
Abstract
Background:
Lymphedema is one of the disturbing complications after breast cancer treatment that may affect the quality of life (QoL) of breast cancer survivors (BCSs).
Methods:
In this double-blind randomized clinical trial, 63 patients with breast cancer-related lymphedema (BCRL) were included in the study. Group A received standard complete decongestive therapy (CDT), group B received CDT with olive oil, and group C received CDT with chamomile and olive oil. Lymphedema volume and range of motion (RoM) were measured at the beginning of the study and at sessions 7, 14, and 21. Patients’ QoL was measured using the Short Form 36 questionnaire at baseline, at the end of the trial, and 1 month after the trial. For statistical analysis, SPSS software with a significance level of p < 0.05 was used.
Results:
The mean age of patients was 55.4 ± 10.1 years. Although the volume of lymphedema was reduced and RoM was increased in all groups, there was no significant difference between the three groups. However, the change in volume and RoM was more evident in group C. Moreover, the effect of interventions on health-related QoL dimensions in all groups was not statistically significant. However, in some dimensions, the score did not decrease in group B during follow-up.
Conclusions:
Chamomile and olive oils are tolerable for BCSs with BCRL; however, adding this intervention to CDT seems to have no superiority to CDT alone.
Introduction
Breast cancer-related lymphedema (BCRL) is one of the important complications after surgery and radiotherapy for breast cancer treatment. The incidence of BCRL depends on differences in BCRL assessment and follow-up duration, and it is suggested that at least one of five survivor women will develop BCRL in the first 2 years. 1 However, the incidence rises in studies with longer follow-up periods.2,3 BCRL is due to chronic lymphatic circulation impairment that leads to edema, accumulation of adipose tissue, and fibrosis. It causes disability of limb, pain, heaviness, and infection; taken together, these decrease the patient’s quality of life (QoL). 4
While there is no cure for BCRL, the current standard management is complete decongestive therapy (CDT). This includes lymphatic drainage, bandaging, exercise, and skincare that mainly decrease volume-related symptoms but need the patient’s compliance for a long time. 5 Although research for new therapies is ongoing and pharmacotherapeutics, new surgery techniques, and low laser therapy have been reported to be useful, 6 patients also may be interested in complementary therapies since these are not invasive or expensive. 7 Some clinical studies have reported the beneficial effects of herbal medicine for BCRL. Coumarin, a well-known benzopyrone, and other phytochemicals have been studied for BCRL treatment.8,9
Chamomile (Matricaria chamomilla L.) is an herb of the Asteraceae family, and its flowers contain oils such as bisabolol and chamazulene and flavonoids such as apigenin and luteolin. 10 Chamomile has been reported to have anti-inflammatory effects by inducing the release of interleukin-10 (IL-10) from macrophages, which acts as an anti-inflammatory cytokine. 11 It also can reduce the production of IL-6 and tumor necrosis factor alpha (TNF-α), two major inflammatory mediators in lymphedema pathogenesis. 12 Moreover, apigenin induces apoptosis and inhibits the growth of different human cancer cell lines.13,14 Chamomile has antioxidant effects on human skin 15 and can improve wound healing as well as bacterial infection, 16 and its mouthwash has been shown to improve chemotherapy-induced mucositis.17,18 Chamomile was reported to be safe and effective in reducing the frequency of chemotherapy-induced nausea and vomiting among patients with breast cancer. 19
Based on recent studies on the pathophysiology of BCRL, inflammation is the key mechanism of lymphedema progression. 20 According to the anti-inflammatory characteristics of chamomile and its safety in women with breast cancer, we hypothesized that chamomile may improve BCRL.
Materials and Methods
Trial design
This was a randomized controlled trial (RCT) conducted in a lymphedema clinic affiliated with the Iranian Breast Cancer Centre in Tehran, Iran. The ethics committee of Shahid Beheshti University of Medical Sciences approved the study (IR.SBMU.RETECH.REC.1397.1195). Also, the protocol was registered and approved by the Iranian Randomized Clinical Trials (IRCT20190312043024N1). The study followed the consolidated standards of reporting trials (CONSORT) guideline for reporting clinical trials, and there were no changes in the protocol during the study. 21
Participants
Breast cancer survivors (BCSs) aged 35–75 years who had developed unilateral upper limb lymphedema following breast cancer were screened for eligibility criteria during 2022–2023. Inclusion criteria were confirmed treatment of breast cancer, edema of an upper limb with a difference of more than 200 mL compared with the other limb, at least 1-month interval to the last session of breast cancer therapy, and interest to participate in the study. All participants were asked to sign informed consent.
Patients were excluded if they had any of the following criteria: chronic or acute infection, cardiovascular or renal diseases, lymphedema due to other reasons than breast cancer, smoking, and alcohol use, deep vein thrombosis, and cancer metastasis or recurrence during the study and any adverse effects during the trial.
Interventions
The intervention was performed in three groups. The first group received the standard CDT treatment (including manual maneuvers for lymphatic drainage, special bandages and exercises, and skincare). 5 The second group received CDT and olive oil. Finally, the third group received CDT and chamomile oil with olive oil. Chamomile oil and olive oil were used topically as a part of MLD. The intervention was performed by a trained therapist who had experience in performing lymphatic therapy for patients with cancer. The first phase of CDT was conducted 5 days per week for 4 weeks and a total of 21 sessions. Each session was 40 minutes of manual lymphatic drainage (MLD) based on the Vodder methods. 22 Both chamomile and olive oils were produced at the Traditional Pharmacy Department at Shahid Beheshti University of Medical Sciences.
Outcomes
Outcomes were evaluated by a lymphologist at the beginning (before intervention); 7th, 14th, and 21st sessions of treatment; and 1 month after the intervention.
The primary outcome was the reduction in the volume of edema at the end of the therapy compared with the baseline, whereas the secondary outcome was an improvement in the range of motion (RoM) of the limb and QoL. The amount of edema was measured by the difference in volume and size of the affected arm compared with the healthy arm using water displacement and tape measure. Also, the RoM was measured with a goniometer.
The Short Form 36 questionnaire was used to assess the QoL. The eight dimensions of the questionnaire include physical function, social function, physical pain, vitality and energy, mental function, general health, limitation of role-playing for physical reasons, and limitation of role-playing for emotional reasons. 23 Patients were asked to fill out the questionnaire at three time points: at baseline, at the end of the trial, and 1 month after the trial.
Sample size
For estimation of sample size, variables of pain, heaviness, and QoL in the pilot study, which included five patients, were used. The sample volume with power equal to 80%, at the error level of 5%, and the drop coefficient of 40% was considered.
According to the dependent variables in this study, determining the sample size was equal to the following: (1) In the pilot study, the percentage of patients who presented with pain was estimated to be 60%. A minimum of 17 was required to account for this variable, based on the 40% fallout. (2) At least 15 samples in each group were required for the assessment of the RoM with a 40% drop. (3) At least 15 patients in each group were required to study the volume reduction, taking into account a 40% loss.
According to the results obtained for the studied variables, the minimum number of samples in each group was considered equal to 17 people.
Randomization
The randomization was done using Random Rx version 2 software. Since there were three groups of treatment, every three sets of randomized numbers were allocated to each group. For example, the first three randomized numbers of patients were allocated to the first group and so on.
Blinding
In this RCT, patients and the lymph therapist were not aware of the treatment group. The statistician who was responsible for randomization and analysis was informed about the name of the treatment in each group. For blinding patients, regular lotion for CDT was used as a placebo that had the same bottle and appearance as the chamomile and olive oils. For blinding the therapist, when a patient was included in the RCT, a phone call was made with the statistician to deliver the bottle. The statistician first wrote the actual name of the bottle and then covered it with a piece of paper to blind the therapist to the actual treatment. Allocation of bottles in this RCT was concealed.
Statistical methods
The SPSS (IBM, version 23) was used for statistical analysis with a significance of p < 0.05. Descriptive statistics were reported using mean, standard deviation, frequency, and percentage in this study. Post hoc tests used in the analysis of variance (ANOVA) were significant to examine the binary relationship between the groups. Also, nonparametric tests such as Mann–Whitney and Kruskal–Wallis were used whenever needed.
Results
Demographic characteristics
A total of 63 patients were enrolled in the study, of which 20 patients in group A, 21 patients in group B, and 22 patients in group C were randomly assigned. During the study, two patients in group B showed cutaneous sensitivity and were excluded from the study according to the defined exclusion criteria. Also, two patients were excluded from the study for personal reasons and did not want to continue. These patients were not included in the analysis. The CONSORT diagram is presented in Figure 1. The mean age of patients participating in the study was 55.38 ± 10.1 years. Also, 82.5% of cases had stages 2 and 3 of lymphedema, while in 17.5% of patients, stage 1 was reported. Forty-two (65.6%) patients had received chemotherapy. There was no statistical difference among groups in volume, RoM, QoL, or any of the mentioned characteristics at baseline.
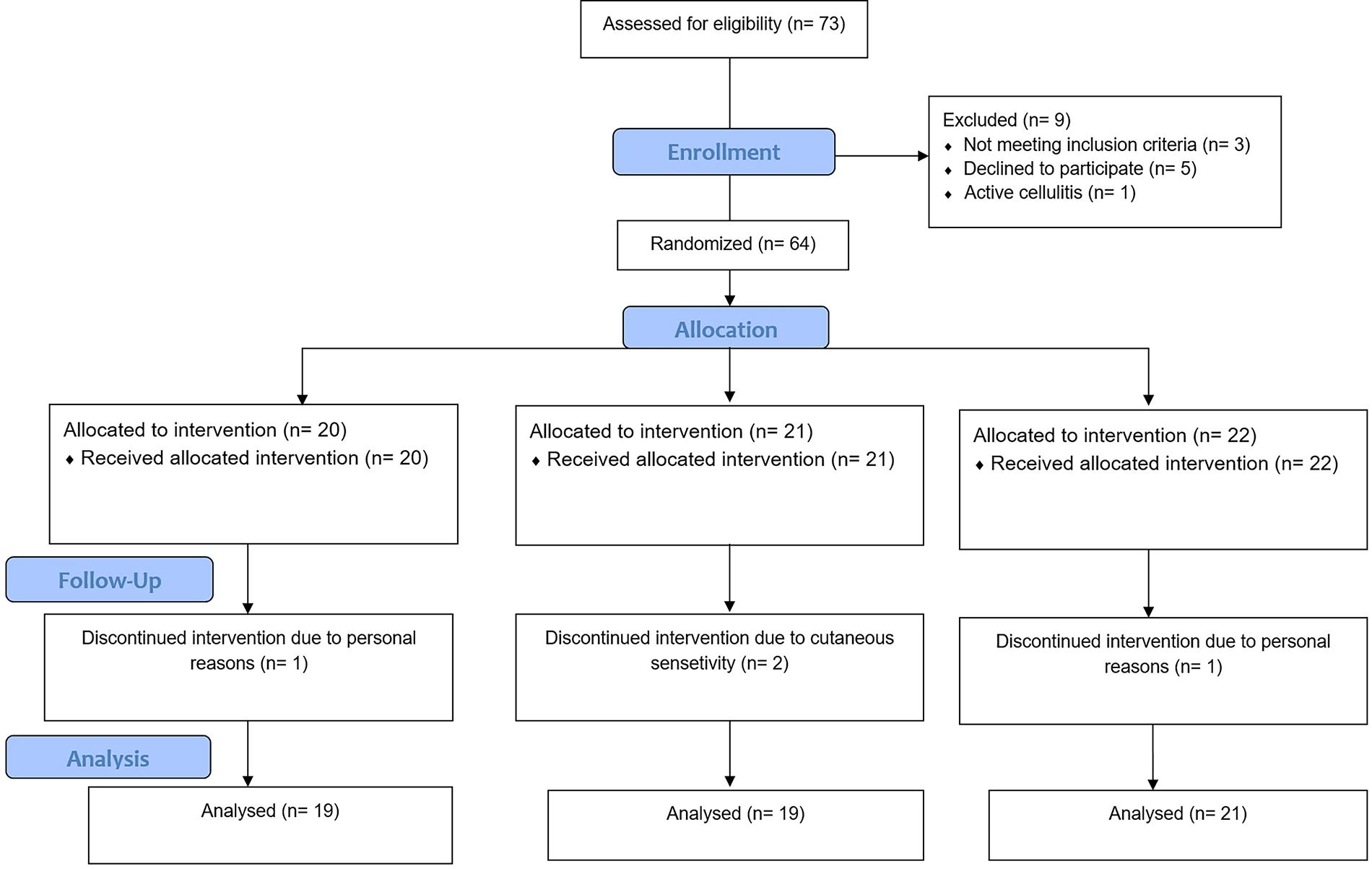
The CONSORT diagram.
Effect on volume
The average volume of edema decreased with an increase in the number of treatment sessions, as shown in Figure 2. The average volume of edema in group A at baseline was 1026.11 mL, which decreased to 353.6 mL at the end of the 21st session. In group B, the mean volume decreased from 1002.7 mL to 310.3 mL at the end of treatment, and in group C, the mean volume of edema decreased from 1237.2 mL at baseline to 445.2 mL at the end of the 21st session.
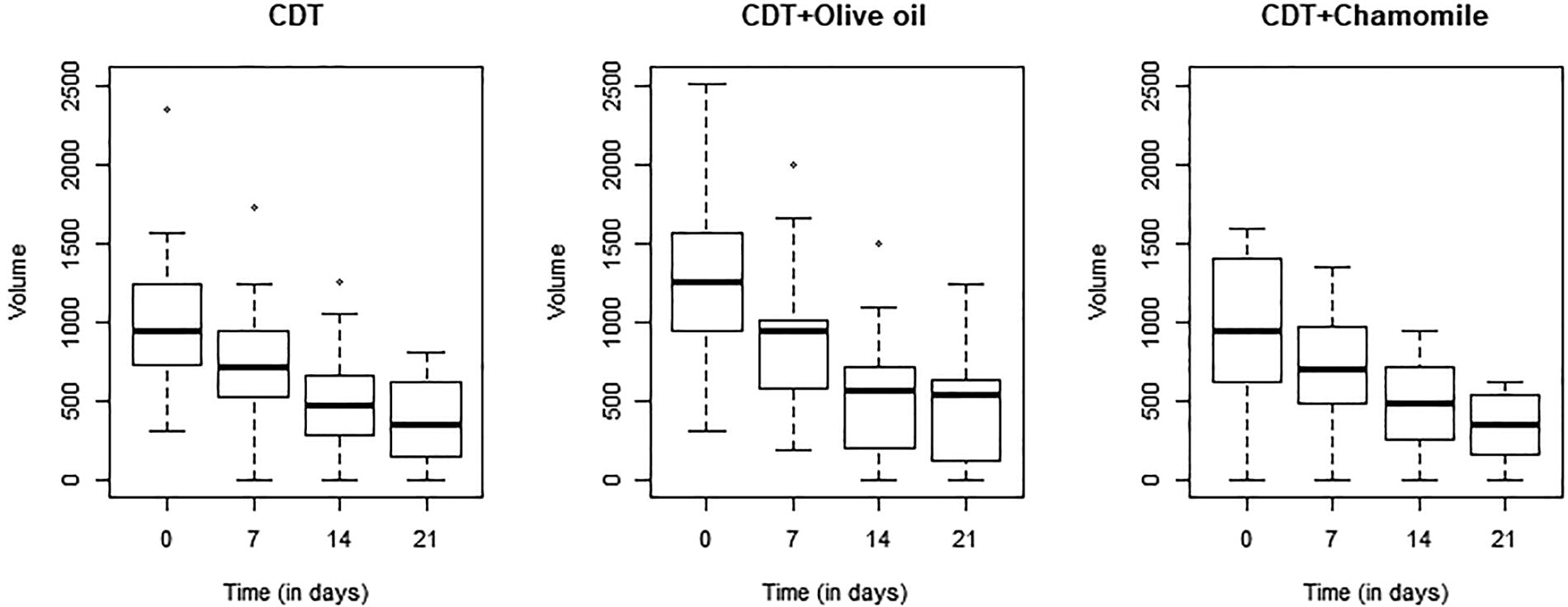
The mean volume of lymphedema at four time points in three groups.
The results of the ANOVA showed that a significant difference was observed in the mean volume of lymphedema at four time points in each group (p < 0.001). Although the volume of lymphedema was significantly reduced in all study groups, according to the results of the analysis, there was no significant difference between the three groups (p = 0.68).
Effect on the RoM
The average shoulder RoM in groups A and C increased with an increase in the number of treatment sessions. But in group B after the 7th session, RoM decreased, as provided in Table 1. In group C, an increase in the mean RoM from 161.36 to 173.63 was observed in the 21st session, whereas the average shoulder RoM in group B increased from 165.9 before treatment to 173.86 at the end of the 21st session. The difference in the mean increase in RoM after the 21st session compared with the baseline in group C was 12.27, which is higher than group A (7.67) and group B (7.96), as shown in Figure 3. The difference in RoM in each group at different sessions was significant (p = 0.009); however, the difference between groups failed to show statistical significance (p = 0.64).
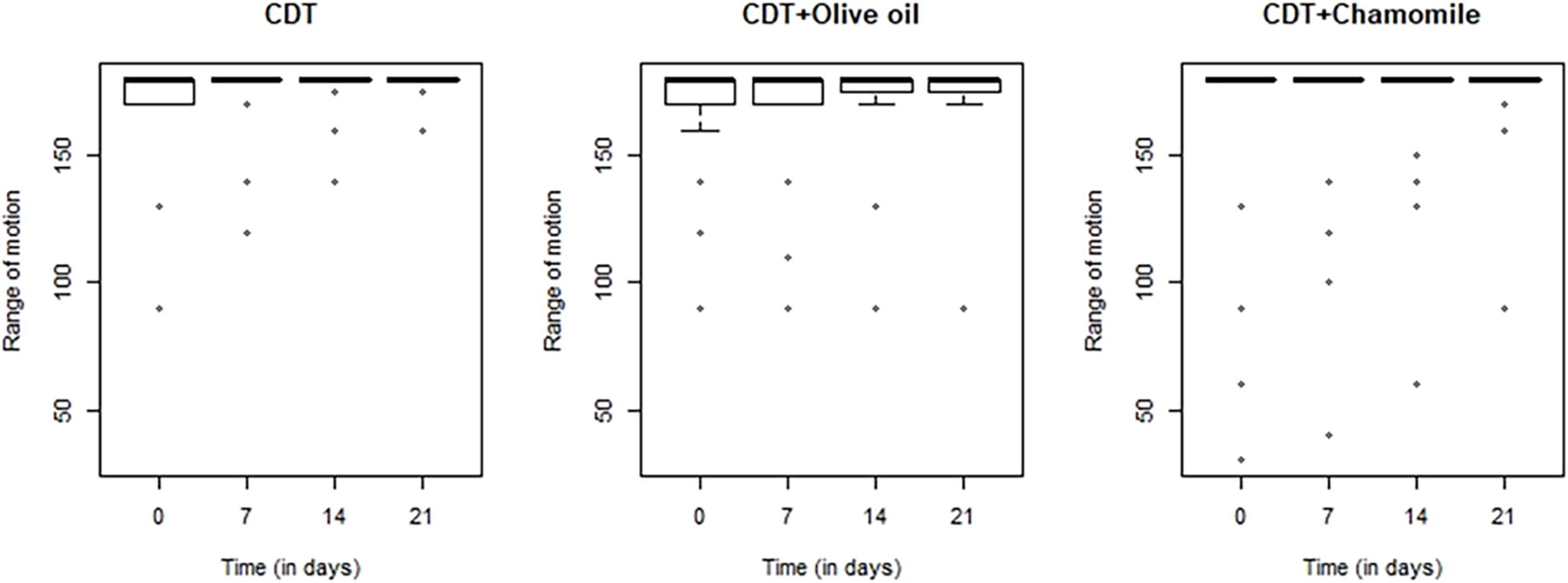
The mean range of motion at four time points in three groups.
Changes in Volume and Range of Motion During the Trial
CDT, complete decongestive therapy.
Effect on QoL
All groups had improvement in physical function; however, it declined after the first month. The total change in group B was more compared with other groups (p = 0.08). Only patients in group C had progressed in limitation of role-playing for physical reasons, although they had lower scores to begin with. The change in general health also declined after the first month, but a higher total difference was observed in group C. Regarding social function, group A had the highest increase in score; however, only group B showed higher scores also 1 month after the trial. There was an improvement in the limitation of role-playing for emotional reasons, which were more evident in group B and were declined in all three groups. Scores related to mental health, physical pain, vitality, and energy were increased and then declined in patients except those in group B. None of the changes in scores for QoL dimensions were significantly compared among groups. The change in each dimension is presented in Table 2.
Changes in Each Domain of Quality of Life During the Trial
CDT, complete decongestive therapy.
Discussion
BCRL is the malfunction of lymphatic circulation as a consequence of radiotherapy or surgical interventions for breast cancer. Lymphedema imposes a substantial impact on BCSs with heaviness, pain, limitation in RoM, and generally by decreasing their QoL. 4 In this study, treatment with CDT plus olive oil or CDT plus olive and chamomile oils failed to show any significant superiority to treatment with CDT alone among patients with BCRL. One reason could be the difference of groups at baseline. Despite that the difference in volume was not significant between groups, still, patients participating in group C had a higher mean lymphedema volume than the other two groups at baseline, and at the end of treatment, it seems that the reduction of edema in this group has been more evident. A similar reason could be mentioned for RoM, as the baseline value was the lowest in group C, and yet the highest increase was observed in this group. The number of patients in each arm was limited, and other trials with higher participants may show significant improvement by treatment with chamomile oil. Also, another reason should be mentioned in the limited time of follow-up. The time point of 1 month after the trial was only considered for QoL assessment.
Different phytochemicals, especially coumarin, have been investigated for lymphedema management. 9 Olive oil has been studied in one trial, 24 but to the best of our knowledge, chamomile has never been investigated for BCRL management. McCord et al. studied the effects of Olivamine-based skincare for 6 months on pruritus intensity. In this study, nine patients with leg or abdominal pannus lymphedema were included, and preliminary results showed improvement in pruritus intensity. 24 In our study, CDT plus olive oil had no significant superiority, but patients in group B generally did not have a decrease in QoL scores in most domains 1 month after the trial. Also, some other studies have investigated the effects of olive or chamomile oil among BCSs. For instance, radiodermatitis is another complication of radiotherapy, which also shares some aspects of pathophysiological mechanisms with BCRL. 25 Both chamomile and olive oils have been reported to be potentially useful in the prevention of radiodermatitis.26,27 The preventive effect of chamomile or olive oils on BCRL remains to be studied in the future.
Chamomile (M. chamomilla) is well known for its anti-inflammatory, antioxidant, and analgesic properties. The anti-inflammatory effects of chamomile are primarily due to its bioactive compounds, including chamazulene, apigenin, and bisabolol.12–14 These components have been shown to inhibit the production of proinflammatory cytokines, including TNF-α and IL-6, which are often elevated in patients with cancer and chronic inflammatory conditions such as lymphedema. 4 By reducing these inflammatory mediators, chamomile may alleviate the swelling and discomfort associated with lymphedema, thereby improving physical functioning and RoM. Volume reduction leads to improvement in accompanying symptoms such as pain, sleep quality, and other aspects of QoL.28,29 While no significant difference was observed in volume reduction between groups, the improvement in patients’ QoL can be attributed to the reduction in physical symptoms and volume reduction. This multidimensional improvement leads to enhancements in both physical and psychological aspects of QoL, which are particularly significant in BCSs managing the challenges of lymphedema. The synergistic effects of chamomile’s anti-inflammatory and psychological benefits likely explain the observed improvements in QoL following the intervention in this trial.
In one previously published study, we reported the possibility of reducing the number of CDT sessions by reaching the desired endpoints of volume and pain reduction before the completion of all sessions. 28 Using complementary therapies such as herbal medicine is an interesting topic of research to decrease the number of therapy sessions. This may lead to lower costs and better adherence to desirable outcomes. Lymphedema has not been well addressed in biomedical research, and therefore, there are still no pharmacotherapeutics developed.30,31 Although recent interest in surgical intervention has led to better outcomes, CDT remains the standard treatment for BCRL. CDT requires trained practitioners and also patients’ time and expenses. The completion of whole sessions may not be practical for some individuals. Also, certain circumstances may affect their accessibility to CDT, as was the case during the COVID-19 pandemic. 32 Therefore, research on improving CDT outcomes, decreasing the number of sessions, or even highlighting self-care would be of great value. Although such an objective was not considered the main outcome of this RCT, current results show preliminary findings of the safety and tolerability of chamomile and olive oils plus CDT among patients with BCRL. Additionally, results showed a higher decrease in volume and improvement in RoM and QoL in groups B and C compared with group A, which received CDT alone. There was no significant difference between groups, but the higher change due to chamomile and olive oils could be beneficial for reducing the number of CDT sessions.
One of the limitations of this study was the limited sample size. Also, the lack of long-term follow-up was another limitation. Moreover, measuring changes in inflammatory biomarkers related to lymphedema and the frequency of cellulitis among participants could be a precise and accurate method for investigating the efficacy of the intervention, which was not performed in this study. Nevertheless, this study investigated the effect of chamomile and olive oils on BCRL for the first time and therefore could be evidence for future studies.
Conclusions
Results of this study showed that CDT plus chamomile and olive oils had no significant superiority compared with CDT alone among patients with BCRL. However, adding chamomile and olive oils to CDT resulted in more evident changes. This may have clinical implications, and further trials are needed to investigate the potential of herbal medicine for reducing the number of CDT sessions.
Footnotes
Authors’ Contributions
Z.S.: Conceptualization, methodology, and software. H.Y. and M.S.: Data collection and writing—original draft preparation. P.M.-H.: Visualization and investigation. G.H.: Supervision. S.F.: Software and validation. A.M.: Writing—reviewing and editing.
Ethical Statement
This trial was performed based on the Declaration of Helsinki of 1975 and also the ethics committee of Shahid Beheshti University of Medical Sciences approved the study (IR.SBMU.RETECH.REC.1397.1195). All participants filled out an informed consent form before the study. Also, the protocol was registered and approved by the Iranian Randomized Clinical Trials (IRCT20190312043024N1).
Author Disclosure Statement
All authors declare that there were no interests to be stated.
Funding Information
This study was funded by Shahid Beheshti University of Medical Sciences (IR.SBMU.RETECH.REC.1397.1195).