
Abstract
Background:
To evaluate the stiffness of the skin and subcutaneous tissues of the arm and forearm of patients with breast cancer-related lymphedema using shear-wave elastography (SWE) and to investigate the relationship between the patients’ symptoms.
Methods and Results:
Both lymphedematous and unaffected upper extremities of 72 patients (72 lymphedematous and 72 unaffected extremities) and 72 upper extremities of 36 controls (72 healthy extremities) were included in the study. The stiffness of the skin and subcutaneous tissues of all extremities was evaluated with SWE. The patients’ pain, tension, weight, and stiffness symptoms associated with lymphedema were questioned using a numerical scale. The patients’ functionality and participation in daily life activities were evaluated. The skin stiffness of the affected extremity was higher and the subcutaneous tissue stiffness was lower in patients than in controls (p < 0.05). The skin stiffness of the affected forearm was higher and the subcutaneous tissue stiffness of the affected arm and forearm was lower than their healthy extremities (p < 0.05). Quick Disabilities of Arm, Shoulder, and Hand and Life Impact Scale; were negatively correlated with arm and forearm subcutaneous tissue stiffness and positively correlated with forearm skin stiffness. The decrease in subcutaneous tissue stiffness of the arm was associated with heaviness sensation, the increase in skin stiffness of the forearm was associated with tightness, and the decrease in subcutaneous tissue stiffness of the forearm was associated with tightness, heaviness, and stiffness sensations.
Conclusion:
The results of this study suggest that SWE measurements can be useful for diagnosis and follow-up of patients.
Introduction
Lymphedema is diagnosed by symptoms, clinical examination, circumference and volumetric measurements, and various imaging methods that provide more objective evaluation. Lymphosyntigraphy, the most used diagnostic test for lymphedema, is invasive, expensive, and a long-term examination involving radiation.1,2 It is not readily available for clinical utility in a lymphedema clinic for use by the practicing physiatrist. It is usually taken in the radiology department of hospitals and evaluated by radiologists. Ultrasonography (USG), besides, stands out with its low cost, no radiation, being noninvasive, and providing information about tissue content. However, its role in diagnosing and grading lymphedema needs to be clarified, as it is not objective, is a practitioner-dependent examination, and requires clear diagnostic criteria for lymphedema.3–5
On the contrary, many symptoms associated with lymphedema may contribute to detecting and grading lymphedema. Among these symptoms, limb stiffness is one of the main symptoms of patient and limb function. Therefore, understanding the mechanical properties of soft tissue in the lymphedema extremity is critical in clinical diagnosis and treatment planning. 6 Objective and quantitative evaluation of soft tissue stiffness provides information about the prognosis of the disease. Also, it allows the assessment of the effect of treatment, early detection of treatment failure, and the need for surgical intervention.
Shear wave elastography (SWE) is an imaging method that evaluates tissue stiffness based on USG. Compared to other elastographies, SWE is not pressure- or user-dependent, so its results are more standardized. Considering the fibrotic tissue changes that develop in lymphedema, SWE may be helpful in the early diagnosis and follow-up of the disease. 2 The latent stage is the early stage of the clinical stage, the preclinical stage in which lymph circulation is impaired, clinical findings have not yet developed, and cannot be detected by lymphoscintigraphy. The clinical stage is the stage in which patients can be detected by lymphoscintigraphy or clinical findings and consists of three stages in which symptoms and clinical findings increase as the stage increases. 7 Already, there is no gold standard in the diagnosis and early detection of lymphedema. Therefore, the use of SWE in diagnosing and staging lymphedema may contribute to facilitating the treatment, follow-up, and rehabilitation process of lymphedema, timely intervention, and eliminating confusion between imaging methods.
Generally, studies evaluate the volume circumference difference between the two extremities as the primary outcome measure for assessing treatment efficacy. However, symptoms that reduce patients’ functionality and quality of life (QOL) should be prioritized in terms of treatment effectiveness. As the lymphedema stage progresses, the fibrosis in the tissue increases, and the tissue stiffness increases the patients’ symptoms. Therefore, if this increased stiffness is shown objectively and the relationship with the symptoms is revealed, SWE can be used as an essential outcome measure in the follow-up and evaluation of patients with lymphedema treatment response.
The primary aim of this study was to measure skin and subcutaneous tissue stiffness by SWE in the lymphoedematous extremities of patients and to compare them with the measurements of healthy extremities of patients and control group, and thus to determine the role of SWE in the diagnosis and staging of patients and to detect patients in the preclinical (latent) stage, which is an earlier stage that is not yet clinically detectable. The secondary aim was to examine the relationship between SWE measurements and lymphedema-related symptoms of the patients.
Materials and Methods
Patients who were previously diagnosed with lymphedema by lymphoscintigraphy, which is a traditional diagnostic method, were primarily included in the study. Then patients aged between 18 and 75 years, and having stage 0–1–2 lymphedema according to the International Society of Lymphology staging were included. In the control group, individuals aged between 18 and 75 years and without a history of breast cancer or lymphedema were included.
Participants with a history of surgery and trauma in the assessment area, signs of active infection, congenital or acquired malformations in the assessment area, primary lymphedema, and any medical condition that could cause edema, such as advanced heart or kidney failure, were excluded from the study.
The limb on the surgical side was referred to as the “lymphedematous extremity” and the limb on the nonsurgical side was referred to as the “unaffected extremity.”
In the study, while both the healthy (unaffected) and lymphedematous extremities of the patient group were included, the control group had each of its extremities included separately as control extremities.
The sociodemographic and clinical characteristics of patients were recorded. The patients’ lymphedema-related extremity pain and feelings of tightness, heaviness, and stiffness were evaluated separately by a numerical scale. The patients’ participation in lymphedema-related daily living activities was assessed with the Quick Disabilities of Arm, Shoulder, and Hand (Quick-DASH) and the Lymphedema Life Impact Scale questionnaires (LLIS).
The Turkish validity and reliability of the Quick-DASH questionnaire were performed by Düger et al. 8 Each section is evaluated and then a score between 0 and 100 is obtained. A high score indicates a high level of disability. The Turkish validity and reliability of the LLIS questionnaire were performed by Değirmenci et al. (2019). 9 It consists of 18 items. The score range for each item is between 1 and 5. High scores indicate a high level of limitation in the assessed area. Both questionnaires do not have a cutoff value, with higher scores indicating a more severe disability.
The circumference measurement was performed starting from wrists to arm level with 4 cm intervals. Those with a circumference measurement difference of less than 2 cm and/or a 10% volume difference were considered preclinical (latent, early clinical), and those above these values were regarded as clinical lymphedema. The volume calculation for both upper extremities was calculated with the truncated cone formula.
SWE parameters were evaluated with the 6–15 mHz linear probe of the GE Logiq E9 device. Gain, frequency, and depth settings were fixed in all patients. The skin and subcutaneous tissue elasticity of the patients were measured from the medial side of both arm and forearm (10 cm proximal and distal to the medial epicondyle) in kilopascals by SWE with the USG probe parallel to the arm axis and in the midline. A gel pad was used to prevent pressure on the skin and to make the stiffness measurement more accessible and more accurate (shown in Fig. 1).

The placement of the gel pad and probe according to the axis of the arm.
The images were taken from the area containing the skin and subcutaneous region; four regions of interest (ROIs) were marked separately from the skin and subcutaneous tissue (shown in Fig. 2).

For SWE measurements, evaluation of homogeneity and stiffness according to colors and then determination of four ROI areas. ROI, regions of interest; SWE, shear-wave elastography.
Evaluations were performed first on the right forearm, then on the right arm; it was done in a particular order as the left forearm and the left arm. The probe positioning and measurement sequence were planned by taking into account the studies in the literature on this subject and measurements were performed in a similar manner to the studies.2,10 SWE assessments were performed by the same investigator for all participants. For intraobserver consistency, measurements of 10 patients were repeated by the same investigator 2 weeks after the measurements. For interobserver consistency, 20 patients were reevaluated by the second investigator.
This study has been approved by the Marmara University Faculty of Medicine Ethics Committee with protocol number 09.2022.145, in accordance with the Helsinki Declaration.
Statistical analysis
SPSS version 23 (IBM Corp., Armonk, NY) program was used for statistical analysis to evaluate the data. The conformity of the data to the normal distribution was assessed with the Shapiro–Wilk normality test. In comparison between groups, the chi-square test for categorical data was used to compare independent variables, the t-test was used in separate groups if the data fit a normal distribution, and the Mann–Whitney U test was used if they did not. In the intragroup comparison, normally distributed data were evaluated with the t-test independent groups, and not normally distributed data were assessed with the Wilcoxon test. In multiple comparisons, one-way Analysis of Variance was used for normally distributed data, and the Kruskal–Wallis test was used for data not normally distributed. If statistical significance was found in these comparisons, Bonferroni correction was used for pairwise comparisons, a t-test was used for data with normal distribution in independent groups, and the Mann–Whitney U test was used for data not normally distributed. Intraobserver and interobserver correlation coefficients were calculated for reliability.
Statistical significance was accepted as p ≤ 0.05 for all analyses.
Results
A total of 85 patients with upper extremity lymphedema were evaluated for the study. Thirteen patients who did not meet the study criteria were excluded. A total of 72 patients (lymphedematous extremities (n = 72) and healthy extremities (n = 72)) and 40 controls (72 control extremities) were included in the study. In the study, the lymphedematous and healthy extremities of the patients were compared (n = 72). In addition, the upper extremities of the patients (n = 72) and 72 upper extremities of the healthy controls (n = 40) were compared according to the dominant and lymphedema involvement sides. The consort diagram of the study is shown in Figure 3.
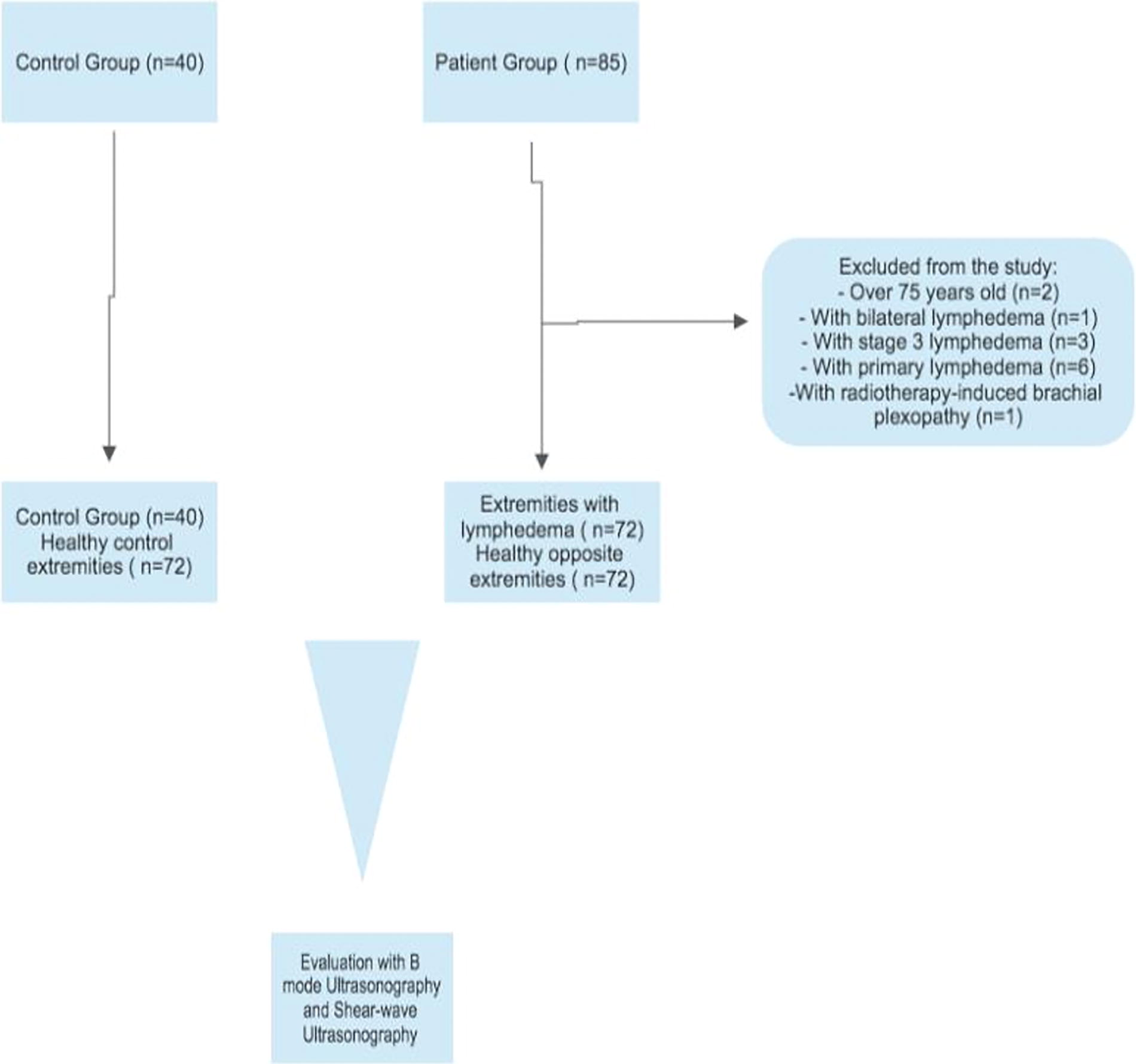
The consort diagram of the study.
Demographic and clinical features
The mean ages of the patient (54.89 [9.25]) and control group (51.58 [8.93]) were similar (p = 0.069). No significant difference was found between the Body Mass Index (BMI) values of the patients (31.10 [4.53]) and the control group (29.47 [4.99]) (p = 0.081). Among the patients, 37 (51.4%) had lymphedema in the right extremity, while 35 (48.6%) had it in the left. Of the patients, 68 (94.4%) had a dominant right extremity, while 4 (5.6%) had a dominant left. Thus, 39 (54.2%) of the patients had the lymphedematous extremity as their dominant one, while 33 (45.8%) had it as their nondominant. When evaluating the duration of lymphedema in the patients, the median value was determined as 7 years (4–10). In terms of lymphedema stages, when assessed; 28 (38.9%) patients were in the latent stage, with 10 (13.9%) in stage 1, and 34 (47.2%) in stage 2, making a total of 44 (61.1%) patients in the clinical stage. While 45 (62.5%) of the patients underwent modified radical mastectomy, 27 (37.5%) underwent breast-conserving surgery. Axillary lymph node dissection was performed in only 68 (94.4%) of the patients. Of the patients, 63 (87.5%) received radiotherapy, and 66 (91.7%) received chemotherapy. When evaluating the volume difference between the two extremities of the patients, the median value was determined as 268.37 mL (89.36–622.11).
Elastographic Measurements
When patients’ lymphedematous and healthy extremities were compared, forearm skin stiffness was higher, and subcutaneous tissue stiffness of the arm and forearm was lower in the lymphedema extremities. When the patient group was compared according to stages, a significant decrease was observed only in subcutaneous tissue stiffness in the forearm.
When the patient group was compared with the control group, arm, and forearm skin stiffness was significantly higher in patients with lymphedema; arm and forearm subcutaneous tissue stiffness was significantly lower in patients with lymphedema (p = 0.036).
The comparison of these measurements of patients’ healthy and lymphedema arms and forearms according to stages and between the patient and the control group are summarized in Table 1.
Elastographic Measurements
p-value less than <0.05 is typically considered to be statistically significant.
IQR, Interquartile Range; SD, Standard Deviation.
The results of multiple comparisons of elastography findings between the control group and patients with latent and clinical lymphedema stages, as well as the results of pairwise comparisons with post hoc analysis, are shown in Table 2.
Comparison of Elastographic Findings Between the Control Group and Patients with Latent and Clinical Lymphedema Stages
IQR, Interquartile Range; SD, Standard Deviation.
Clinical stage 3 patients were not included in our study. Since one of the main aims of our study was to identify patients before the development of clinical findings, the main evaluation focused on differentiating the latent stage from the clinical stage. Since the number of patients in the group decreased when the clinical stages were staged within themselves, the evaluation was made as a comparison of latent and clinical stages.
The skin and subcutaneous tissue stiffness of the healthy extremities of the patients and the control group were compared in Table 3. Arm and forearm skin stiffness and forearm subcutaneous tissue stiffness were significantly higher in the healthy arm of the patients than in the control group (p < 0.001).
Comparison of Elastographic Findings Between the Unaffected Side of Patients and the Control Group
IQR, Interquartile Range; SD, Standard Deviation.
Intraobserver and interobserver reliability
In the interobserver reliability evaluation of SWE with 20 patients; Intra-class Correlation (ICC) values were 0.712, 0.922, 0.763, and 0.921 for arm skin, arm subcutaneous tissue, forearm skin, and forearm subcutaneous tissue, respectively.
In the intraobserver reliability evaluation of SWE with 10 patients; ICC values were 0.900, 0.946, 0.943, and 0.878 for arm skin, arm subcutaneous tissue, forearm skin, and forearm subcutaneous tissue, respectively.
Relationship of elastographic parameters with demographic and clinical parameters of patients
Arm subcutaneous tissue stiffness with difference in BMI (p = 0.006) and volume difference (p = 0.032); forearm subcutaneous tissue stiffness was significantly negatively correlated with volume difference (p = 0.018).
Relationship of elastographic parameters and volume difference with patients’ symptom, functionality, and QOL parameters
Arm skin stiffness was not correlated with any parameter. Arm and forearm subcutaneous tissue stiffness was found to be negatively correlated with Quick-DASH and Life Impact Scale (LIS), while forearm skin stiffness was found to be positively correlated. When looking at the patients’ relationships with their symptoms; arm subcutaneous tissue stiffness was negatively correlated only with the patients’ feeling of heaviness, forearm subcutaneous tissue stiffness was negatively correlated with tightness, heaviness, and stiffness symptoms, and forearm skin stiffness was positively correlated only with the feeling of tightness. Based on the fact that the patients’ forearm skin stiffness was significantly higher and their subcutaneous tissue stiffness was significantly lower than the control group, the relationship between the forearm skin/subcutaneous tissue stiffness ratio and symptom, functionality, and QOL parameters was evaluated. The patients’ Quick-DASH and LIS scores were found to be positively correlated with feelings of tightness, heaviness, and stiffness.
The findings are summarized in Table 4.
Relationship of Elastographic Parameters and Volume Difference with Patients’ Symptom, Functionality, and QOL Parameters
QOL, quality of life; DASH, Disabilities of Arm, Shoulder, and Hand.
Volume difference was correlated with Quick-DASH (r = 0.268, p = 0.024) and LLIS (r = 0.380, p = 0.01); There was no relationship between volume difference and symptoms (p > 0.05).
The role of elastography in the diagnosis of lymphedema
Predictive values, sensitivity, and specificities for differentiating all lymphedematous extremities from intact extremities and also lymphedematous extremities in the latent stage from intact extremities were evaluated separately for both arm and forearm, skin, and subcutaneous tissue by ROC curve analysis. However, in the ROC curve analyses, the predictive values, sensitivity, and specificity values were found to be significantly higher only for forearm subcutaneous tissue.
When the lymphedema and healthy extremities of the patients were compared, forearm subcutaneous tissue stiffness was significantly lower in the lymphedema extremity compared to the healthy side, and this significance was also valid for patients in the latent stage.
The cutoff value of subcutaneous tissue stiffness of the forearm with lymphedema in differentiating lymphedema from the intact arm was <9.3 kpA, with a sensitivity of 73.7% and a specificity of 67.9%.
The predictive value of forearm subcutaneous tissue stiffness with lymphedema in distinguishing latent lymphedema from the healthy arm was <11 kpA, with a sensitivity of 67.9% and a specificity of 60.7%.
Discussion
The primary outcome measures of this study were to measure the skin and subcutaneous tissue stiffness with SWE and then to compare all these measurements with the healthy extremities of the patients (by dividing it into latent and clinical phases) and the control group. The secondary outcome measures were the evaluation of the relationship between the parameters evaluated SWE, and clinical findings included pain, tightness, heaviness, and stiffness scoring, Quick-DASH, and LLIS.
When the stiffness parameters were evaluated in this study, in general, the skin stiffness of the lymphedema side was found to be higher, and the subcutaneous tissue stiffness was found to be lower. Lymphedema is a multicellular complex tissue response that develops due to a series of injuries. Fibrosis is stimulated in lymphedema, which is a chronic inflammation. Many factors such as the presence of subcutaneous fat tissue, fibrosis, and edema are added. 11 Since the propagation speed of the wave is measured in SWE, the speed and propagation will be expected to decrease within this entire complex structure. It is not surprising that fibrosis increases skin hardness, while edema and fatty tissue in the subcutaneous tissue decrease hardness.12,13 What is surprising here is arm and forearm skin and forearm subcutaneous tissue stiffness were also found to be increased in the healthy side of the patients compared to healthy controls; this result suggested that breast cancer-related surgery and treatment modalities that may cause fibrosis, such as radiotherapy, may also play a role in the development of stiffness.14,15 However, the correlation found between the degree of skin stiffness and the stage of the lymphedematous arm reflects the impact of lymphedema on tissue stiffness, also.
This situation shows us that many factors affect the process, and each complicates the situation. In addition, the increase in stiffness observed on the unaffected side may also be considered as another reason for the more frequent use of that side.
The data in the present study were compatible with many studies in the literature about the lymphedematous side. Suehiro et al. showed in 18 patients with lower extremity lymphedema that skin and subcutaneous stiffness by compression elastography was lower in lymphedematous limbs than in unaffected limbs. 16 Lim et al. evaluated skin and subcutaneous tissue stiffness by compression elastography in 39 upper extremities with postmastectomy lymphedema and reported lower stiffness in extremities with lymphedema. 17 Hayashi et al. compared retrospective, qualitative elastography data and indocyanine green lymphography in 18 patients with lower extremity lymphedema. Similarly, elastography values were found to be lower in the extremity with lymphedema. 18
In another study by Hashemi et al. using strain elastography, all strain measurements from the lymphedematous extremity were found to be lower than those from the unaffected extremity. 12
In another study in which lymphedema stiffness was measured with SWE in kPa, subcutaneous tissue stiffness in the lower extremities of patients with lymphedema was found to be lower than unaffected extremities, similar to this study. After the intensive decongestive treatment was applied to the lymphedematous extremity, it was determined that the stiffness of these tissues increased. This situation was attributed to reduced edema and fluid in the subcutaneous tissue with the treatment applied. 13
There are two other studies that emphasize that their results are different from this study, 13 and that their results are different from the present study, but their measurement method and method are very similar to the present study. However, although evaluation was made with SWE in these two studies, the measurement units are m/sec, not kPa.
In one of them, stage 1 and 2 lymphedema patients were evaluated by Iyigün et al., The latent stage was excluded from the study because it was not possible to detect the patients clinically and stage 3 lymphedema because it was very easy to detect clinically. In their study, they determined that elastographic evaluation of the forearm subcutaneous tissue could be used to differentiate stage 1 and stage 2 lymphedema. And it was predicted that 1.78 could be used as a cutoff value to differentiate the stages. However, in this study, no statistically significant difference was found between the lymphedematous arm and the unaffected arm of stage 1 patients; therefore, it was also stated that SWE could not be used in the detection of early lymphedema (in this study, stage 1 is meant as an early stage). 10 In the current study, unlike this study, latent stage lymphedema patients were included in the study and the data of these patients were compared with the data of patients with clinical lymphedema (stages 1–2) and it was shown that the skin stiffness of patients with clinical lymphedema increased and subcutaneous tissue stiffness decreased compared to latent stage patients. In addition, in contrast to the study by Iyigün et al.; in the current study, it was found that the stiffness of the forearm subcutaneous tissue of the forearm of the extremity with lymphedema decreased significantly in the latent patient group compared to the unaffected side and that a forearm subcutaneous tissue stiffness <11 could be used to detect the latent stage with a sensitivity of 67.9% and a specificity of 60.1%. In the study of Iyigün et al., tissue stiffness was found to be higher in the lymphedematous extremities against to the unaffected extremities. It is not discussed that Iyigün et al. found a finding different from the literature in their study. Only studies with similar results were evaluated. 10
In the other study, Polat et al. investigated the role of SWE in the diagnosis of lymphedema and its usability as a reference standard in early lymphedema. Three groups including clinical stage, latent stage, and normal group without lymphedema were included in the study. No significant difference was found between the three groups in terms of skin and subcutaneous tissue stiffness. While in patients with lymphedema in clinical stages (stages 1–2), arm and forearm skin and subcutaneous tissue stiffness were found to be higher than on the unaffected side, in the patients with latent lymphedema only forearm skin and subcutaneous tissue stiffness were higher than the unaffected side. Skin and subcutaneous tissue stiffness of the forearm with lymphedema was found to be higher in the latent group, but no difference was found in the lymphedematous arm compared to the unaffected arm. 2 In the present study, it was shown that in clinical lymphedema, the stiffness of the skin of the arm and forearm was higher and the subcutaneous tissue stiffness was lower than the unaffected arm. In the latent phase, forearm subcutaneous tissue was found to be lower than the unaffected side. The finding of stiffer subcutaneous tissue in the study of Polat et al. and softer subcutaneous tissue in the current study may be related to the complex pathophysiology of lymphedema and the fact that both fibrosis and fluid increase accompany the lymphedema process. It may be related to the heterogeneous structure of the subcutaneous tissue in patients with stage 2 lymphedema, especially in patients with stage 2 lymphedema due to the increase in fluid between the tissues in the early period and the increase in fibrosis in the late periods. In the study of Polat et al., both arm and forearm skin and subcutaneous tissue thickness and arm and forearm stiffness were found to be higher than the unaffected arm when the extremity measurements of lymphedema in clinical stages (stages 1–2) were examined. In the current study, forearm and arm skin stiffness were found to be high in the clinical lymphedema stages in accordance with this study, but unlike this study, forearm and arm subcutaneous tissue stiffness was found to be low. In the study of Polat et al., the fact that the stiffness increased only in the forearm in the early period was defended as lymphedema affected the forearm in the early stage and started to affect the arm as the condition progressed. 2
All this contradictory data of studies evaluating tissue stiffness in lymphedema extremities in the literature may be related to technological problems and variable methodologies, such as the number of ROI areas measured, the size of the ROI area, and the diversity of the population group included in the studies. These incompatibilities in the literature were extensively discussed in the study of Zarrad et al. And, as we mentioned above, these incompatibilities are attributed to the characteristics of the elastography device used in each study and the differences in the ROI area evaluated. 13
However, compared to studies in the literature, the high number of patients in this research and the comparison of lymphedema extremities with both healthy extremities of patients and healthy controls increase the reliability of the data. In addition, the fact that the SWE assessment was evaluated within and between observers in this study and the high reliability of these values increases the accuracy of these data.
In the current study, when the ultrasonography measurements of the patients were evaluated, it was found that all measurements made from the upper extremities of the patients with lymphedema were thicker than both their unaffected sides and healthy controls. This increase in thickness was found to differ between latent and clinical stages. These results were also consistent with the literature. In a study by Suehiro et al., the upper extremity lymphedema was evaluated; lymphedema side thicknesses were found to be higher, and this increase was found to be more pronounced in forearm measurements. 19 Forearm lymph circulation is less drained than arm lymph circulation, with the forearm having less connection with the lymphatic drainage to the deltoideopectoral and/or supraclavicular lymph nodes. For these reasons, and with the effect of gravity, it was thought that fluid and cells accumulated in the forearm. 19
Similarly, in this study, the decrease in stiffness only in the forearm in the early clinical stage (latent) supports the theory that lymphedema initially affects only the forearm and as the clinic progresses it begins to affect the arm.2,19 Previous studies have shown that extremities affected by lymphedema exhibit increased skin thickness.20,21 As lymphedema advances, the dermis becomes thicker due to an increased number of fibers, with tissue projections extending both toward the epidermis and into the subcutaneous layer. In addition, the skin may thicken further due to edema, leading to an enlargement of the subepidermal low-echogenic band. 22
When the studies comparing the volume difference with the patients’ symptoms and QOL are evaluated; although these parameters were found to be interrelated in some of the studies,23–25 in another part of the studies, both of which included a very high number of patients, similar to the present study, it was emphasized that the presence of symptoms of the patients should be taken into consideration rather than the lymphedema severity and volume difference,26,27 and it was found to be more associated with symptoms and the number and severity of symptoms rather than the volume difference of the patients are more important for the patients’ QOL. 27
In this study, clinical staging was performed, and severity grading based on volume measurement was not carried out. However, the relationship between volume measurement difference and SWE data was evaluated, and a low-level correlation was found between the decrease in subcutaneous tissue stiffness in the arm and forearm and the increase in volume difference. The reduction in subcutaneous tissue stiffness is associated with increased interstitial fluid in the pathophysiology of lymphedema, and the increased fluid could also lead to an increase in volume difference.
This study determined that the patients’ lymphedema symptoms, functionality, and QOL deteriorated, primarily as forearm skin stiffness increased and forearm subcutaneous tissue stiffness decreased. The increase in the ratio of skin stiffness to subcutaneous tissue stiffness was associated with this worsening at a higher level. These relationships of clinical parameters with stiffness parameters were more evident than their relationships with volume difference. Stiffness and clinical parameters may be better than volume change as the primary outcome measure in research and clinical follow-up of patients.
The strengths of the study are the high number of patients with classification according to stages and the control group, which is similar in terms of both healthy sides and BMI and age. This study is the first to evaluate the relationship of elastographic parameters with clinical functionality and QOL. Again, the study is the first to assess the involvement of the unaffected extremity in the group of patients with breast cancer-related lymphedema and indeed found that it is affected.
The limitations of the study are that the measurements cannot be made blindly, and the patient group who was operated for breast cancer but did not develop lymphedema was omitted.
Conclusion
This study showed that elastographic measurements may be helpful in diagnosis, even in patients in the latent stage. The relationship of elastographic parameters with lymphedema-related symptoms, functionality, and QOL reveals that SWE is crucial in treating patients with lymphedema. It may provide an advantage in clinical practice and the evaluation of treatment response in research. Compared to other measurement methods, it is easy to apply, inexpensive, fast and noninvasive, safe.
Declarations
Informed consent was obtained from all patients.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
There is no funding for this study.