
Abstract
Different signaling pathways have been studied in ankylosing spondylitis. New treatment options such as secukinumab could have an important role inhibiting the release of proinflammatory cytokine IL-17. The aim of this study was to compare the efficacy and safety of secukinumab in ankylosing spondylitis. A systematic review was conducted using MEDLINE and EMBASE databases to identify randomized clinical trials (RCTs) that assess the role of secukinumab in ankylosing spondylitis. The variables were safety (total adverse events, serious adverse events, headache, nasopharyngitis, cough, deaths, discontinuation due to adverse events, candida, neutropenia, and diarrhea) and efficacy based on quality-of-life scores (ASAS 20, ASAS 40, ASAS 5/6, ASASPR). Three RCTs (770 patients) that compare secukinumab with placebo were included in the study. There were significant differences in the quality-of-life scores in favor of the secukinumab group (p < 0.05). Regarding the adverse events, there were higher rates of any adverse events in the secukinumab group (p < 0.05). Also, the secukinumab group showed a higher rate of nasopharyngitis and diarrhea (p < 0.05). The use of secukinumab in ankylosing spondylitis increased the quality of life and had more adverse events rate compared with placebo.
Introduction
Ankylosing spondylitis is a chronic autoinflammatory disease affecting the spine, SI joints, and occasionally the peripheral joints.(1,2) While enthesitis and axial spondylitis are the hallmarks of this disease, clinicians must be mindful of extra-articular and skeletal manifestations, which may be cardiac, pulmonary, neurological, renal, dermatological, or ocular.(3) It is reported in the literature that up to 30% of AS patients will develop ischemic heart disease. If left untreated, patients end up with severe loss of posture and mobility.(4) The relatively common and widespread impact of AS on practically all organ systems highlights the necessity for effective disease control.(5–7)
Although there is no cure for ankylosing spondylitis, many treatments have emerged in the management of AS in controlling inflammatory symptoms. There is a general consensus that all patients are to receive physical therapy in conjunction with being placed on chronic NSAID therapy, with the latter aimed at decreasing radiographic progression of the disease.(8) For patients with persistent active disease despite NSAID therapy, a biologic DMARD is the next logical step. Prior first choice and best-studied therapy includes anti-TNF drugs. These drugs have greatly benefited patients with AS in the new decade. Regrettably, many patients cannot tolerate or eventually develop resistance to anti-TNF therapy.(9)
In this review, we examine the side effect profile and efficacy of secukinumab, a human IgG1k monoclonal antibody IL-17 alpha blocking biologic DMARD with similar reported disease management to anti-TNF agents.(10)
Materials and Methods
Search strategy and study selection
This meta-analysis was conducted according to the PRISMA statement.(11) A systematic search of the literature using PubMed was carried out through July 2018. The following search terms were used: (1) ankylosing spondylitis; (2) secukinumab; (3) randomized clinical trials (RCTs). In addition, the reference lists of retrieved articles and recent reviews were reviewed. The search was limited to studies published in the English language.
Studies were considered eligible if they met the following criteria: (1) the study design was an RCT study; and (2) the outcome of interest was safety and efficacy based on different quality-of-life scores. Exclusion criteria were studies that did not treat humans, studies that were the same, and studies that did not share variables.
Data extraction
We extracted the basic data independent of each study: article, year, number of patients, sex, age, dose, and follow-up. The variables for comparison were limited to quantitative variables. These variables were related to the efficacy and safety of the use of secukinumab in ankylosing spondylitis. These were dichotomous. First, a comprehensive reading of the articles was done taking into account the comparisons presented by each one. With this method, two aspects could be compared: safety (total adverse events, serious adverse events, headache, nasopharyngitis, cough, deaths, discontinuation due to adverse events, candida, neutropenia, and diarrhea) and efficacy based on quality-of-life scores (ASAS 20, ASAS 40, ASAS 5/6, ASASPR). The safety analysis was performed with all the doses that were offered in the study during the follow-up. The evaluation of the efficacy was performed by the 150 mg arm and during a follow-up of 6 or 16 weeks. The primary efficacy endpoint was the percentage of patients with a 20% response according to the Assessment of SpondyloArthritis international Society criteria for improvement (ASAS20) at week 6. Twenty-one secondary efficacy endpoints included ASAS40 (40% response according to ASAS criteria for improvement) and ASAS5/6 responses (improvement in five of six domains: pain, patient global assessment, function, inflammation, spinal mobility, C-reactive protein [acute-phase reactant] without deterioration in the 6th domain). ASAS partial remission was a score of ≤2 units in each of the four core ASAS domains.
Study quality assessment
The quality of RCTs was evaluated in accordance with Review Manager (RevMan) version 5.3 (The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, 2014) software to assess the risk of bias (Fig. 1). If there was a conflict between the two reviewers, a third reviewer is consulted and a discussion is conducted to arrive at a decision. The evaluation method consisted of the following steps: random sequence generation, allocation concealment, blinding, incomplete outcome data, and selective outcome reporting

Risk of bias summary (+ = low risk, white = unknown).
Statistical analysis
The meta-analysis was performed using the Review Manager 5.3 software provided by the Cochrane community. The odds ratio (OR) with a 95% confidence interval (CI) was calculated for the dichotomous variables, and the difference in means (DM) and the 95% CI were calculated for the continuous variables. Heterogeneity was evaluated using the chi-square test and the I2 method. The I2 statistic describes the percentage of variation across studies that is due to heterogeneity rather than chance. When heterogeneity is substantial, a prediction interval rather than a confidence interval can help have a better sense of the uncertainty around the effect estimate. I2 varies from 0% to 100%: 30%–40% indicates insignificant heterogeneity, 30%–60% moderate heterogeneity, 50%–90% substantial heterogeneity, and 75%–100% high heterogeneity. The inverse variance method and the fixed effects were used according to whether or not there was significant statistical heterogeneity in the results. p-Values <0.05 were considered significant.
Results
Literature search
The results of the selection process are presented in Figure 2. The decision to conduct a meta-analysis was based on the following. First, 11 studies were found with the first screening. One of them used secukinumab for rheumatoid arthritis. Eight articles were the same and we chose the article that included the required variables to compare with the other two studies. This article included MEASURE 1 and MEASURE 2 information. Second, there is no meta-analysis related to this topic. The meta-analysis consisted in three RCTs. With regard to the included patients, the sample was homogeneous, with a similar average age in the three RCTs and a follow-up time of 16 weeks. We chose the arm that treated with 150 mg of secukinumab.
Study selection flow diagram (preferred reporting items for systematic reviews and meta-analysis).
Baseline data
The main characteristics of the three selected studies are summarized in Table 1. The studies were published from 2013 to 2017. There were a total of 770 patients, 492 received secukinumab and 278 received placebo, of whom 371 and 399 were men and women, respectively. The RCTs were performed in people aged 40– 45 years. The dose arm selected was 150 mg. Furthermore, the average duration was 16 weeks.
Characteristics of Included Randomized Control Trials
S, Secukinumab group; P, placebo group.
Efficacy
The ASAS20 criteria were achieved by 58.2% in the secukinumab group versus 30.1% in the control group (OR 3.35, 95% CI: 2.36–4.75, p < 0.00001, I2 = 0%). A total of 43.2% of the secukinumab group met the criteria of ASAS 5/6 improvement versus 11.9% in the control group (OR 5.91, 95% CI: 3.84–9.12, p < 0.00001, I2 = 0%). The ASAS 40 was achieved by 37.8% in the secukinumab versus 14.7% in the control group (OR 3.69, 95% CI: 2.45–2.56, p < 0.00001, I2 = 13%). Finally, the ASAS PR was achieved by 9.6% in the secukinumab versus 2.9% in the control group (OR 3.52, 95% CI: 1.56–7.92, p < 0.002, I2 = 0%) (Fig. 3).
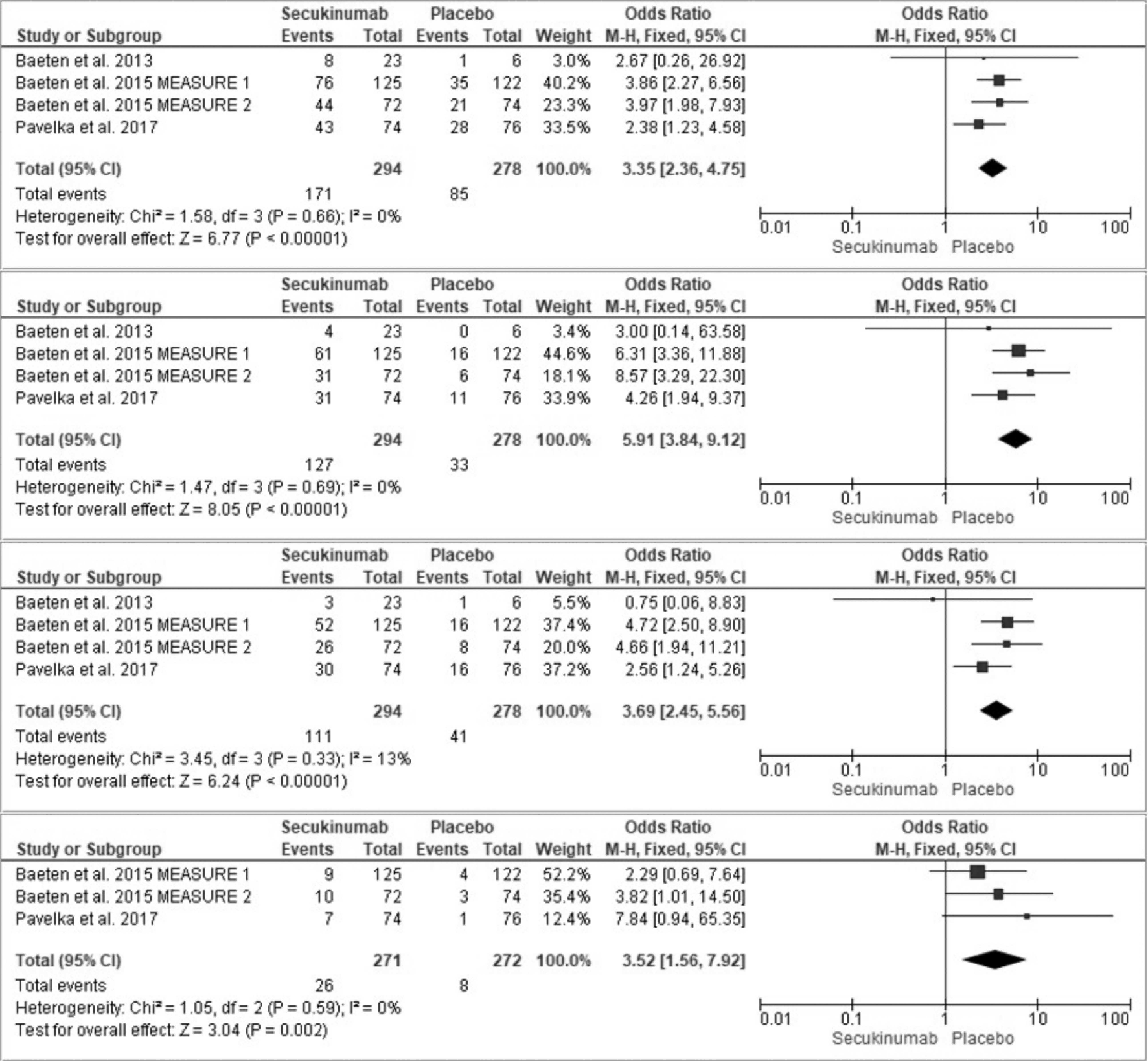
Forest plot of risk difference in quality-of-life scores.
Safety
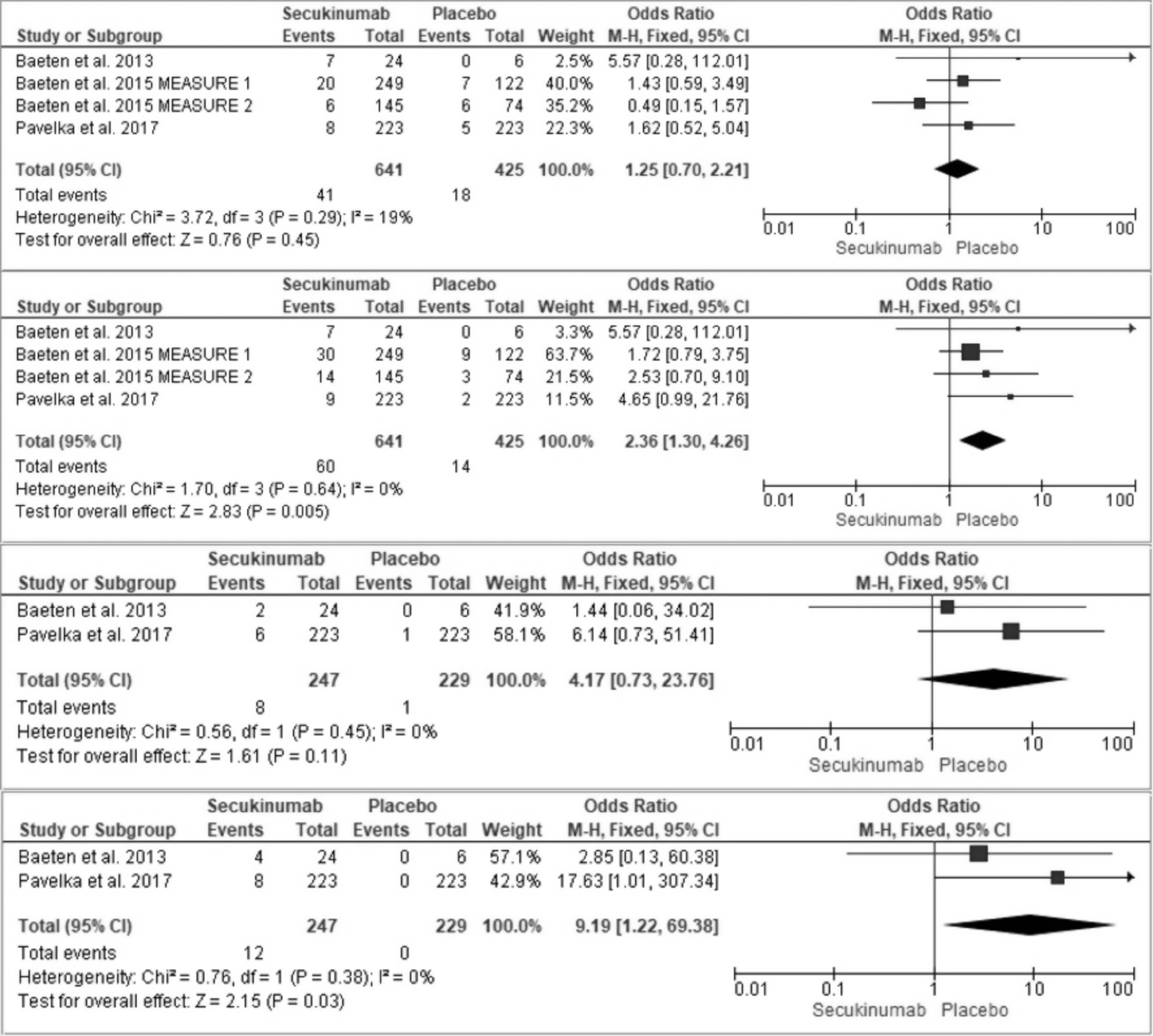
The summary of all the adverse effects compared in the study is shown in Figure 4. The total of any adverse event was lower in the control group (OR 1.70, 95% CI: 1.29–2.24, p = 0.0002, I2 = 58%). These differences were not significant for any of the specific adverse events except for nasopharyngitis (OR 2.36, 95% CI: 1.30–4.26, p = 0.005, I2 = 0%) and diarrhea (OR 9.19, 95% CI: 1.22–69.38, p = 0.03, I2 = 0%) in favor of the control group (Figs. 5 and 6).

Risk difference in adverse events rates from randomized control trial studies included the following: any adverse event; serious adverse events; discontinuation due to adverse events; and deaths.
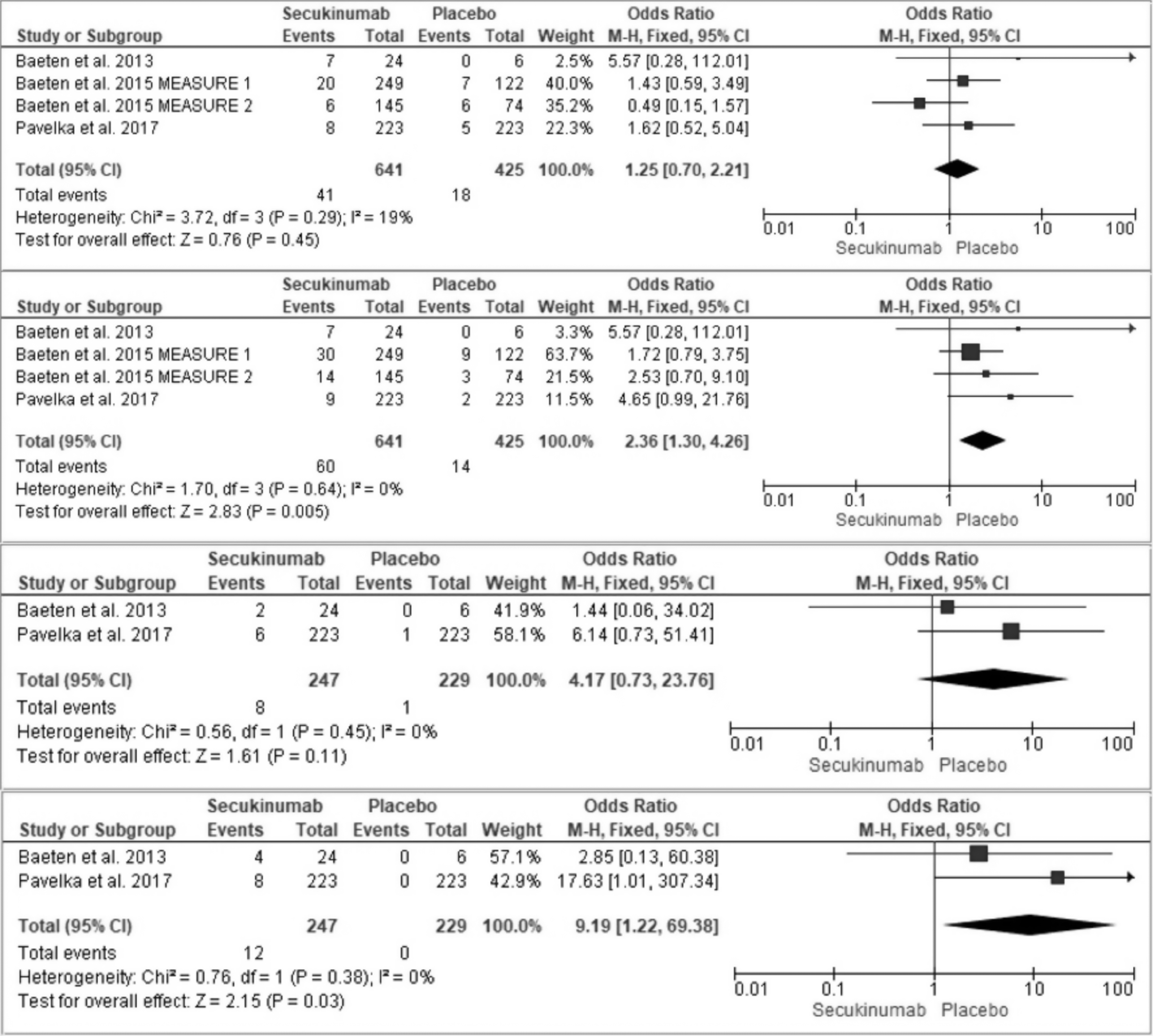
Risk difference in adverse events rates from randomized control trial studies included the following: headache; nasopharyngitis; cough; and diarrhea.
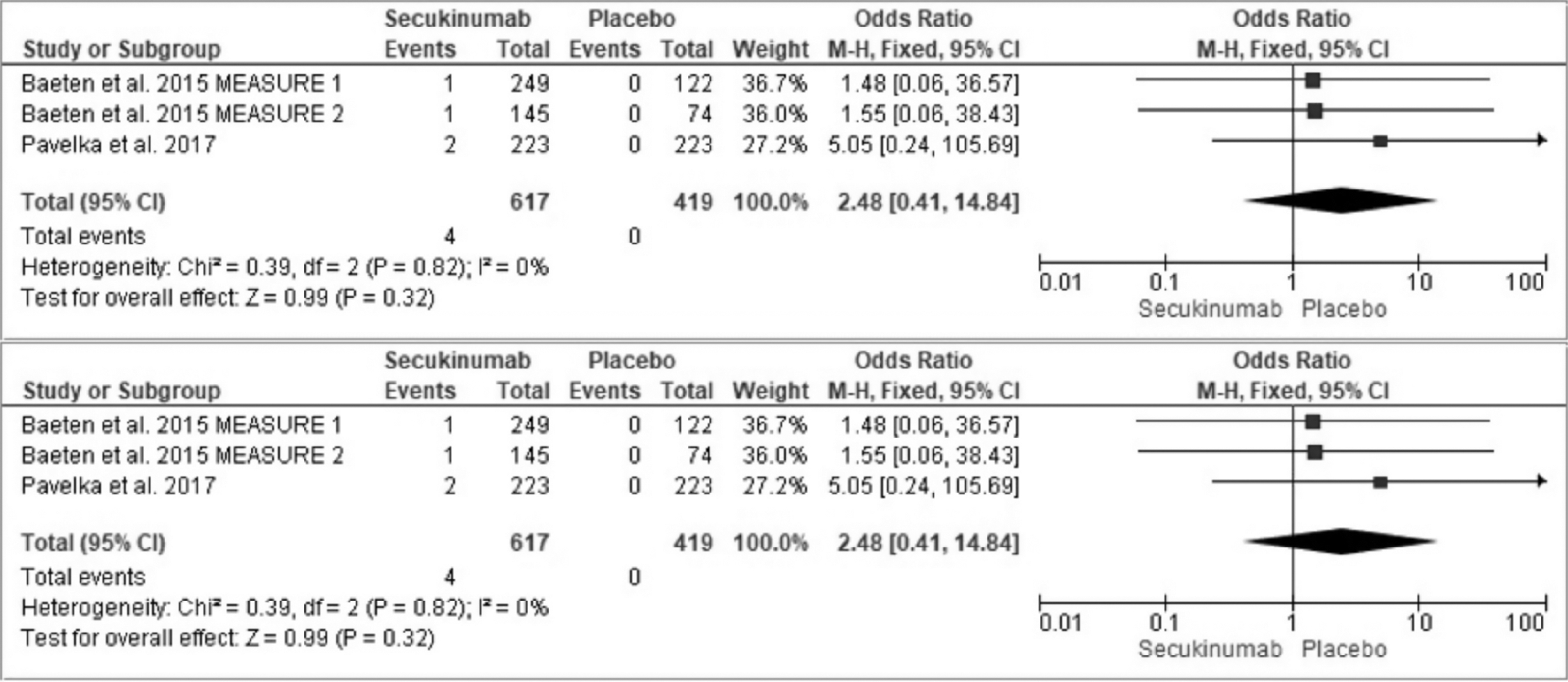
Risk difference in adverse events rates from randomized control trial studies included candida and neutropenia.
Discussion
In our review, secukinumab demonstrated superiority to placebo with regard to efficacy. Secukinumab met the primary (ASAS 20) and secondary (ASAS 5/6, ASAS 40, ASAS partial remission) endpoints in terms of statistically significant disease activity score increases, with up to 58.2% of patients in the secukinumab group reaching ASAS 20 criteria and 9.6% reaching ASAS PR (both higher than placebo). These data also showed that 43.2% of patients met the criteria of ASAS 5/6 improvement and 37.8% reached ASAS 40 illustrating secukinumab's long-term benefits. Patients taking the 150 mg dose achieved meaningful improvements by an average of 16 weeks demonstrating its rapid reduction of clinical or biological signs. These results were sustained through 52 weeks of treatment.
The side effect profile with anti-TNF is fairly extensive, including serious bacterial and opportunistic infections, increased risk of melanomas and other skin cancers, development of demyelinating syndromes, congestive heart failure, and hematologic abnormalities (neutropenia, thrombocytopenia, and pancytopenia) to name a few. This makes it a challenge to initiate anti-TNF in patients with various comorbidities. Secukinumab was generally well tolerated at all doses. Our review showed an expected total increase of adverse events in patients using secukinumab compared with placebo, as seen in other studies.(15) Other studies reported no significant differences regarding the adverse events rate.(16,17)
Nasopharyngitis and diarrhea were the only statistically significant side effects. Most important to note was that there was no statistically significant evidence of an increase in serious adverse events.
The data above show there is high-quality evidence that secukinumab improves clinical symptoms and that the IL-17 alpha pathway plays a significant role in the pathogenesis of ankylosing spondylitis. Secukinumab is a very effective medication in the management of AS, which can be safely used if side effects are acknowledged. Compared with its anti-TNF counterpart, the side effect profile (nasopharyngitis, diarrhea) of secukinumab is less extensive and severe making it the more advantageous option in patients with significant comorbidities or contraindications. In one study, patients who were naive to anti-TNF therapy with secukinumab started as their first biologic treatment, ASAS20 response rates were ∼5% higher with secukinumab than with the general population.(14)
This information is promising not only for starting secukinumab after anti-TNF failure but also potentially as the first choice treatment in AS patients. Blocking the IL-17 alpha pathway offers clinicians a viable alternative to the classically used anti-TNF agents, with similar routine monitoring for other biologic therapies.
Footnotes
Author Disclosure Statement
The authors declare no conflict of interest, financial or otherwise.
Funding Information
No funding was received for this article.