
Abstract
The epidemiology of patients associated with ampicillin-resistant Enterococcus faecium (ARE) was investigated by combining both clinical approach and molecular analysis in a kidney transplant patient's ward. A case–control study was performed to identify risk factors for ARE by matching each patient with ARE with two control patients without any isolated E. faecium strain. ARE isolates were characterized by pulsed-field gel electrophoresis. From June 2004 to May 2006, 18 cases with clinical ARE samples were detected and compared with 35 control patients. By univariate analysis, recurrent urinary tract infections (UTIs) (odds ratio [OR], 4.9; 95% confidence interval [CI], 1.0–25.6), mean number of hospitalization days in the last year (p < 0.003), pyelonephritis or UTI (OR, 9.6; 95% CI, 2.2–46.1), oral third-generation cephalosporin use (OR, 12.42; 95% CI, 2.04–109.1), and fluoroquinolone use (OR, 4.4; 95% CI, 1.1–18.2) were significantly associated with ARE urinary tract colonization. By conditional logistic regression, hospitalization >21 days within 1 year (adjusted OR [aOR], 6.9; 95% CI, 1.0–46.5), recent medical history of pyelonephritis or UTI (aOR, 8.6; 95% CI, 1.5–49.1), and prior oral third-generation cephalosporin use (aOR, 13.1; 95% CI, 1.2–142.6) were identified as independent factors associated with ARE urinary tract colonization. Genotyping revealed a heterogeneous epidemiological situation with two major clones in patients hospitalized in successive rooms and 10 different single pulsotypes. Emergence of highly resistant enterococcal strains is a collateral damage from antibiotic prescription and represents a potential source of patient-to-patient transmission. Combining epidemiological approach and molecular analysis is a powerful tool to delineate mechanisms of emerging resistance. Improving our knowledge on ARE emergence in high antibiotic pressure hospital wards is a key factor to better control these colonizations/infections and to prevent the emergence of vancomycin-resistant E. faecium.
Introduction
Materials and Methods
Setting and background
The Nantes center is a tertiary-care university hospital with 3,000 beds. The Immunology-Nephrology-Transplant (INT) Department is a 30-bed service (9 rooms with 2 beds and 21 single rooms). One hundred kidney and 30 pancreatic transplantations are performed each year. Three ARE isolates were detected by the laboratory between June and October 2004 in patients hospitalized in the INT Department. The Infection Control Team was alerted to investigate this new epidemiological situation.
Study design
Consecutive positive clinical specimens for all patients admitted to the INT Department were prospectively examined between June 2004 and May 2006 to identify cases of ARE colonization or infection in pancreatic and/or kidney transplant patients. ARE clinical isolates were characterized by pulsed-field gel electrophoresis (PFGE). Patients with enterococcal positive cultures were compared with controls with enterococcal negative cultures to identify risk factors for colonization or infection with ARE.
Microbiological methods
Urine samples were cultured on urinary tract infection (UTI) agar (Oxoid, Dardilly, France). Initial identification was based on colony morphology, catalase-negative test, and agglutination test with the Streptococcal Grouping Kit® test (Oxoid). The Vitek2® system (bioMérieux, Marcy-l'Etoile, France) was used for identification (ID-GP) and antimicrobial susceptibility testing (AST-P563 card) of the E. faecium isolates. UTI was defined following the French definition. 15 No systematic screening for digestive carriage was performed as our objective was to identify risk factor associated with ARE colonization/infection.
Genotypes of the E. faecium strains were determined by PFGE. DNA extraction and purification were performed as follows: DNA was digested with the restriction enzyme SmaI, and the restriction fragments were separated in a CHEF-DRIII unit (Bio-Rad, Marnes-la-Coquette, France). The gel image was analyzed using Gel Compar II software (Applied Maths, Snit-Martens-Latern, Belgium). A dendrogram was made using the Dice coefficient and the unweighted pair group method with arithmetic mean analysis. PFGE profiles were interpreted using Tenover criteria. 3
Collection of clinical data
Data were recorded concerning sex, age, diabetes status, type, and date of transplant. The following additional data were extracted from the medical record: (1) within the last year before ARE isolation: recurrent UTI (>3 UTI) and hospital length of stay (total number of days); (2) within the last 3 months before ARE isolation: history of UTI, or hospitalization, dialysis, kidney tract catheterization, corticoids, and antibiotic use (ampicillin, cephalosporin, aminoglycoside, fluoroquinolone, carbapenem, cotrimoxazole, vancomycin). All included ARE were obtained from clinical specimens, as no systematic screening for ARE gastrointestinal carriage was performed during the study period. Systematic urine samples were performed at the outpatient clinic for pancreatic and/or kidney transplant patients during the postdischarge surveillance, and not only when an infection was suspected. Clinical information was collected to differentiate ARE colonization from infection. The time required for colonization or infection by ARE after antibiotic exposure was calculated.
Statistical analysis
A comparison was performed to identify risk factors for colonization/infection with ARE. Controls were selected from a kidney patient's database. Two control patients were matched with each ARE patient by the following criteria: year and month of transplantation, sex, diabetes status, and duration of follow-up at the time of matching (1 year). Controls were defined as patients without any isolated E. faecium strain and without any bacteria in systematic urine samples performed in the outpatient clinic. One case was only matched with one control. The mean number of systematic urine samples performed in the outpatient clinic was equal in both groups during the 1-year follow-up. Univariate analysis was performed, and the chi-squared test (Mantel–Haenszel) or the Fisher's two-tailed test for proportions and Student's t-test for the continuous variables were used for the significance of association. A p-value of <0.05 was considered significant. A conditional logistic regression was used to select the most informative variables to introduce in a multivariate model and to control for all the confounding factors. For model building, we applied a forward stepwise introduction of variables (p-value of <0.20). Adjusted odds ratio (OR) and 95% confidence interval (CI) were derived from the estimated regression coefficients. The fit of the model was checked using the Hosmer and Lemeshow test. Data were analyzed using the EPI INFO (Epi Info version 6.0; CDC, Atlanta, GE) and SPSS® (version 10.0; SPSS, Chicago, IL) databases.
Results
Characteristics of patients with ARE
From June 2004 to May 2006, 18 patients with urinary tract ARE isolates were identified (including the first 3 patients). The mean age was 50 ± 16 (standard deviation) years; eight patients had diabetes. Twelve patients had kidney transplant, and six had kidney/pancreas transplant. ARE was responsible for colonization in 17 patients, and for UTI with bacteremia in 1 patient. Sixteen patients had prior infection in the last 3 months: pyelonephritis or UTI (n = 12), surgical site infection (n = 2), pneumonia (n = 1), and catheter-related infection (n = 1). Most pyelonephritis or UTIs were caused by Enterobacteriaceae (67%). All 18 patients had prior antibiotic use with one or two antibiotics: fluoroquinolones (n = 11), ampicillin or co-amoxiclav (n = 8), aminoglycosides (n = 3). Fourteen patients were exposed to third-generation cephalosporins.
The mean time before ARE detection after starting antibiotic treatment was 31 ± 23 (median, 24; range, 10–108) days. No controlled urine samples performed in the outpatient clinic remained positive for ARE. The mean number of systematic urine samples was four,4,8–10,12,16 with no significant difference between cases and controls. No antibiotic was prescribed for ARE urinary tract colonization.
Matched criteria and risk factors
A case–control study was performed using matched criteria comparing 18 cases and 35 controls (Table 1). Twelve (67%) case patients and 24 (69%) control patients had kidney transplantation (p = 0.741). The other patients had kidney/pancreas transplantation. The date of transplantation between cases and controls did not differ by more than 2 months. Factors significantly associated with the emergence of ARE were recurrent UTI, total number of days at hospital within 1 year, prior UTI, digestives troubles, kidney or urinary tract catheterization, and antibiotic exposure (Table 1). The mean number of antibiotics prescribed was higher in cases than in controls (3.7 vs. 1.5, p < 0.001). Among antimicrobial agents, third-generation cephalosporin or fluoroquinolone use was significantly associated with emergence of ARE, but cotrimoxazole use was not (Table 1). In multivariate analysis, hospitalization within 1 year (OR, 6.91; 95% CI, 1.03–46.53), recent medical history of UTI (OR, 8.7; 95% CI, 1.53–49.14), and prior oral third-generation cephalosporin use (OR, 13.2; 95% CI, 1.21–142.6) were identified as independent factors associated with ARE urinary tract colonization/infection (Table 2).
OR, odds ratio; 95% CI, 95% confidence interval; UTI, urinary tract infection; NC, not calculable.
aOR, adjusted odds ratio.
Microbiological analysis and distribution of the different pulsotypes
Two major clones (A and B) and 10 single PFGE pulsotypes (C to L) were detected by molecular analysis using the Tenover criteria (Fig. 1). The pulsotype A (six patients) included strains resistant to ampicillin, imipenem, and fluoroquinolone and with a high-level aminoglycoside resistance. It remained susceptible to glycopeptides, linezolid, and quinupristine/dalfopristine. Pulsotype A was detected during the first year of the study period. The six patients were hospitalized in the same part of the ward in three adjacent rooms: room 41 (patients 1 and 4), room 42 (patients 2 and 3), and room 43 (patients 5 and 6). Patients 3, 4, and 5 were hospitalized during the same period. There was a 5-month period between patients 5 and 6 hospitalizations.

Pulsed-field gel electrophoresis banding patterns after SmaI digestion of 18 ampicillin-resistant Enterococcus faecium isolates. Percentages of similarity are shown on the left of the dendrogram. The different pulsotypes are named by a letter on the right of the dendrogram.
Pulsotype B included two closely related isolates, detected from two patients in May 2005. Those two patients were successive patients in a same room (room 60). The different PFGE pulsotypes and their temporal distribution are shown in Fig. 2.
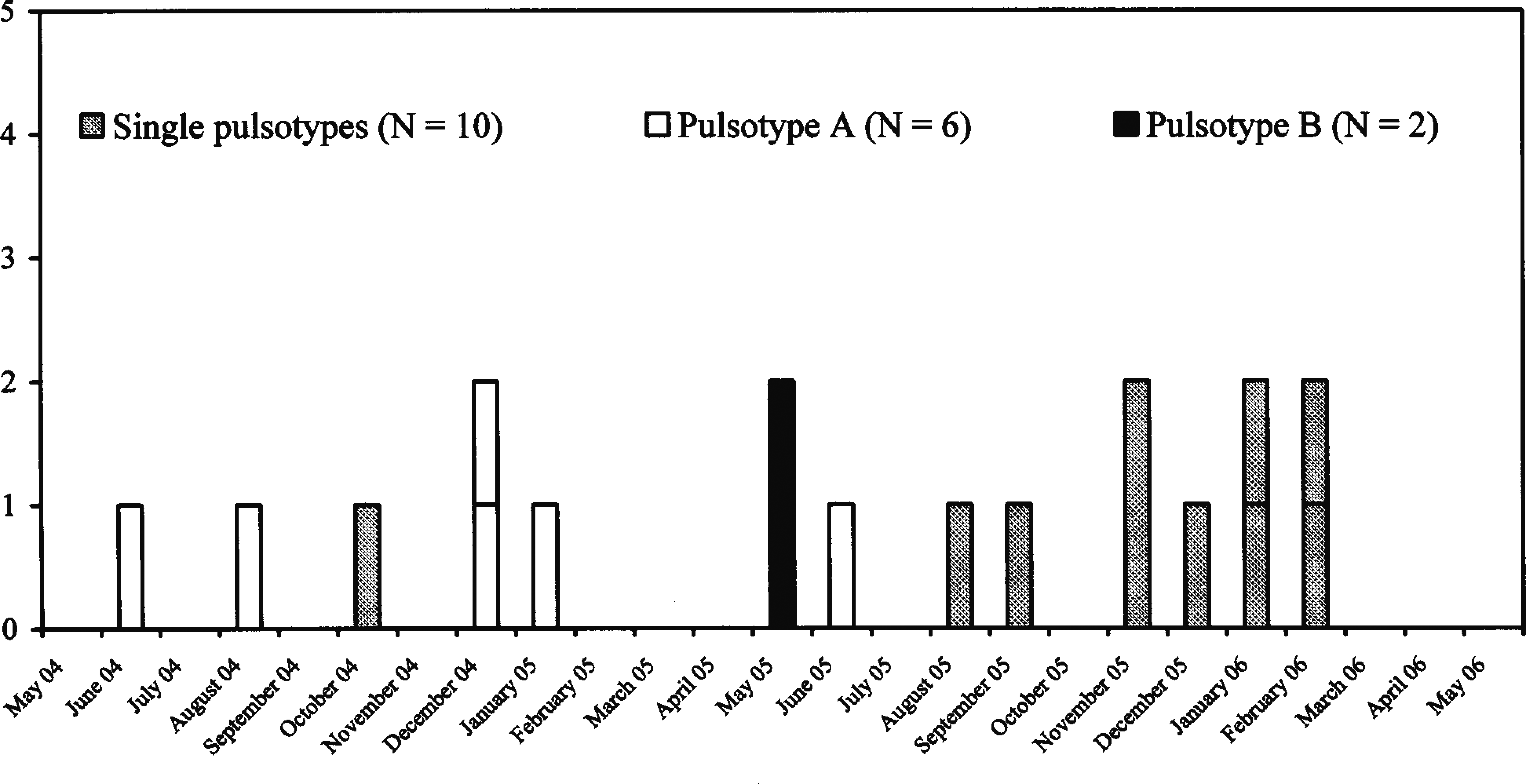
Distribution of epidemic and nonepidemic pulsotypes of high ampicillin resistance Enterococcus faecium in a kidney transplant ward.
Discussion
In this study, we reported the emergence of ARE in the kidney transplantation ward of Nantes University Hospital from June 2004 to May 2006. What makes this study of value is that this type of bacteria is somewhat neglected and most papers focus on vancomycin-resistant enterococci. It is important to understand the spread of ARE strains to implement strategies for prevention in such a low incidence setting. ARE were frequently isolated from routine urinary samples in the outpatient clinic, few weeks after hospitalization for pyelonephritis or UTI. No systematic screening for digestive carriage was done because we focused on the risk factors for urinary tract infection (UTI) colonization and/or infections.
When compared with control patients with enterococcal negative culture, case patients were more likely to be colonized with ARE after exposure to oral third-generation cephalosporin. Few case–control studies of risk factors for ARE infection have been previously published. Venditti et al. compared 17 ARE-infected patients with 64 patients infected with ampicillin-susceptible enterococcal strains: hospitalization in a surgical service, prolonged hospital stay, and prior treatment with antimicrobial agents were considered as significant risk factors for ARE infection. 18 Nevertheless, they did not perform a multivariate analysis to identify potential confounding factors. More recently, Sexton et al. performed a logistic regression analysis of 44 patients colonized or infected with ARE, compared with 100 control patients with ampicillin-susceptible enterococcal strains. 14 After adjusting for age and site of infection, they found that patients with ARE were more likely admitted to the same hospital and treated by third-generation cephalosporins or clindamycin. However, only advanced age and clindamycin use were independently associated with ARE.
In a Norwegian study, Harthug et al. compared 123 ARE-infected patients with 123 control patients without enterococcal infection. 9 A logistic regression analysis showed that cephalosporin use was significantly associated with ARE infection (OR, 4.7), without differences between first-, second-, or third-generation cephalosporins.
The results of this study showed also an association between fluoroquinolone use and ARE by univariate analysis, but this association was not confirmed by multivariate analysis. The small sample of our study can explain this finding and our results need to be confirmed in a larger cohort population.
The choice of the most appropriate control group is critical in case–control studies assessing the impact of antibiotic use. 7 In our study, we analyzed the potential risk factors for ARE emergence in kidney transplant patients, by comparing patients with positive culture for ARE with control patients without any isolated enterococcal strain. Further, the duration of follow-up of 1 year was a matching criterion to adjust risk factors on duration of exposure. It was not possible to use the length of stay as a matching criterion, as the number of possible matching controls was very low.
The impact of cephalosporin use has also been demonstrated in the emergence of VRE, particularly in ICU patients.5,6,11 The relation between the ARE diffusion and the emergence of VRE is complex and difficult to elucidate. The emergence of vancomycin resistance by ARE seems to be also associated with increased use of vancomycin. 8 However, the use of third-generation cephalosporins and vancomycin may favor the emergence of VRE during an ARE outbreak. 6 In our study, most of the ARE strains were also resistant to imipenem and fluoroquinolone, but remained susceptible to vancomycin. Stress-inducing conditions in hospital, such as antimicrobial drug use, may have favored the selection of an enterococcal subpopulation, with enhanced antibacterial resistance and ability to spread.13,19
The PFGE analysis showed that epidemic spread is possible, leading to a patient-to-patient transmission. Two of PFGE pulsotypes concerning eight patients were observed during the first part of the study. Six patients were probably colonized by cross transmission during their hospitalization (five patients with the pulsotype A and one patient with the pulsotype B). Several patients with pulsotype A were hospitalized at the same time in successive rooms and colonization pressure may have played a role in nosocomial transmission of ARE, as already demonstrated in VRE.1,2 The isolation measures implemented for ARE patients in the outpatient clinic and INT department by the infection control team can explain the decrease of clonal strains at the end of the study period. Nevertheless, molecular analysis seems to indicate that antibiotic pressure was another important factor associated with ARE emergence, as shown by the 10 patients with single phenotypes observed during the 3 years of the study period. Resistant enterococcal subpopulations selected from the endogenous flora could explain this heterogeneity. Since 2007, monthly multidisciplinary staffs including infectious disease practitioners were implemented in the INT Department to control the antibiotic exposure. Sporadic cases significantly decreased but did not completely disappear during the 2007–2009 period.
In summary, we investigated the emergence of ARE in a kidney transplant ward. This study indicates that prior cephalosporin use and patient-to-patient transmission were associated with the emergence of ARE. However, the role of each antibiotic exposure needs to be confirmed in a larger cohort population. Even if the outcome was favorable, emergence of highly resistant enterococcal strains is a collateral damage from antibiotic prescription and represents a potential source of patient-to-patient transmission, particularly in immunocompromised patients. Combining epidemiological approach and molecular analysis is a powerful tool to delineate mechanisms of emerging resistance. Improving our knowledge on ARE emergence in high antibiotic pressurehospital wards is a key factor to better control these colonizations/infections and to prevent the emergence of VRE.
Footnotes
Acknowledgments
The authors are grateful to Marie-Emmanuelle Juvin for her statistical laboratory assistance and to Cécile Giraudeau for her contribution to the molecular analysis.
Authors' Contributions
Olivier Maillard has collected, analyzed, and interpreted data, drafted the submitted article, and provided final approval of the version to be published.
Stéphane Corvec has performed and interpreted molecular analysis, revised the article critically for important intellectual content, and provided final approval of the version to be published.
Jacques Dantal has matched cases and control patients, revised the article critically for important intellectual content, and provided final approval of the version to be published.
Alain Reynaud and Pascale Bémer have analyzed microbiological data, revised the article critically for important intellectual content, and provided final approval of the version to be published.
Jean-Christophe Lucet has revised the article critically for important intellectual content and provided final approval of the version to be published.
Didier Lepelletier has made substantial contributions to conception of the study, analyzed data, revised the article critically for important intellectual content, and provided final approval of the version to be published.
Disclosure Statement
The authors declare that no competing interests exist.
This study was presented in part at the 46th Annual International Conference of Antimicrobial Agents and Chemotherapy, San Francisco, California, September 27–30, 2006.