
Abstract
Among multiple parameters, applied in the immunologic monitoring of transplantation, the levels of serum soluble CD30 (sCD30) and peripheral regulatory T cells (Tregs) are very promising. These are relatively new biomarkers, considered to reflect immune activation and tolerance in solid organ transplantation. Results are shown here from a preliminary study on the relevance of sCD30 and Tregs in the monitoring of the early post-transplantation period. Sixteen patients with chronic liver or kidney disease were examined. Nine of them were further selected for transplantation. Follow-up of sCD30 and Tregs was carried out during the first month after transplantation. Until day 30 (D30) after transplantation, a progressive decrease in sCD30 levels was observed in all patients. Conversely, the dynamic of Tregs was dependent on the transplanted organ: in liver recipients, an increase of Tregs was detected at day 7 (D7) followed by a gradual decrease until D30, whereas in kidney recipients, a sustained downward trend starting on D7 was observed. In liver recipients, the increase in Tregs preceded albumin normalization, whereas in kidney recipients, sCD30 was found to have predictive significance for the creatinine levels. Our results demonstrated that peripheral blood sCD30 and Tregs are valuable parameters in the immunologic monitoring of transplanted patients.
Introduction
The greatest challenges in transplantation are the control of post-transplantation immune activation and the maintenance of the recipient's immune tolerance milieu. In the majority of cases, graft human leukocyte antigen molecules and alloantigens, being recognized as foreign, induce the generation of a huge number of activated T cells and macrophages into recipients causing graft rejection. This is usually manifested by elevated cytokines levels, T cell proliferation, increased cytotoxicity, and upregulated surface molecules in situ and in the circulation. Together with the lineage-specific molecules, expressed by immune cells upon activation, the molecule CD30 was found to be less cells specific but strongly activation dependent.(1) CD30 is a 120 kDa transmembrane glycoprotein, which belongs to the tumor necrosis factor/nerve growth factor receptor superfamily.(2) In healthy individuals, minimal levels of soluble CD30 (sCD30) can be detected in the peripheral blood. Upon cellular activation, CD30 undergoes enzymatic cleavage and sheds from the cell surface being released in the surrounding milieu and in the bloodstream.(3) In transplantation, high levels of sCD30 in the presence of donor-specific antibodies (DSA) were associated with graft rejection.(4)
Various mechanisms are involved in the conflict between the foreign antigens stimulating immune activation and the required induction of tolerance. These include immune cells, soluble factors, and so on. Usually, the quenching of this conflict is achieved by the application of immunosuppressive drugs. However, in some cases, a spontaneous tolerance was observed, so-called “operational tolerance.”(5) First described in kidney allograft survival, this phenomenon was found more frequently in liver transplantation.(6) In these cases, the immune system is able to control the immune activation by itself without pharmacological immunosuppression. Although immune tolerance is a multifactorial process, the prevention of allograft rejection is strongly associated with regulatory T cells (Tregs).(7)
Tregs were shown to control immune responses and to silence the excessive immune activation because of their particular molecular signature. Tregs are defined by the expression of the transcription factor FoxP3, which was found to modify gene expression profile of T cells.(8,9) The exact mechanism of Tregs suppressive function is still not fully understood. Multiple mechanisms were shown to be in use: direct contact with the target cell or dendritic cells,(10) secretion of suppressive cytokines such as TGF-b, IL-10, and IL-34, or release of perforins and granzymes.(11–13) Along with the direct effects on conventional T cells, Tregs indirectly reshape their activation manifestations by the concurrent consumption of IL-2(14) or affecting key cellular signaling mechanisms.(15)
In the present study, we investigated the peripheral blood levels and dynamics of sCD30 and Tregs in patients before and during the first 30 days after liver or kidney transplantation. Expressing two different arms of post-transplantation immunity—activation and tolerance, sCD30 and Tregs demonstrated a differential trend in liver and kidney transplantation. Correlations with specific serum biochemistry parameters suggest that sCD30 might have a predictive value for kidney transplantations, whereas the early increase of Tregs could be associated with an upcoming normalization of serum albumin (ALB) levels.
Patients and Methods
Study participants
Twenty-nine individuals were tested. Of them, 15 were age-/sex-matched healthy controls and 12 were with advanced liver (n = 4) or kidney (n = 8) chronic diseases. All patients with liver disease and five with renal diseases were subjected to transplantation. Two more patients with previous liver transplantation were also examined. Detailed subject characteristics are shown in Table 1. Patients were transplanted and monitored both clinically and in the laboratory in the first month of the post-transplantation period in the University Hospital “Lozenetz.” The evaluation of the main virological parameters—hepatitis C virus, hepatitis C virus, cytomegalovirus, and Epstein-Barr virus—did not show any changes from the baseline results, including IgM antibodies. Patient data collection was in accordance with the Declaration of Helsinki as revised in 2013.
Subjects' Demographic and Clinical Characteristics
Excluding criteria: chronic inflammatory diseases including infections, endocrine diseases, cancer, autoimmune deviations, and pregnancy.
Antibiotics.
Antimycotics.
AB, antibiotics; Amyc, antimycotics; F, female; HCV, hepatitis C virus; M, male; MMF, mycophenolate mofetil; NA, not applicable; NAFLD, nonalcoholic fatty liver disease; TCLM, tacrolimus.
Samples collection
Serum samples and peripheral blood mononuclear cells (PBMCs) were obtained from 6 mL of peripheral blood. PBMCs were isolated by Ficoll gradient centrifugation. sCD30 and Tregs were followed up on 0, 7, 14, and 30 days for transplanted patients and once for patients with chronic liver or kidney insufficiency without transplantation.
Quantitative measurement of sCD30 was carried out by a commercially available enzyme-linked immunosorbent assay (Human CD30 Platinum ELISA; Affymetrix, Thermo Fisher), according to the manufacturer's instructions.
Evaluation of Tregs was carried out by Human Regulatory T Cell Staining Kit (eBioscience, Thermo Fisher). Isolated PBMCs were stained with anti-human CD4 (clone RPA-T4) FITC and CD25 (BC96) APC cocktail, followed by a permeabilization step and blocking with normal rat serum. Intracellular staining was carried out with anti-human Foxp3 PE (clone PCH101). Rat isotype control PE (IgG κ1) was used to identify positive gate. Cells were acquired on a flow cytometer BDFACS Canto II and analyzed by software Diva 8.0.1.
Assessment of clinical biochemistry was performed as a part of the routine patient monitoring.
Statistical analysis was performed by the nonparametric Mann–Whitney test by GraphPad prism software, v.7, when applicable. In the text, in parenthesis, are shown mean values ± standard deviation for every parameter. p-Value <0.05 was accepted for statistically significant difference.
Results
Evaluation of sCD30 and Tregs in healthy individuals and patients with chronic diseases
The serum levels of sCD30 and Tregs in peripheral blood were measured in 15 healthy subjects (Table 1). The serum values of sCD30 were found between 0.51 and 72.33 ng/mL, and the mean value was 32.15 ± 19.60 ng/mL. The mean value of Tregs found was 5.57% ± 2.75%, range 2.8%–11.22%.
Sixteen patients with advanced-stage chronic liver or kidney diseases were studied in parallel. To get more relevant data, about chronic disease background, we also included nine patients on day 0 (D0) (i.e., before transplantation) of those, who followed a transplant of the respective organ (Table 1).
As shown in Figure 1A, the serum levels of sCD30 in all the patients were very high in comparison to the healthy control group (p < 0.0001). Separate analysis within each patients' group demonstrated a significant increase only in patients with kidney pathology (p = 0.03). Conversely, the percentages of Tregs were very low in all patients (p = 0.008) (Fig. 1B). For all of them, neither sCD30 nor Tregs values were found dependent on the background diagnosis and current therapy.
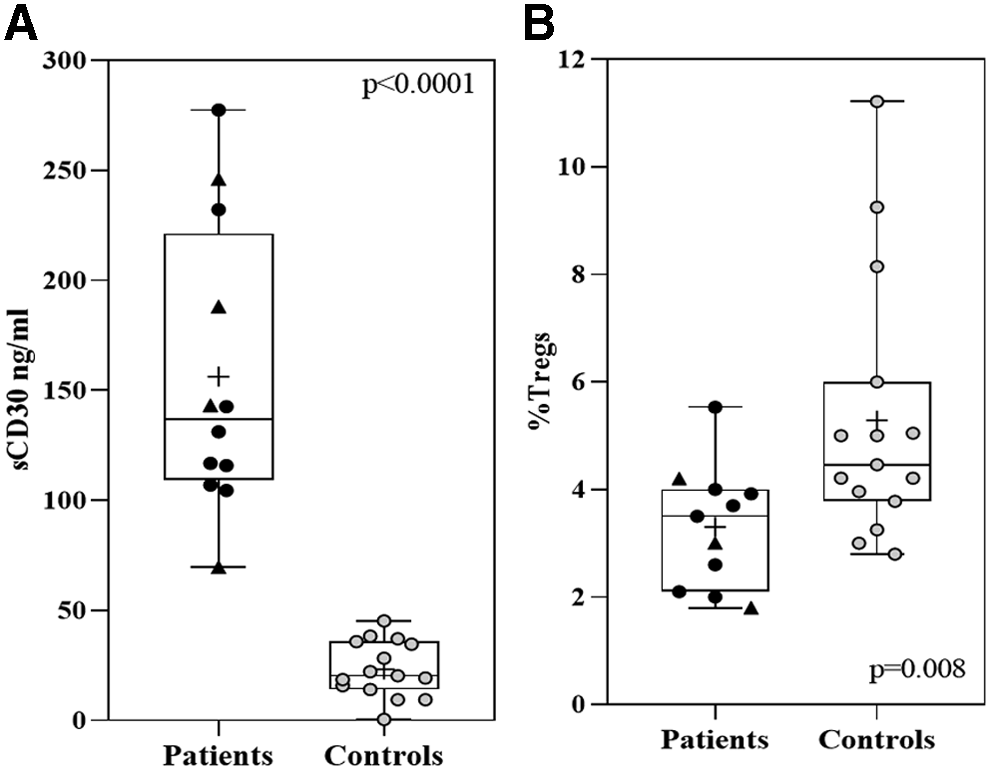
Evaluation of sCD30 and Tregs in patients and controls. Individual values are shown for sCD30
Post-transplantation dynamic of sCD30 and Tregs in patients with liver graft
All the patients with chronic liver diseases underwent transplantation during the study. They were followed on D0 (before transplantation) and on days 7 (D7), 14 (D14), and 30 (D30) after transplantation. Two other patients were evaluated for the same parameters later because of suspected late liver graft rejection.
In liver recipients, the levels of sCD30 were elevated on D0 compared with controls (161.73 ± 64.8 ng/mL vs. 32.15 ± 19.15 ng/mL, respectively), indicating high degree of immune activation. After transplantation, they decreased gradually until the end (D30) of the observation period, without reaching those in the control group (71.30 ± 32.00 ng/mL vs. 32.15 ± 19.15 ng/mL, respectively).
Interestingly, the percentages of Tregs increased at D7 more than twice in comparison to D0 (8.45 ± 2.12 vs. 3.0 ± 1.2, respectively). One week later (D14), a steep decrease was registered in all the liver transplanted patients (D14 = 4.44 ± 1.5). At the end of the first month (D30), the mean proportion of Tregs did not change, staying close to the control values (D30 = 4.21 ± 2.62 vs. controls = 5.57% ± 2.75%) (Fig. 2A).
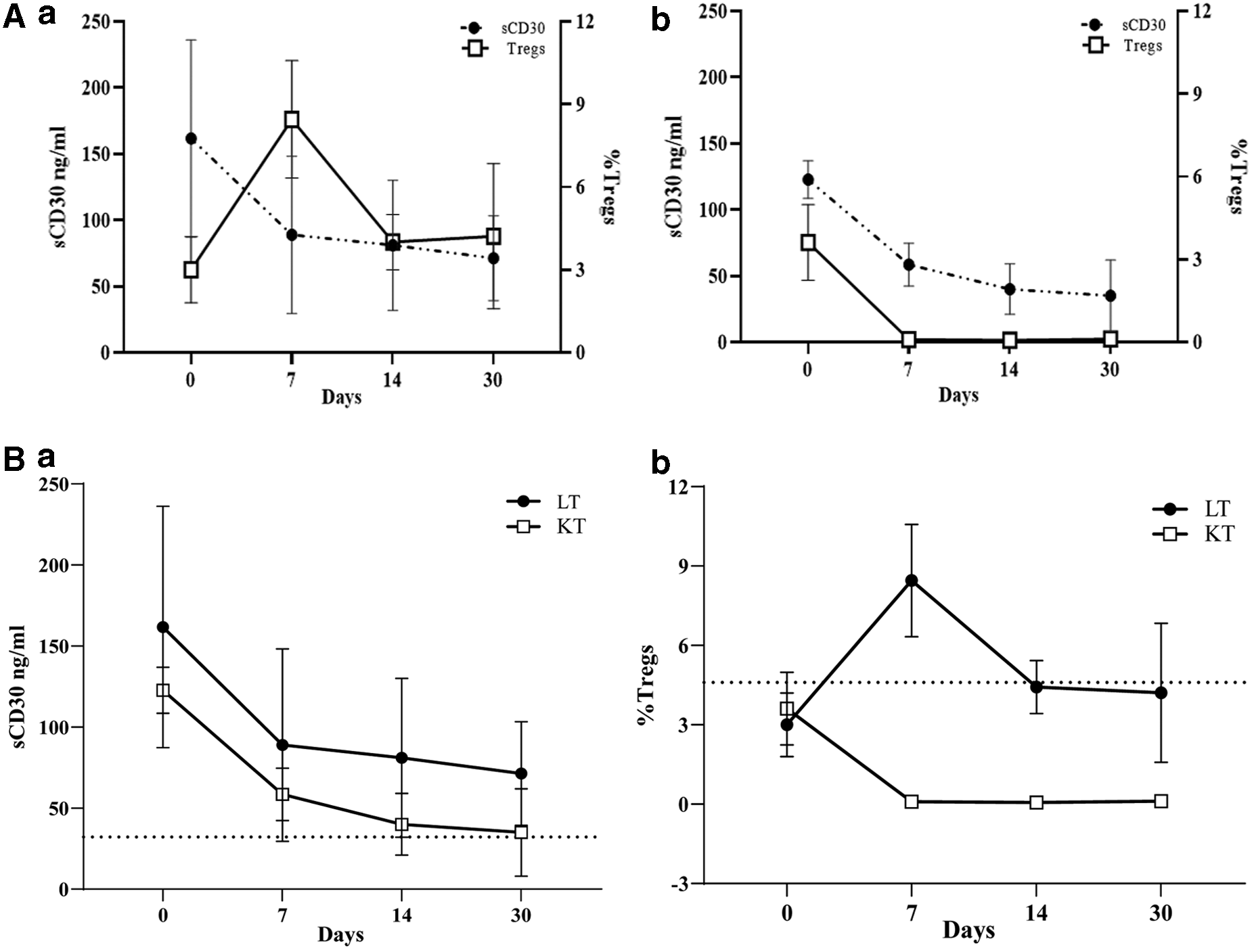
Evaluation of sCD30 and Tregs in peripheral blood from patients with liver and kidney transplantation. Variations in liver transplanted group are shown in
In addition, two patients, suspected for liver graft rejection, were examined. Both were on immunosuppressive therapy (IST) for a long time. In the first patient, transplanted in 2005, the examination showed sCD30 of 46.80 ng/mL (in the range of the control group) with very low Tregs of 0.3%. In the second patient (transplanted in 2014), the constellation was elevated sCD30 of 123.37 ng/mL and low Tregs of 0.9%.
Post-transplantation dynamic of sCD30 and Tregs in patients with kidney transplantation
Five of eight patients with chronic renal failure underwent kidney transplantation. Serum levels of sCD30 and Tregs were evaluated on D0, D7, D14, and D30; the baseline levels of sCD30 (D0) were more than twice higher than those in controls (122.71 ± 12.63 ng/mL vs.15 ± 19.15 ng/mL). At the end of the first week (D7), a substantial decrease was registered (57.35 ± 13.14 ng/mL). A stepwise decline was observed until D30, where values were within the range of the control group (D30 = 27.85 ± 15.30 ng/mL vs. 32.15 ± 19.15 ng/mL).
The parallel evaluation of Tregs showed, that before transplantation (D0), the percentage of Tregs was comparable with that of the control group (3.61 ± 1.22 vs. controls = 5.56% ± 2.57%) and with patients with ChRF without transplantation (3.34 ± 1.15). On D7, Tregs dropped sharply (0.09% ± 0.02%), and on D14, Tregs were below 1% and kept at a very low level until D30. In contrast to liver recipients, there was no elevation of Tregs on D7 in kidney recipients (Fig. 2B).
Clinical relevance of the dynamic of sCD30 and Tregs
We next asked the question of how the sCD30 and Tregs could be associated with some critical laboratory parameters. For liver transplanted patients, we evaluated serum transaminases, aspartate transaminase (AST) and alanine transaminase (ALT), and ALB. The small number of patients did not permit a precise statistical analysis. However, the trend of decline in serum levels of sCD30 and the increase in Tregs were associated with normalization of the enzymes activity, as measured by AST and ALT (Fig. 3A, C).
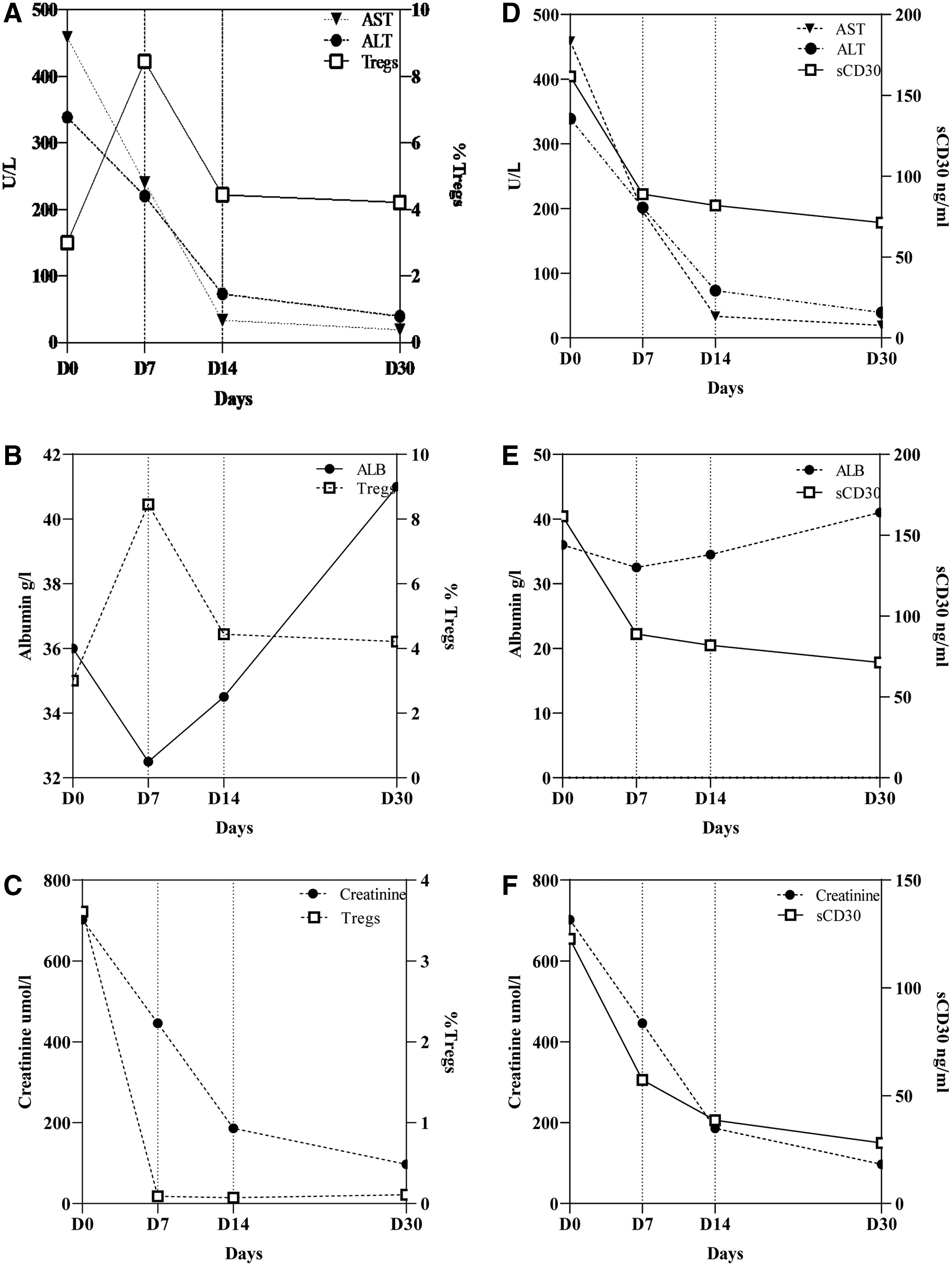
Relevance of sCD30 and Tregs to graft-specific laboratory parameters after transplantation. Graphics in (
The dynamic of ALB was different from that of AST and ALT. During the first postoperative week, the serum levels of ALB decreased, reaching their lowest point on D7. Afterward, in all the patients, the concentration of ALB gradually increased until D30. This dynamic corresponded well with the decreased levels of sCD30 and was associated with moderate variations in Tregs. As shown in Figure 3E and F, the sharp increase of Tregs on D7 preceded the improvement of ALB secretion.
Kidney graft function was assessed based on the serum creatinine levels and analyzed in connection with sCD30 levels and Tregs. While sCD30 was inversely associated with the serum creatinine levels (Fig. 3F), there was no such relationship for Tregs (Fig. 3E). Of note, the decrease of sCD30 preceded the normalization of creatinine levels in a way similar to this, found in ALB and Tregs.
Discussion
The selection of appropriate biomarkers for the immunologic monitoring in the post-transplantation period is still a subject of intensive discussions. Many parameters were shown to provide important information about the tolerance status of the recipient. Among them, sCD30 and Tregs are interesting because they mirror the paradigm of immune activation and immune tolerance in transplantation. Data in the literature showed that the low sCD30 levels are associated with high Tregs.(16) Similar results we obtained in the control group. Conversely, for all the patients with chronic disease, the levels of sCD30 were increased more than five times than those in controls and associated with very low Tregs. These results indicated not only the impaired balance between activation and tolerance in patients with chronic diseases and organ failure but also the limited capacity of the current therapy and/or dialysis to overcome the impaired immune balance. Hence, in such situations, the solid organ transplantation is considered to be the treatment of choice.
In our study, four patients with liver pathology and five with chronic kidney insufficiency underwent organ transplantation. During the early post-transplantation follow-up, we observed particular dynamics of both parameters that seem to be graft-dependent. Changes were more pronounced in Tregs, which in liver transplantation increased more than twice on D7 and then decreased, being at a higher proportion at the end of the first month. Conversely, in kidney recipients, Tregs decreased on D7 and remained very low till D30.
In both groups of transplanted patients, we found rapidly decreased immune activation shortly after transplantation, but not to the same extent. While in renal recipients all values were comparable with those in the control group, in liver recipients they remained above the controls until the end of the study.
Another question addressed by our study was whether the dynamic of sCD30 and Tregs reflects any aspect of the graft status and/or early post-transplantation graft function. Among multiple parameters routinely measured in this situation, the levels of serum transaminases AST and ALT are of particular importance, being associated with liver cytolysis. So, their elevation is indicative of probable liver dysfunction induced not only by toxin-induced liver injury but also by ischemic liver damage (ALT) and liver tissue degeneration and necrosis (AST).(17) Both mechanisms are considered in the post-transplantation period in connection with intensive effector immune response and impaired immune tolerance. Our results showed that the decreased activity of AST and ALT is parallel to those of immune activation, determined by the sCD30. We suggest that Tregs also might have an important contribution to this process, because the higher Treg cell in peripheral blood corresponds to the low transaminase values, for example, to the liver function in the early post-transplantation period.
Liver is known to have multiple important physiological functions. One of them is the synthesis of ALB, which is largely used as predictor for the outcome of many medical conditions and particularly of transplantation. Moreover, ALB mirrors the synthetic capacity of the liver and the liver graft. We found a decrease in ALB, below the baseline during the first week, probably because of the operative stress. At that moment, the decline of sCD30 started, which in the rest of the study went concomitantly with the improved ALB concentrations. The changes in Tregs are more pronounced. On D7, where Tregs increased sharply, ALB decreased, and on D14, it returned to the baseline levels with a tendency to increase until D30. It is likely that increased Tregs on D7 might influence the rapid establishment of immune tolerance, and facilitation and revitalization of the synthetic function of the liver. Data in the literature are controversial and do not provide consistent evidence about the dynamic of ALB. Instead, the ALB infusion is discussed as a routine therapy that theoretically can modify ALB concentrations for several hours.(18,19) That was not the case in our study, which allowed us to advise liver function improvement. For this reason, we suggest Tregs as an early biomarker in liver transplantation facing the graft function.
Our investigation confirms that Tregs could be an additional parameter for the assessment of kidney post-transplantation period and the graft function. We used creatinine as a laboratory parameter for kidney function. The drop of sCD30, but not of Tregs, preceded the decrease of serum creatinine in the first week (D7) after transplantation. Thus, our results are in agreement with several multicenter studies,(20–22) showing the rational for the implementation of sCD30 as a biomarker in kidney transplantation.
The impact of the IST should also be considered. The question is why the IST almost neutralized Tregs together with the immune activation, expressed by sCD30, in kidney, but not in liver recipients? The answer might be bidirectional—the IST combination in kidney transplantation was fourfold—calcineurin inhibitor (CNI), Mycophenolate mofetil (MMF), corticosteroids, and anti-CD25 monoclonal antibody (Basiliximab), whereas in liver transplantation, it was mild. Tacrolimus, as a CNI, not only impacts NF-AT dephosphorylation but also downmodulates IL-2 synthesis. The latter is indispensable for the survival and function of Tregs.(23,24) MMF has a powerful cytotoxic effect in activated T and B cells.(25) Regarding Tregs, data are controversial. Some studies showed that MMF hinders Tregs, whereas others described a positive effect due to the increased ratio Tregs/Th17.(26) This increase might be relative, as a consequence of the decreased Th17 cells.(27,28) Basiliximab was expected to negatively impact Tregs because of the CD25 blockade. It is associated with a transient reduction of CD25 expression, but not with the Tregs loss, we have observed.(29–31) In any case, there is a need to clarify how Tregs should be determined. In the literature, CD25 seems to be a disputable marker for Tregs—from association with loss of function in autoimmunity(32) to a reservoir of future Tregs with retained function.(33,34) Tregs are often considered as CD4+FoxP3+. This could be a reasonable approach, because FoxP3 defines their suppressive function. In this case, the evaluation of Tregs might be significantly more independent of the therapy. Another question is how to define Tregs: as percentage or count. Regarding the mechanisms of Tregs induction and the heterogeneity of the population, we have chosen the percentage as a more relevant parameter, although some authors have placed more reliance on the absolute cell count.(35)
The next direction that might explain differential dynamics of Tregs is the organ-specific immune characteristic. For example, the liver is less susceptible to rejection and the success rate in liver transplantations is high.(36) It has been shown that a substantial number of donor Tregs detach from the liver graft during perfusion and continue to migrate into the recipient after transplantation, suppress alloresponses, and may contribute in vivo to the chimerism-associated tolerance early after transplantation.(37)
In conclusion, our results show that the evaluation of sCD30 and Tregs mirrors the balance between immune activation and tolerance in transplantation. Their specific dynamic in the early post-transplantation period can be associated with the organ-specific immunologic background and prediction of the graft function development. Our pilot data indicate that the serum sCD30 and peripheral Tregs might be considered as valuable biomarkers in the early post-transplantation immunologic monitoring. Further investigations will clarify their significance in the late postoperative period.
Footnotes
Acknowledgment
This study has been funded by a research grant from Sofia University, contract 10-122/24.04.2018.
Author Disclosure Statement
No competing financial interests exist.