
Abstract
Human cardiac troponin I (cTnI) is one of the most specific biomarkers for detection of acute myocardial infarction (AMI). To formulate immunoassay kits for rapid immunodiagnosis of AMI, monoclonal antibodies with high affinity and specificity were generated against cTnI and subsequently tested through a series of experiments. C57BL/6 mice were immunized with cTnI as the immunogen and cell fusions with myeloma cells of BALB/c origin were performed to generate hybridomas. The supernatants of the hybridoma cell culture were routinely screened for antibody secretions against intact cTnI and synthetic peptides from the N-terminal half of cTnI (amino acid residues N1-30, N24-40, N59-79, and N80-95). Monoclonal antibodies specific to different epitope regions were then determined and selected, according to their respective affinity and specificity, for formulation of enzyme immunoassay kits. The results of this study found that most of the selected antibodies revealed comparable binding affinity to cTnI and to the corresponding synthetic peptides. Optimal sandwich enzyme immunoassays with high sensitivity could be achieved through proper combinations of the epitope-distinct monoclonal antibodies in different capture-detection pairs; signal enhancements were frequently observed when a mixture of epitope-distinct anti-cTnI monoclonal antibodies was used for coating. This indicates that a combination of epitope-distinct anti-cTnI monoclonal antibodies recognizing the N-terminal half of cTnI yield reliable detection and greater sensitivity for cTnI in AMI patients.
Introduction
T
Because of the tissue-specific expression of cTnI in the heart tissue, cTnI has been utilized as a marker for cardiac damage. For the past two decades, cTnI has been established as one of the most specific biomarkers for diagnosis of acute myocardial infarction (AMI).(3) In normal healthy patients, levels of cTnI are very low, while in AMI patients, cTnI levels are elevated. Therefore, cTnI is widely used in the clinical setting for differential diagnosis of patients presenting with chest pain.(4) Early detection of higher than normal levels of cTnI in the bloodstream and diagnosis of AMI are necessary in order to guide time-sensitive decisions in patient management and to decrease the number of missed AMI cases.
Given the urgent need for a highly sensitive cTnI assay for early detection of AMI, antibodies of high affinity and specificity are desirable for the formulations of rapid and sensitive immunoassays. However, complications arise from the instability of cTnI in the human circulation following AMI onset.(5–10) It is generally accepted that cTnI released from the cardiac muscle exists primarily in complex with troponin C (TnC) and troponin T (TnT), together known as the ITC complex, as well as in high degrees of heterogeneity in the human blood.(6) Purified cTnI is highly susceptible to proteolytic degradation, but within the ITC complex the central part of cTnI is protected from proteolysis due to the binding of TnC. Therefore, the most stable part of cTnI is located between amino acid residues 30 and 110.(5) Furthermore, lack of conformational stability of matrix cTnI in the ITC complex results in the generation of monoclonal antibodies reacting with mainly the linear epitopes of N-terminal half (N1-110) of cTnI.
In view of our current understanding of the specificity of cTnI, early detection of cTnI in the human blood by highly sensitive immunoassays allow the identification of AMI patients within the first 1–3 h, thus making cTnI an early marker of AMI.(11,12) In this communication, anti-cTnI monoclonal antibodies of high affinity and specificity were generated and their epitopes mapped to formulate immunoassays for reliable and sensitive clinical detection of cTnI among AMI patients.
Materials and Methods
Chemicals
Unless otherwise specified, all chemicals and reagents were obtained from Sigma Chemical Co. (St. Louis, MO).
Clinical specimens
Most of the frozen clinical serum specimens from the normal non-AMI control and AMI patients were provided by Lake Arrowhead Laboratory Consultants (Blue Jay, CA). Minor clinical patient serum specimens were obtained from the Department of Cardiology at the Vancouver General Hospital (Canada).
Troponin I isoforms and synthetic peptides
Purified cTnI (free form) and other cTnI isoforms were obtained from Scripps Laboratories (San Diego, CA). Purified troponin I-T-C complex was purchased from BiosPacific (Emeryville, CA). Oligopeptides corresponding to different parts of cTnI amino acids (N1-30, N24-40, N59-79, and N80-95) were synthesized by GenScript (Piscataway, NJ).
Production of monoclonal antibodies to human cardiac troponin I
A preliminary report for the generation and production of monoclonal antibodies against cTnI has been published previously.(13) Basically, more monoclonal antibodies were generated by using the same methodology with minor modifications and improvement. The emphasis is placed on the identification of high affinity monoclonal antibodies reacting with epitopes specifically in the N-terminal half of cTnI. These monoclonal antibodies were mapped by using specific synthetic peptides of cTnI located in the N-terminal half of cTnI (N1-30, N24-40, N59-79, and N80-95) (see Fig. 1).
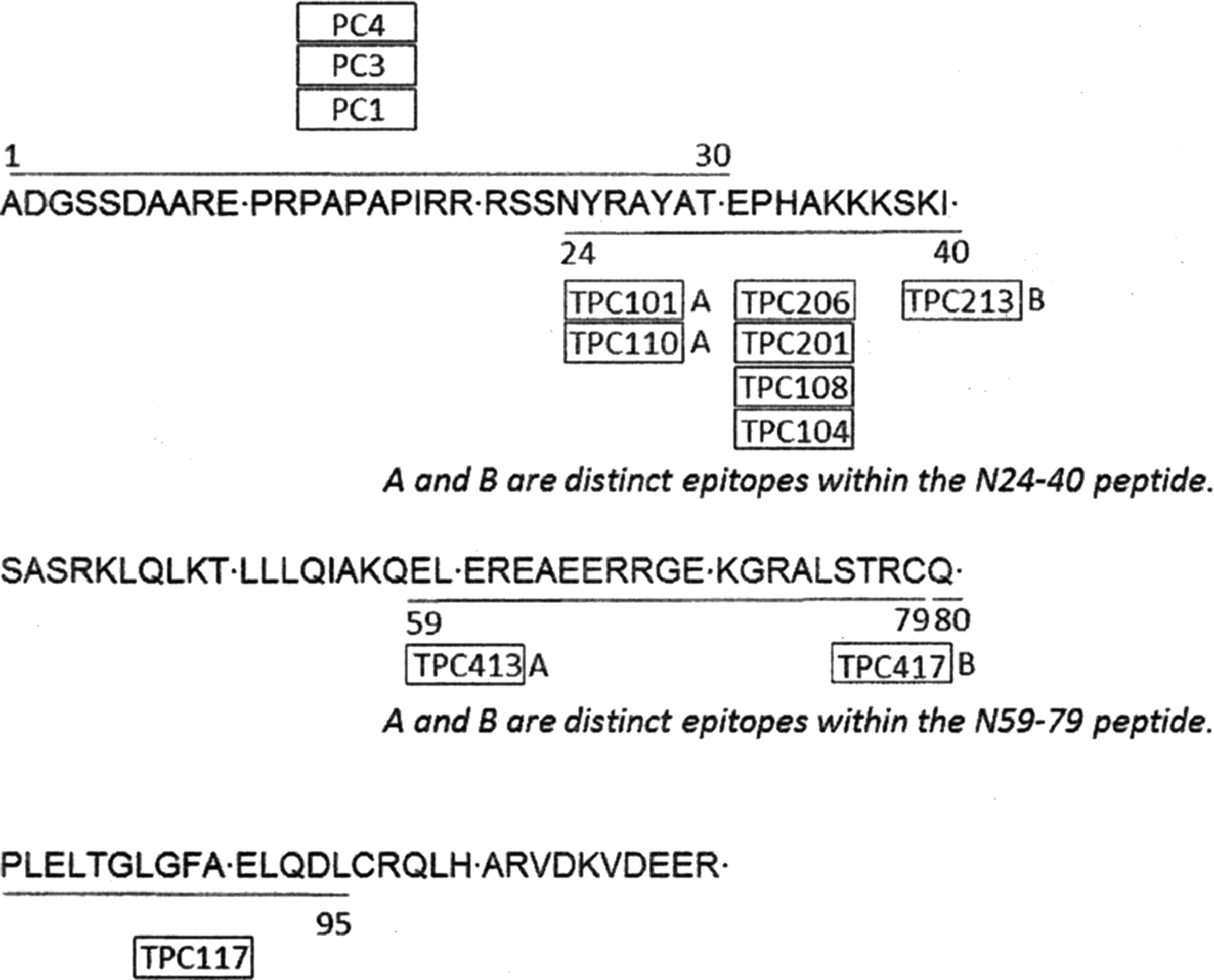
Epitope locations recognized by the generated monoclonal antibodies for human cardiac troponin I (N1-110). N24-40A and N24-40B are two distinct epitopes recognized by two separate monoclonal antibodies. Same observations were made with those of N59-79A and N59-79B.
For final formulations of enzyme immunoassay kits to achieve desirable assay sensitivity, various mixtures of epitope-distinct monoclonal antibodies were selected for capturing and signal detections (described in the Results section). Enzyme immunoassays were performed by using standard protocols, as described previously. cTnI standards from human heart extract were calibrated against the kit obtained from HyTest (Turku, Finland).
Results
Generation and characterization of monoclonal antibodies against distinct epitopes of human cardiac troponin I
Based on previous experience in our laboratory, C57BL/6 mice were used for immunizations with cTnI followed by cell fusions with myeloma cells of BALB/c origin.(13,14) This resulted in a higher immune response and higher yields of anti-cTnI positive hybridomas. Therefore, more than ten cycles of cell fusion experiments were performed with thousands of hybridomas generated and routinely screened for secretion of anti-cTnI monoclonal antibodies. Special attention was paid to those that reacted with synthetic peptides (N1-30, N24-40, and N80-95) derived from the N-terminal half (N1-110) of cTnI molecules.
Based on their respective epitope specificity, a group of anti-troponin I monoclonal antibodies were identified and are listed in Table 1. The relative epitope locations recognized by these monoclonal antibodies are also presented for comparisons. Some were shown to recognize amino acid residues N1-30 of cTnI (PC1, PC3, and PC4). Seven were specific to the epitopes located on the N24-40 peptide, while the other two recognized the N59-79 peptide, and one reacted with the epitope region on the N80-95 peptides. The epitope regions of the remaining four have not yet been unambiguously assigned.
N24-40A and N24-40B are two distinct epitopes recognized by two separate monoclonal antibodies. The same observations were made with those of N59-79A and N59-79B.
ND, not determined; TBD; to be determined.
Cross-reactivity between the selected monoclonal antibodies and two of the TnI isoforms from fast twitch and slow twitch skeletal muscle were also examined through typical binding ELISA.(15) It was clearly demonstrated that the selected monoclonal antibodies specific to these selected N-terminal half epitope regions displayed little cross-reactivity to any of these two skeletal muscle TnI isoforms. Therefore, all were considered to be highly specific to cTnI.
Relative dissociation constants of some of these monoclonal antibodies to cTnI were determined through typical binding assays with micro-wells coated with cTnI antigen derived from human heart extract. The dissociation constants of selected high affinity monoclonal antibodies were estimated and are presented in Table 1 for comparative purposes. Among the selected antibodies, the dissociation constants (Kd) range from 0.37 nM for TPC110 to 1.9 nM for TPC117. The relative affinities of the selected monoclonal antibodies to cTnI were found to be slightly better than those from commercial sources. For example, under our routine assay conditions, HyTest 9C17 and 8E10 were shown to have Kds of 1.8 nM and 8.6 nM, respectively. On the other hand, Medix 9701, 9703, 9705, and 9707 have Kds ranging from 1.3 to 4.3 nM.
By means of competitive binding experiments, the relative pairings between any two monoclonal antibodies can be assessed. As described in Table 1, two distinct epitopes exist in either the N24-40 or N59-79 synthetic peptides as each peptide can be recognized by two separate monoclonal antibodies. Therefore, the binding signals can be enhanced when both epitope-distinct antibodies in the same epitope region are paired. They can also pair simultaneously with a third antibody located in other epitope regions. For example, TPC101 (N24-40A) or TPC110 (N24-40A) can be paired with TPC213 (N24-40B) for sandwich immunoassay. Similarly, TPC413 (N59-79A) and TPC417 (N59-79B) can be mutually paired. The relative locations of these distinct epitopes recognized by the selected monoclonal antibodies along the N-terminal half of cTnI amino acid sequences were determined and are presented diagrammatically in Figure 1.
Since TPC101 and TPC110 have relatively high affinity to cTnI, either one can be conjugated with HRP for signal detection in a sandwich enzyme immunoassay. For capturing cTnI, the micro-wells can be coated with one to four epitope-distinct monoclonal antibodies to increase the assay sensitivity. Based on this assumption, proper combinations of the selected anti-cTnI monoclonal antibodies can result in the desirable assay sensitivity for early detection of AMI patients. The results of such pairing combinations are listed in Table 2.
Typical assay conditions are described in text.
During pairing experiments with various mixtures of epitope-distinct anti-troponin I monoclonal antibodies, it was noted that signal enhancement was obtained upon combinations of two or more antibodies in a typical sandwich enzyme immunoassay. Results of such examples are shown in Table 3. When TPC417 was mixed equally with TPC117, TPC213, or TPC413, significant signal enhancement was observed in each case.
Wells were coated with 10 μg/mL of each antibody indicated on x and y axes. Values given are those achieved with 3.3 ng/mL of cTnI following 30 min co-incubation at 37°C with horseradish peroxidase-labeled TPC101 and subtraction of the blank.
Numbers in brackets ([ ]) designate values obtained from well coating with 10 μg/mL of a given antibody and 10 μg/mL of normal mouse IgG.
Judging from such analyses, an assay sensitivity of 0.10–0.15 ng/mL cTnI can be achieved by a typical enzyme immunoassay within 30–45 min of total incubation time at room temperature. A typical standard curve of this sandwich enzyme immunoassay is presented in Figure 2.
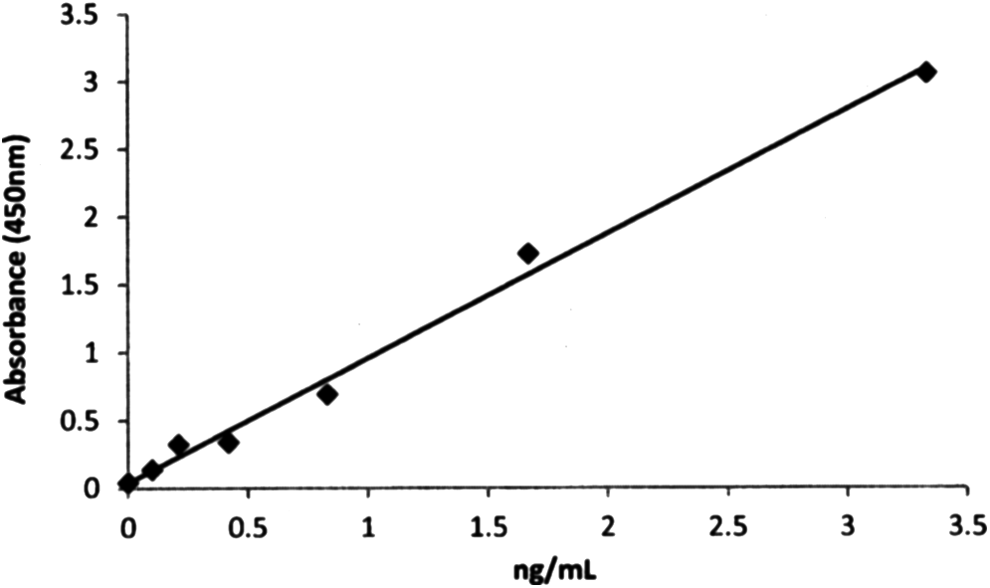
Typical standard curve of cTnI with a mix of TPC117, TPC213, and TPC413 as the capturing antibody and TPC101 as the detection antibody. Wells were coated with 20 μg/mL total of TPC117, TPC213, and TPC413. Serial dilution of cTnI was performed with 30 min co-incubation at room temperature horseradish peroxidase-labeled TPC101.
Clinical correlation studies
A combination of three epitope-distinct monoclonal antibodies (TPC117, TPC213, and TPC413) was used for coating as capturing antibodies on micro-wells. TPC110-HRP served as the detecting antibody. A typical sandwich enzyme immunoassay was employed to perform clinical correlation studies. The results are summarized and presented in Table 4. From these clinical correlation studies, it is clearly demonstrated that the assay results of the EIA kit formulated in this study are well correlated with those of Abbott's AxSYM, with correlation coefficients of 0.9018 for AMI cases and 0.8036 for non-AMI cases, respectively.
Discussion
According to the American Heart and Stroke Association, the estimated annual incidence of AMI in the USA in 2014 was 515,000 for new attacks and 205,000 for recurrent events. In addition, approximately 15% of patients, who experienced an AMI, died.(16) Therefore, early detection of AMI is crucial in order to guide quick medical treatment and intervention to AMI patients and prevent complications arising from AMI and patient death. Highly sensitive cTnI assays can aid in detecting AMI patients within 1–3 h after AMI onset and ensure prompt and accurate medical care.
In this study, a variety of anti-cTnI monoclonal antibodies were generated and selected. Our final selection of these antibodies was based on the assumption that the N-terminal half of cTnI is the most stable part of cTnI in human blood.(5,13) Other cTnI assays that have demonstrated superior clinical performance, such as Beckman Coulter's AccuTnI assay, also utilize monoclonal antibodies with epitopes in this region.(17) It is known that cTnI in human blood exists predominantly in a complex form with TnC and TnT, and does not have a stable and well-defined tertiary or conformational structure in the ITC complex.(6) Therefore, it is possible to identify more epitope-distinct monoclonal antibodies for cTnI than for other globular proteins that possess limited accessible epitopes.
It was also found that mutual pairings of anti-cTnI monoclonal antibodies in a sandwich enzyme immunoassay are possible when a pair of epitope-distinct monoclonal antibodies was used in the assay format. Furthermore, assay sensitivity can also be enhanced through a proper combination of epitope-distinct monoclonal antibodies, due to cooperative binding of the antibody mixture to the analyte.(18) Examples of such signal enhancement experiments can even be demonstrated with a mixed coating of two monoclonal antibodies, as demonstrated in Table 3. Therefore, the immunoassays can be performed with a combination of more than two mutually epitope-distinct monoclonal antibodies in order to achieve high assay sensitivity. The different epitope specificity of the monoclonal antibodies for cTnI may also play a role in determining clinical performance of the assay.(17)
In view of the fact that TPC110 shows one of the highest affinities to cTnI, it has been widely used by a number of major immunodiagnostics companies since 1999 as one of the key antibody components for rapid immune-detection of AMI.(13) Similarly, additional anti-cTnI monoclonal antibodies presented in this study are equally beneficial to AMI patients in terms of rapid immunodiagnosis of AMI. These antibodies may be useful for different assay platforms designed to detect cTnI.
Clinical correlation studies were also performed for the EIA kit formulated in this study and compared with that of Abbott's AxSYM system. The correlation coefficient obtained from such a study with 110 AMI cases was 0.9018, which is considered to be satisfactory for clinical applications and fulfills the requirements or route standard performance by the US Drug and Food Administration (K023505, K050644).
In conclusion, immunoassays designed with a combination of epitope-distinct anti-cTnI monoclonal antibodies recognizing the N-terminal half of cTnI yield reliable detection and greater sensitivity for cTnI in AMI patients. Therefore, these anti-cTnI monoclonal antibodies hold great potential in assisting healthcare workers in early diagnosis of AMI patients.
Footnotes
Author Disclosure Statement
The authors have no financial interests to disclose.