed more than 500 LVAs using tapered cutting needles. Therefore, we investigated the caliber of the anastomosed lymphatic vessels and veins, characteristics of the lymphatic vessels, the time required to perform the anastomosis, damage to the lymphatic vessels and veins during anastomosis, and patency of 30 recently performed consecutive anastomoses. Regarding the characteristics of lymphatic vessels, the degree of hardening and progression of fibrosis were classified into four levels: severe degeneration, moderate degeneration, mild degeneration, and no degeneration. To perform comparisons, 30 cases involving LVAs created using a normal round needle were also studied in the same way.
Surgical procedure
Indocyanine green fluorescent angiography (ICG) and ultrasonography were used to identify the location of lymphatic vessels and veins preoperatively. Lymphatic vessels should be selected for early ICG contrast, and veins should have a valve structure and be approximately 1 mm in diameter. 16 Based on preoperative examination, determine the position of the skin incision. Under local anesthesia, a skin incision was made to identify the lymphatic vessels and closest caliber vein for the anastomosis. The central segment of the lymphatic vessel and peripheral segment of the vein were cut while maintaining a length that allowed for the anastomosis without tension. The resected ends of the lymphatic vessels and veins were placed on a background sheet, and the anastomosis was initiated after excess tissue was trimmed from the transected ends. We used 12-0 nylon thread when the diameters of the vein and lymphatic vessel to be anastomosed were 0.5 mm or smaller; however, for other cases, we used 11-0 nylon thread. If the diameter of the lymphatic vessels was too small to insert the forceps in the lymphatic vessels for the anastomosis, then we gently pushed the entire lymphatic vessel with the forceps while poking the lymphatic vessel wall with the tip of the tapered cutting needle. When the needle tip was positioned at the desired location on the lymphatic wall, the needle was pushed into it. The second and subsequent stitches were performed in the same manner by probing the lymphatic wall with the tip of the needle; then, the needle was passed and the anastomosis was created at the appropriate position. After the anastomosis of the anterior wall was completed, the anastomotic vessel was turned over, and the anastomosis of the posterior wall was performed in the same manner (Supplementary Video S1).
Characteristics of tapered cutting needles
The tip of the tapered cutting needle is in the form of a sharp square needle with a gradual circular transition from the center. Therefore, the sharp part of the square needle is used for easy penetration into the wall, and the point of exit of the needle is in the form of a circle, which does not cause blood leakage. The needle’s excellent penetrability eliminates the need to apply excessive force to the wall, preventing wall damage during anastomosis. A t-test was performed to compare the operation time using tapered cutting needles or normal round needles. p < 0.05 was defined as statistically significant.
Results
Of the 30 anastomoses, 24 were for secondary lymphedema and 6 were for primary lymphedema. Eleven anastomoses and 19 anastomoses were created in the upper and lower extremities, respectively. The mean caliber of the anastomosed lymphatic vessels was 0.68 mm (range, 0.4–1.2 mm), and the mean caliber of the veins was 0.87 mm (range, 0.5–1.5 mm). Regarding the progression of fibrosis, 14 cases were classified as no degeneration, 13 cases were classified as mild degeneration, 2 cases were classified as moderate degeneration, and 1 case was classified as severe degeneration. Regarding the progression of hardening, 14 cases were classified as no hardening, 13 cases were classified as mild hardening, 2 cases were classified as moderate hardening, and 1 case was classified as severe hardening. The average time required to perform the anastomosis was 9.93 minutes (range, 8–13 minutes). No cases of lymphatic or venous injury or laceration occurred during the anastomosis procedure. After the anastomosis was created, intraoperative patency was observed in all patients (Table 1).
Details of the Lymphaticovenular Anastomosis Using Tapered Cutting Needles
Regarding the anastomoses created using a normal round needle, 23 were for secondary lymphedema cases and 7 were for primary lymphedema cases. Four and 26 anastomoses were created in the upper and lower extremities, respectively. The mean caliber of the anastomosed lymphatic vessels was 0.56 mm (range, 0.3–0.9 mm), and the mean caliber of the veins was 0.72 mm (range, 0.4–1.5 mm). Regarding the progression of fibrosis, 9 cases were classified as no degeneration, 12 cases were classified as mild degeneration, 8 cases were classified as moderate degeneration, and 1 case was classified as severe degeneration. Regarding the progression of hardening, 13 cases were classified as no hardening, 13 cases were classified as mild hardening, 1 case was classified as moderate hardening, and 3 cases were classified as severe hardening. The average time required to create the anastomosis was 13.47 minutes (range, 10–15 minutes). In three cases, lymphatic vessel laceration was observed during the creation of the anastomosis, and another anastomosis was created (Table 2). p < 0.05 in the required time for anastomosis was predominantly shorter for the taper cutting needle.
Details of the Lymphaticovenular Anastomosis Using Normal Round Needles
Discussion
Microsurgery, which usually involves the anastomosis of blood vessels with a diameter of 2–3 mm, and super-microsurgery,17–19 which involves the anastomosis of blood vessels, nerves, and lymphatic vessels smaller than 1 mm, differ greatly in the thickness of the thread used, instruments used, such as needle holders, surgical shears, and vascular clips, and surgical techniques used for the anastomosis. With conventional microsurgery, the patency rate after anastomosis is generally very high (≥97%), and cases of anastomotic failure are rare.20,21 Additionally, the success or failure of flap transfer is evident. Although the success or failure of anastomoses can be clarified during super-microsurgeries such as amputation and finger reattachment, patency immediately after performing the LVA can be confirmed by clinical findings and ICG examination findings; however, in many cases, the postoperative condition cannot be scrutinized.22–27 This makes it difficult to review the relationship between the anastomosis technique and surgical results and is considered an obstacle to improving the technique.
In particular, with super-microsurgical anastomoses, it is difficult to apply countertraction when inserting the needle in the wall using forceps inside the lymphatic vessel, thus making it difficult to insert the needle at the appropriate site. Therefore, we previously reported surgical innovations that allow quick and accurate LVAs.28,29 We also published an educational video regarding super-microsurgery with an LVA. 30
In this study, the diameter and characteristics of the anastomotic target vessels were similar between the regular circular needle and the tapered cutting needle. However, the time required for anastomosis was more than 3 minutes shorter with the tapered cutting needle, and there were no cases of damage during anastomosis. This suggests that the tapered cutting needle is a more suitable suture needle for LVA.
Comparison of round and tapered cutting needles
A circular needle with a pointed tip and a thick, circular shape is usually used for anastomosis of blood vessels and lymphatic vessels. This shape prevents damage to the vascular vessels and leakage of liquid components such as blood and lymphatic fluid from the needle entry point. However, in the present study, lymphatic vessel laceration was observed in three cases during anastomosis creation, and another anastomosis was required. Lymphatic vessels have a small diameter and a very thin wall; therefore, applying excessive force when threading the wall can result in damage to the wall.
In contrast, the tapered cutting needle is square at the tip and rounded at the midpoint. Therefore, the tapered cutting needle is superior to the normal round needle because of its ability to penetrate the vascular wall at the tip. Furthermore, because the body of the tapered cutting needle is shaped like that of a round needle, the entry point after penetration is round; therefore, no leakage of blood or lymphatic fluid occurs in this area. Therefore, the tapered cutting needle is useful for super-microsurgical anastomoses and suturing blood vessels and lymphatic vessels with very small diameters for which countertraction cannot be applied when the needle is inserted in the wall.
Adaptation of tapered cutting needle
Tapered cutting needles are also used during conventional microsurgery because of their ease of use when creating LVAs. A technical problem during microsurgery, especially for inexperienced surgeons, is the weak countertraction force when using forceps in the hand opposite the needle holder. In this regard, the use of a tapered cutting needle with excellent penetration force is thought to facilitate good anastomoses, even when performed by beginners. The tapered cutting needle is also effective for the arterial anastomosis, for which penetration is difficult because of arterial stiffness by arteriosclerosis. Additionally, when performing more delicate techniques and attempting to increase the penetration force, holding the needle for a shorter duration can be effective. We typically use a 4-mm-diameter needle when creating the LVA and hold the needle approximately two thirds distal from the center of the needle. However, when the anastomosis involves thin vascular vessels or caliber differences and requires fine adjustment, we grasp approximately one third of the proximal portion. The grasping position is adjusted one needle at a time so that the anastomosis can be performed smoothly.
Problem of tapered cutting needles
One concern regarding the use of tapered cutting needles is that the angular needle portion penetrates the vascular wall, thus damaging the wall and tearing or breaking the lymphatic vessel wall during anastomosis. However, during this study, there were no cases of such lacerations of the vascular wall. Furthermore, in our experience, the vascular wall is rarely damaged when performing the anastomosis. On the contrary, it is thought that the anastomosis can be created in a gentler manner without applying excessive force to the wall of the vascular canal.
This study suggests that the taper cutting needle is highly useful in lymphatic surgery. If the usefulness of tapered cutting needles becomes widely known and they are used by many lymphatic surgeons, it will increase the efficiency and effectiveness of surgery and contribute to improving the quality of life of patients with lymphedema.
Conclusion
The tapered cutting needle is useful for LVAs because of its excellent thread-ability protective properties for blood vessels. Furthermore, the tapered cutting needle is useful for short anastomoses, regardless of the diameter or condition of the lymphatic vessels. In the future, the tapered cutting needle could reduce the technical difficulties associated with the LVA and dramatically change the surgical style; therefore, it is expected to become the needle of choice for LVAs.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.