
Abstract
Sclerostin is a protein synthesized mainly by osteocytes whose function is to inhibit bone formation. A recent monoclonal antibody, Romosozumab, is able to block sclerostin. The aim of this meta-analysis is to compare the safety of Romosozumab with placebo and alendronate. Five randomized controlled trials that described the safety of Romosozumab in healthy men and postmenopausal women were analyzed. The measures to be compared were the number of adverse events and the number of serious adverse events. Specific results included injection site reaction, arthralgia, nasopharyngitis, and back pain. A total of 11,741 patients were included in this meta-analysis, in three different groups: Romosozumab, alendronate, and placebo. Significant differences were seen between the groups with regard to injection site reaction: 5.88% in the Romosozumab group versus 3.62% in the placebo group (Mantel–Haenszel [M-H] 1.54, confidence interval [95% CI] 1.22–1.96; p < 0.001) and 2.62% in the alendronate group (M-H 1.8, 95% CI 1.32–2.60; p < 0.001). In addition, patients treated with Romosozumab had significantly fewer total adverse events than the alendronate group (M-H 0.85, 95% CI 0.74–0.98; p < 0.05). In conclusion, Romosozumab may have lower adverse effects compared to alendronate and comparable to a placebo, except injection site reactions. Injection site reactions were more with romosozumab compared to alendronate and compared to the placebo as well. Romosozumab appears to have a similar safety profile to bisphosphonates.
Introduction
Osteoporosis is a systemic skeletal disease that increases the risk of fragility fractures in osteoporotic men and postmenopausal women.(1) This disease causes around 9 million fractures per year worldwide.(2) The antiresorptive drugs have been the first choice among the pharmacological options, as stated in the guidelines.(3) While evidence for bone protection in the short and medium term is high, there are concerns about long-term treatment.(4) Almost all bisphosphonates are associated with a high risk of adverse events such as osteonecrosis of the jaw, atypical femoral fractures, and atrial fibrillation.(4,5)
Denosumab and teriparatide offer an alternative approach for osteoporosis treatment; however, these drugs also have significant adverse events.(6–8) Despite the fact that denosumab offers an alternative approach to the treatment of osteoporosis, it is also an antiresorptive, and thus, it may have the same adverse events as bisphosphonates.(6) Teriparatide, a bone-forming agent, is often reserved for patients with a very high risk of fracture or those who have been previously exposed to bisphosphonate therapy. However, current data suggest that the clinical benefit of teriparatide might be reduced in patients transitioning from bisphosphonates compared with bisphosphonate-naive patients.(9,10)
Romosozumab is a humanized monoclonal anti-sclerostin antibody that has been shown to increase bone formation and reduce bone resorption.(11) The increased bone mass and strength in the absence of functional sclerostin has been observed in rodents and human beings affected by sclerosteosis and van Buchem disease. Recently effective neutralization of sclerostin with a monoclonal antibody has emerged as a novel therapeutic approach.(5,12) Several clinical trials and a meta-analysis have indicated that Romosozumab treatment is associated with increased bone mineral density (BMD).(13–19) However, the safety of this new drug is not well documented, and as a newly introduced drug, an assessment of adverse events is important.
Therefore, we undertook this systematic review and meta-analysis of randomized controlled trials (RCTs) to analyze the safety of Romosozumab in osteoporotic men and postmenopausal women. We compared RCTs of Romosozumab versus placebo or alendronate, and we evaluated the adverse effects reported in the studies, including major and minor events. In this way, the safety of romosozumab can be assessed with a level of evidence I for the first time.
Materials and Methods
Search strategy
This meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses incorporating network meta-analysis (PRISMA-NMA) statement.(20) A systematic search of the literature using PubMed, EMBASE, Scopus, and the Cochrane Collaboration Library database was carried out through August 2019. The following search terms were used: (1) Romosozumab; (2) osteoporosis; and (3) RCTs. In addition, the reference lists of retrieved articles and recent reviews were reviewed. The search was limited to studies published in the English language.
Study selection
Screening of titles and abstracts was first performed. Then a second screening was based on full-text reviews. Studies were considered eligible if they met the following criteria: (1) the study design was a RCT study; (2) osteoporosis was treated with Romosozumab; (3) treatment with Romosozumab was compared with placebo or alendronate; (4) the outcome of interest and adverse effects were measured; and (5) relative risk or hazard ratio and its corresponding 95% confidence interval (CI) (or data to calculate them) were reported. Exclusion criteria were (1) conference abstracts or unpublished data; and (2) studies that did not treat humans.
Extraction data
We extracted the basic data independently from each study: article, year, number of patients, sex, mean age, dose, follow-up, intervention characteristics of the trial, and outcome measures, especially the adverse effects related to Romosozumab, alendronate, and placebo. The primary measure was the safety of the drug. To do this, we analyzed the number of adverse effects and the number of serious adverse effects. In addition, we measured specific adverse effects such as an injection site reaction, arthralgia, nasopharyngitis, and back pain. Adverse events potentially associated with injection-site reactions included any of the following events occurring at the injection site: pain, hematoma, erythema, reaction, discomfort, hemorrhage, or rash.
Assessment of study quality
The quality of RCTs was evaluated in accordance with Review Manager (RevMan) version 5.3 (The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, 2014) software to assess for the risk of bias. If there was a conflict between the two reviewers, a third reviewer was consulted to arrive at a decision. The evaluation methods consisted of the following steps: random sequence generation, allocation concealment, blinding, incomplete outcome data, and selective outcome reporting.
Statistical analysis
The meta-analysis was carried out using the review manager 5.3 of the Cochrane community. The odds ratio (OR) with a 95% CI was calculated as dichotomous results. The Mantel–Haenszel (M-H) method and fixed effects were used depending on whether or not there was significant statistical heterogeneity in the results. Heterogeneity was tested with a chi-square test and the I2 method. I2 varies from 0% to 100%: 30%–40% indicates insignificant heterogeneity, 30%–60% moderate heterogeneity, 50%–90% substantial heterogeneity, and 75%–100% high heterogeneity. The inverse variance method and fixed effects were used according to whether or not there was significant statistical heterogeneity in the results. p Values <0.05 were considered significant.
Results
Literature search
The results of the selection process are presented in Figure 1. In this study, only adverse effects are included in the comparison. A published meta-analysis in 2017(13) was found which focused on BMD and the incidence of fractures. A total of 136 studies regarding Romosozumab were found, but only 9 of these studies were RCTs. Studies reporting on safety and adverse events were evaluated in light of the inclusion criterion. Five RCTs met the inclusion criteria, and these were included in the pooled analysis.(14,18,19,21,22) Among these, one trial included a comparison between Romosozumab, placebo, and alendronate, three trials reported on Romosozumab versus placebo, and one trial compared Romosozumab versus alendronate. The quality of RCTs is presented in Figure 2.
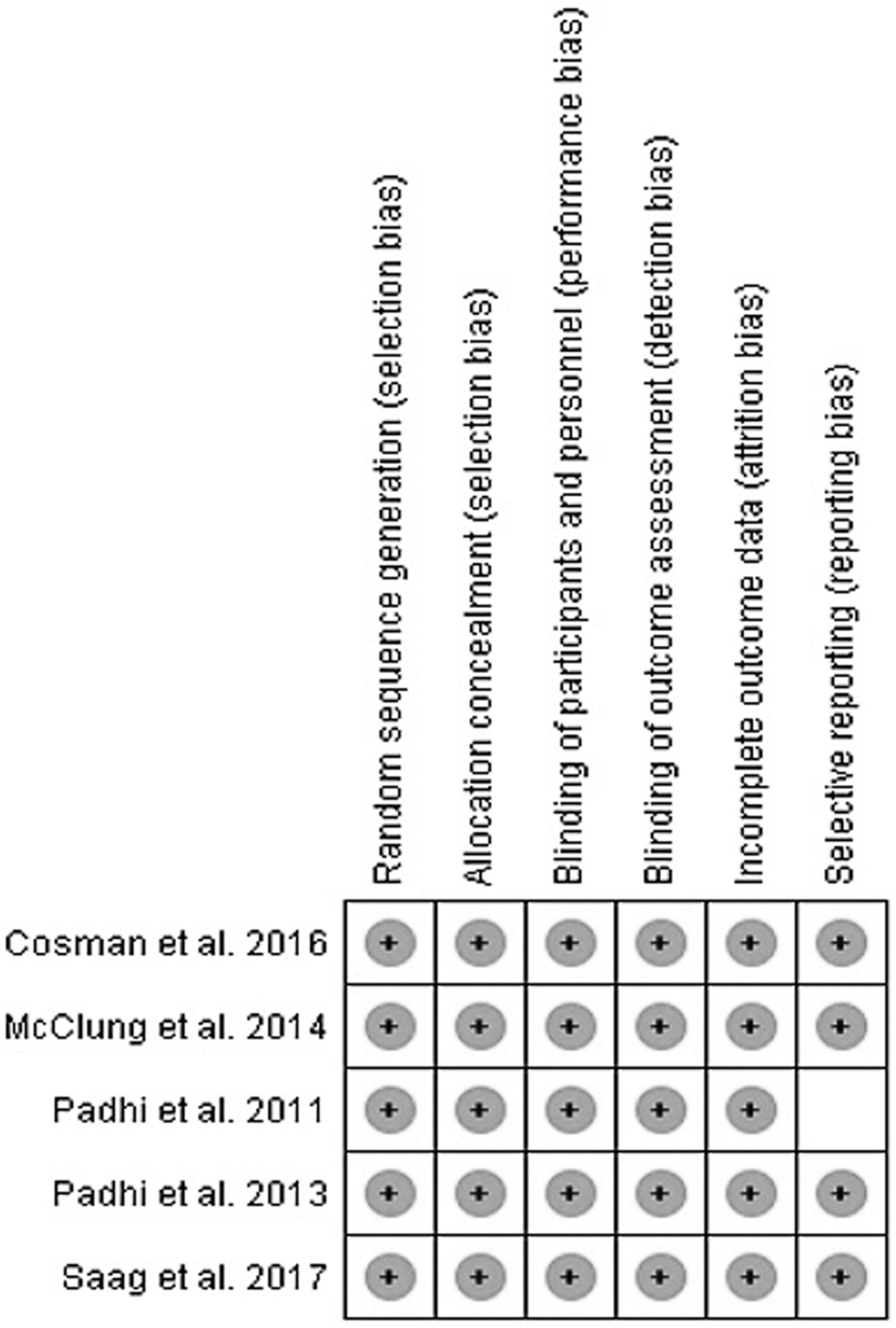
Risk of bias summary (+: low risk; white: unknown).

Study selection flow diagram (Preferred Reporting Items for Systematic Reviews and Meta-Analysis).
Baseline data
The main characteristics of the five selected studies are summarized in Table 1. The studies were published from 2011 to 2017.(14,18,19,21,22) A total of 11,741 patients were included in the study. Five thousand nine hundred seventy-four received Romosozumab, 2098 alendronate, and 3669 placebos. Three groups were assessed: the experimental group, which included patients treated with Romosozumab, and the two control groups, alendronate and placebo. Although there were two control groups, each was compared separately with Romosozumab.
Characteristics of the Randomized Controlled Trial Studies Included in the Meta-Analysis
A, alendronate; D, doses; P, placebo; R, romosozumab; RCT, randomized controlled trial; SC, subcutaneous; SD, standard deviation.
The basic characteristics of the patients were collected in the three groups. Regarding sex, the majority was postmenopausal women (90.6%), and men made up the remainder (9.4%). The mean age of the patients in the three groups, Romosozumab, alendronate, and placebo, was 64.6, 70.6, and 62.4 years, respectively. The average duration of the studies was 8.33 months. Safety was studied with respect to all the administered doses given subcutaneously.
Placebo group
In the placebo group four studies which had the relevant data were included. A total of 7566 patients were assessed. The total number of adverse events was marginally higher in patients who received placebo (2914/3652, 79.8%) than in patients receiving Romosozumab (3085/3914, 78.8%), but this difference was not significant (M-H 0.92, 95% CI 0.82–1.03, p = 0.15) (Fig. 3a). Looking at reports of serious adverse events, 7518 patients were assessed. The placebo group had fewer serious adverse events (319/3640, 8.7%) than Romosozumab (362/3878, 9.3%), but again no statistically significant difference was seen (M-H 1.09, 95% CI 0.93–1.27, p = 0.30) (Fig. 3b).

Forest plot of risk difference in placebo versus Romosozumab in the randomized controlled trial studies included.
A comparison of reactions at the injection site included 6840 patients. In this case, statistically significant differences were found, with a higher number of injection site reactions in patients treated with Romosozumab (230/3914, 5.8%) compared to the placebo group (106/2926, 3.6%) (M-H 1.54, 95% CI 1.22–1.96; p < 0.001) (Fig. 4a).

Forest plot of risk difference in placebo versus Romosozumab in the randomized controlled trial studies included. Specific adverse events.
Arthralgia was measured in 7261 patients and was lower in the placebo group (432/3602, 11.9%) compared to Romosozumab (475/3659, 12.9%) without significant difference (M-H 1.10, 95% CI 0.95–1.26, p = 0.19) (Fig. 4b).
Nasopharyngitis was analyzed in 7025 patients. There was no significant difference in the Romosozumab group (467/3617, 12.9%) compared to the placebo (439/3588, 12.2%), (M-H 1.06, 95% CI 0.92–1.22, p = 0.42) (Fig. 4c).
Similarly, low back pain, which was reported as a measure in 7261 patients, did not show significant difference in the Romosozumab group (382/3659, 10.4%) compared to the placebo group (381/3062, 10.6%) (M-H 0.99, 95% CI 0.85–1.15, p = 0.86) (Fig. 4d).
Alendronate group
In the alendronate group, 4360 patients were included in the reporting of adverse events. Significant differences were seen with more adverse events reported in patients treated with alendronate (1628/2065, 78.8%) with respect to Romosozumab (1765/2295, 76.9%) (M-H 0.85, 95% CI 0.74–0.98, p < 0.05) (Fig. 5a) although this difference, though statistically significant, may not be clinically relevant.

Forest plot of risk difference in Alendronate versus Romosozumab in the randomized controlled trial studies included.
Serious adverse event group included 4360 patients. In the alendronate group, more serious adverse events (282/2065, 13.6%) were described in comparison with Romosozumab (279/2295, 12.2%). However, this was not found to be statistically significant (M-H 0.92, 95% CI 0.77–1.10, p = 0.35) (Fig. 5b).
Injection site reaction was assessed in 4360 patients. Injection site reactions were higher with Romosozumab (121/2295, 5.27%) compared to the alendronate group (54/2065, 2.62%), and the difference was significant (M-H 1.85, 95% CI 1.32–2.60, p = 0.0003) (Fig. 5c).
Discussion
Several clinical trials and a meta-analysis have indicated that Romosozumab treatment is associated with increased BMD.(13–19) However, the safety of this new drug is not well documented.(13) In our meta-analysis, we found that Romosozumab has adverse effects comparable to placebo and that it does not significantly produce nasopharyngitis, arthralgia, and back pain with respect to the control groups. However, Romosozumab does have a higher incidence of reactions at the injection site.
Sclerostin is an inhibitor of osteoblast-mediated bone formation secreted by osteocytes to regulate and control bone turnover. Romosozumab is a monoclonal antibody that binds to sclerostin.(23) Several sclerostin antibodies have been clinically evaluated; however, the use of Romosozumab is the most frequent.(5) Romosozumab treatment has been demonstrated to improve bone mass and strength while maintaining the bone quality.(24) However, to our knowledge, only one meta-analysis has evaluated the Romosozumab treatment.(13) That meta-analysis focused on the improvement in BMD and the incidence of fractures during the treatment. In our meta-analyses, we focus on the safety of this new drug. A total of nine RCTs that compared Romosozumab treatment with placebo or alendronate were found,(14–19,21–23) but only five studies included the adverse events.(14,18,19,21,22) It was not possible to compare romosozumab with teriparatide because among the studies found only one included adverse events.(18) It is important to emphasize that the largest number of patients included the FRAME and ARCH studies, with >95% of the weight.
The total number of adverse events was higher in patients who received alendronate or placebo than in patients receiving Romosozumab, but this difference was not significant. However, if we observe only serious adverse events, the placebo group had fewer serious adverse events than Romosozumab, meanwhile alendronate group had more serious adverse events than Romosozumab, but these differences were not statistically significant. McClung et al. found that the proportions of participants reporting adverse events and serious adverse events were similar in the pooled placebo group and the Romosozumab groups. No serious adverse event was reported by more than one participant in any group, and none of the serious adverse events was considered by the investigator to be treatment related.(18)
Also in other studies the incidences of adverse events and serious adverse events were similar overall between the Romosozumab and placebo or alendronate treatment groups during the 12-month assessment.(14,19) In the other two studies, only two subjects had serious adverse events, neither of which was considered to be related to the treatment by the authors; however, the follow-up period was only 12 weeks.(21,22) In all studies the principal serious adverse effects were the cardiovascular events.(14,18,19,21,22) The Saag et al. study reported that 50 patients (2.5%) in the Romosozumab group and 38 (1.9%) in the alendronate group had serious cardiovascular adverse events (OR 1.31; 95% CI 0.85–2.00).(19) Cosman et al., found a 1.2% (44 patients) incidence of serious cardiovascular adverse events in Romosozumab group and 1.1% (41 patients) in the placebo group.(14) In all these studies the eligible subjects were osteoporotic men and postmenopausal women, between 45 and 80 years of age, with low BMD or total hip.(14,18,19,21,22) No cardiovascular evaluation of these patients was required before enrollment in their respective studies. In this meta-analysis, cardiovascular adverse events could not be compared independently. Only two studies specifically reported cardiovascular adverse events.(14,19) These could not be pooled since one compared Romosozumab with alendronate and the other with placebo. We realize that despite the potential efficacy of Romosozumab, the Food and Drug Administration (FDA) has not yet approved Romosozumab for the treatment of osteoporosis. This is apparently because of an unexpected increase in cardiovascular events.(25) With the available data and this meta-analysis, we can only state that the risk of major adverse events is similar with Romosozumab and alendronate.
According to the present meta-analysis, compared to the placebo group, the only significant differences were found in the injection site reactions. We think if the Romosozumab is capable of generating a local reaction, the severity of this reaction should be assessed. McClung et al., and Cosman et al., described that most reactions were moderate, although some were also severe.(14,18) Saag et al. reported that in the first 12 months, injection site reactions (mostly mild in severity) were reported in more patients receiving Romosozumab (90 of 2040 patients [4.4%]) than in those receiving alendronate (53 of 2014 patients [2.6%]).(19) Cosman et al., found injection site reactions, which were mostly mild in severity, in 187 patients (5.2%) in the Romosozumab group and in 104 (2.9%) in the placebo group. Moreover, they reported that serious adverse events that were indicative of hypersensitivity occurred in seven patients in the Romosozumab group in the first year of treatment.(14) McClung et al., also reported injection site reactions; however, they also stated that no patient had to leave the study due to injection site reactions.(18)
Romosozumab injection site reactions should be further characterized. Some have postulated that the dose could be a factor influencing this local process.(11,26,27) The dose administered in most studies that included Romosozumab and injection site reactions was 210 mg.(18,19) Trials have shown the greatest efficacy with this dose; however, efficacy was also present with other lower doses.(21) Moreover, in the study of Padhi et al., with lower doses of Romosozumab (2 mg/kg), a lower incidence of injection site reactions was reported compared to other studies.(21) It was also observed that there were more injection site reactions with the highest doses (5 or 10 mg/kg).(22) Using the smallest effective dose may reduce injection site reactions.
Our study has a few limitations. First, not all the RCTs selected measured the same adverse events so only those that coincided could be compared. Moreover, we had to exclude from the final analysis four RCTs because they did not measure adverse effects. Second, the studies were heterogenous; patients differed in terms of age, although they were considered older patients in all the studies. Third, there is heterogeneity in the times of follow-up. Most studies obtained a follow-up of 12 months; however, some studies included had smaller follow-up. Even though our meta-analysis is useful, we think that better evaluation of the safety of Romosozumab needs larger RCTs with longer duration of follow-up, particularly with respect to cardiovascular events.
In conclusion, the results of our meta-analysis suggest that Romosozumab has somewhat fewer adverse effects overall than alendronate and comparable to a placebo, except injection site reactions. Injection site reactions were also more frequent in comparison to alendronate.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.