
Abstract
Detection of blaKPC-harboring Klebsiella pneumoniae (KP) in the clinical laboratory remains a difficult task. Decreased ertapenem (ERT) susceptibility has been considered one of the most sensitive phenotypic indicators of K. pneumoniae carbapenemase (KPC) production, but has been found to be nonspecific. Susceptibility testing using imipenem or meropenem lacks the sensitivity for detection of KPCs, and there is limited experience using doripenem (DOR). Fifty-five individual ERT-nonsusceptible KP isolates and 19 isolates that were ERT-susceptible, extended spectrum β-lactamase-positive KP were collected from the clinical laboratory and tested for DOR susceptibility by Etest methodology. PCR screening for blaKPC was performed on all specimens. All but three isolates with ERT resistance were KPC positive by PCR. Compared to PCR, ERT detection of KPC had a sensitivity of 98% and a false-positive rate of 6%. Overall, there was a 97% agreement between ERT and DOR susceptibility results. However, there was one KPC-positive isolate that was discrepant (ERT susceptible, DOR nonsusceptible by Etest). Selected isolates of KP from both groups underwent pulsed-field gel electrophoresis analysis to determine the degree of genetic relatedness of KPC-positive and KPC-negative isolates. Pulsed-field gel electrophoresis of selected KPC-positive and KPC-negative KP identified a common pattern between both groups. The resistance to DOR and/or ERT is sensitive and a specific indicator for detection of blaKPC in KP.
Introduction
Methods
From 2005 to 2009, 55 consecutive individual single-patient isolates of KP showing reduced susceptibility to ERT by Etest® methodology (AB bioMerieuex) were collected from the clinical microbiology laboratory in the VA NJHCS. An isolate with a minimal inhibitory concentration (MIC) of >2 μg/ml for ERT was considered ERT nonsusceptible. 11 For DOR, MIC of ≥0.5 μg/ml was considered nonsusceptible based on the U.S. Food and Drug Administration (FDA) breakpoint criteria for Enterobacteriaceae. Of the 55 specimens, 11 isolates that were collected between 2006 and 2007 lost ERT resistance (MIC ≤ 2 μg/ml) when retested. They were re-inoculated into trypticase soy broth containing 2 μg/ml of ERT and grown overnight at 37°C. If growth was noted, the isolate was subcultured onto blood agar plates and retested by Etest. Out of 11 isolates, 8 showed an increase in MIC values in the ERT resistant range, but the other 3 isolates remained ERT susceptible. These three ERT-susceptible isolates, which were originally KPC positive by PCR, on repeat PCR testing were KPC negative and were excluded from the 55 specimens. Nineteen consecutive individual KP isolates that were ESBL positive via double-disk test and ERT sensitive via Etest were also collected during the same time period. They were used as negative controls to assess specificity. All isolates were further examined for the presence of KPC by PCR using previously described primers and methods. 10
As this study was performed before the Clinical and Laboratory Standards Institute (CLSI) came out with new breakpoints for carbapenems, including DOR, we reanalyzed the data using the new 2010 CLSI breakpoints for carbapenems (2010 CLSI M100-S20 Supplement). An isolate with an MIC of >0.25 μg/ml for ERT and >1 μg/ml for DOR was considered ERT and DOR nonsusceptible, respectively.
Lastly, 26 randomly chosen isolates of KPC-positive KP were subjected to pulsed-field gel electrophoresis (PFGE) analysis using XbaI restriction endonucleases and compared to 11 ERT-susceptible, KPC-negative KP, as previously described. 10 These two groups were then compared to KP isolates that were KPC positive from New York Hospital Queens by the Molecular Analyst Finger-printing Software (Bio-Rad). Dendrograms were generated using band-based similarity coefficients. Susceptibility results from Etest were compared with PCR outcomes using McNemar's test. p-Values < 0.05 were considered statistically significant.
Results
Fifty-two ERT-nonsusceptible and 19 ERT-susceptible isolates were collected and included in the study. Before June 2009, all isolates collected in the VA NJHCS that were ERT nonsusceptible by Etest methodology harbored blaKPC by PCR. This correlated with a sensitivity of 100% (49/49) and a specificity of 100% (18/18). After June 2009, three ERT-nonsusceptible isolates that were KPC negative and one ERT-susceptible isolate that harbored blaKPC by PCR reduced the ERT sensitivity and specificity to 98% (49/50) and 86% (19/21), respectively. The three ERT-nonsuceptible isolates had ERT MICs of 32, 32, and 8 μg/ml and DOR MICs of 32, 1.5, and 0.047 μg/ml, respectively. The ERT-susceptible isolate that was noted to carry KPC had an ERT MIC of 2 μg/ml and a DOR MIC of 1 μg/ml (nonsusceptible according to the FDA approved breakpoints). There was 97% (69/71) categorical agreement between ERT and DOR with two discordant results. One of the discordant results was a KPC-negative isolate reported as ERT nonsusceptible but DOR susceptible. The other discordant result was an KPC-positive isolate that was ERT susceptible and DOR nonsusceptible with an MIC of 1 μg/ml. Overall, ERT had a sensitivity of 98% (49/50) and specificity of 86% (19/21) compared to PCR (p = 0.625) and DOR had a sensitivity of 100% (50/50) and specificity of 90% (17/19) compared to PCR (p = 0.5) (Table 1). KPC-producing KP showed higher MIC values for ERT and/or DOR when compared to KPC-nonproducing KP (Fig. 1).

Ertapenem and doripenem minimal inhibitory concentration (MIC) among blaKPC-positive and -negative isolates. *Doripenem had no breakpoints on the 2009 Clinical and Laboratory Standards Institute (CLSI) document, so U.S. Food and Drug Administration breakpoints were used.
This isolate was nonsusceptible to imipenem and meropenem and susceptible to DOR.
Collected after June 2009.
Two isolates were nonsusceptible to imipenem, meropenem, and DOR. One isolate was susceptible to all other carbapenems.
CLSI, Clinical and Laboratory Standards Institute; DOR, doripenem; ERT, ertapenem; KPC, Klebsiella pneumoniae carbapenemase.
When applying the new 2010 CLSI ERT breakpoints, five isolates that were categorized as susceptible where now classified as nonsusceptible with MICs of 0.38, 0.64, 1, 1, and 2 μg/ml. The previous ERT-susceptible (MIC 2 μg/ml) and KPC-positive isolate was now considered ERT nonsusceptible resulting in an ERT sensitivity of 100% for the detection of KPC. With the new ERT breakpoints, the ERT specificity for the detection of KPC was 67%. DOR showed a sensitivity and a specificity of 96% and 90% for detection of KPC, respectively. Two DOR-susceptible isolates (MIC, 1 μg/ml) were KPC positive by PCR and two DOR-nonsuceptible isolates (MIC, 1.5 and 32 μg/ml) were KPC negative by PCR.
Analysis of the PFGE showed three clusters of KPC-producing strains with proportional distribution of the isolates. One of the PFGE clusters (cluster A) showed 100% similarity to previously described New York Hospital Queens isolates (Fig. 2). 10 Three KPC-negative and ERT-susceptible isolates had ≥90% PFGE pattern similarity to cluster A's PFGE pattern (one isolate showing 100% similarity).
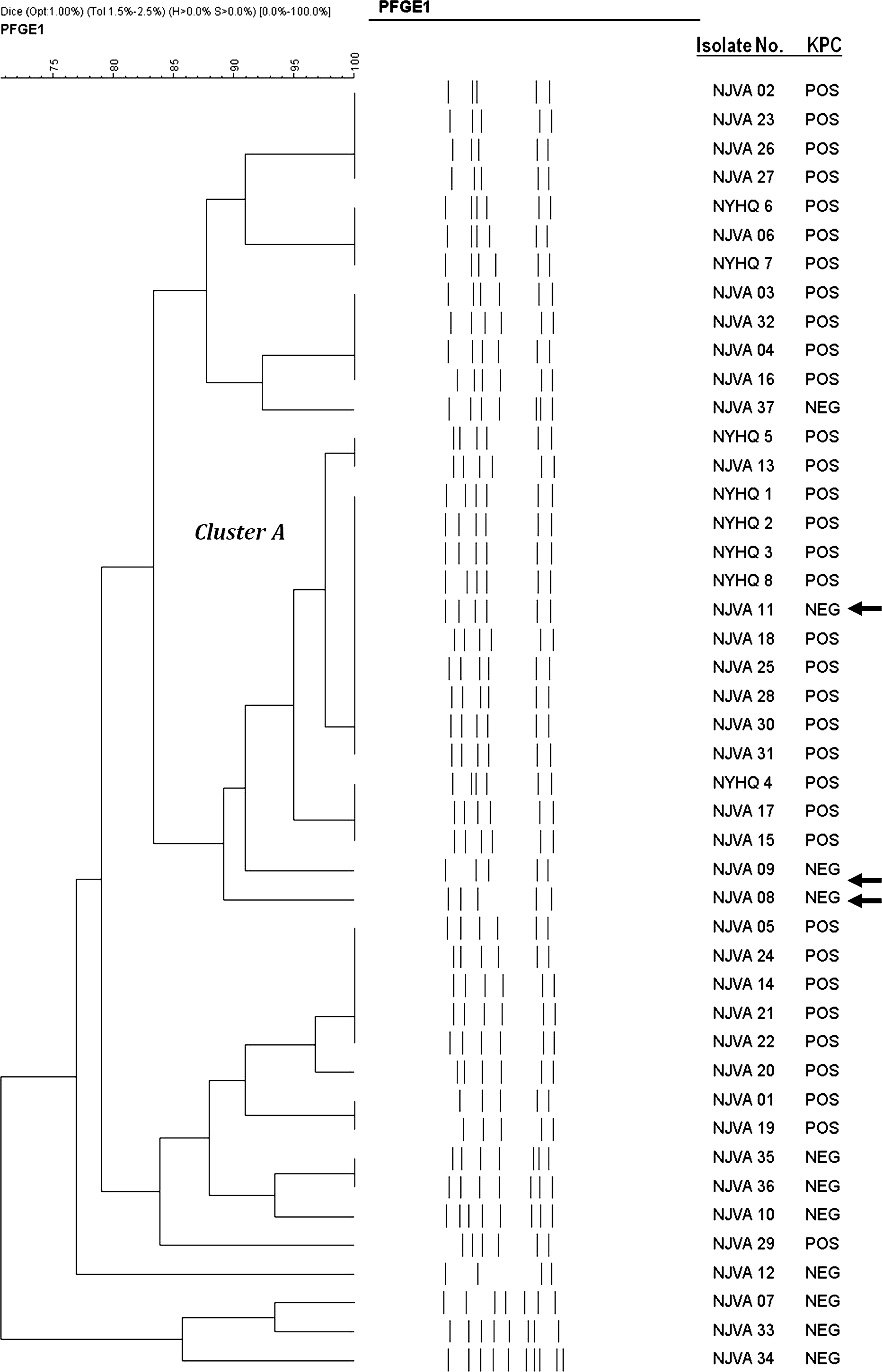
Dendogram showing the predominant cluster A of Klebsiella pneumoniae carbapenemase (KPC)-positive isolates. Arrows indicate the ertapenem-susceptible and KPC-negative isolates with similar pulsed-field gel electrophoresis (PFGE) pattern as the KPC-positive isolates from NYHQ and NJVA.
Discussion
Before the first report of KPC-producing KP in 2001, 32 carbapenem resistance in Enterobacteriaceae was rare and was mainly due to ESBL or AmpC β-lactamases and loss of outer membrane proteins.4,17 However, carbapenem resistance mediated by KPC enzymes became the predominant mechanism in Enterobacteriaceae affecting therapy and mortality.20,31
Dilemmas in detection of ESBL-producing isolates have existed for >15 years and clinical microbiology laboratories are confronted with the same dilemma assessing bacteria possessing KPC enzymes. Automated systems have been noted to misidentify KPC-producing organisms as carbapenem-sensitive strains due to a variety of reasons including inoculum effect and established breakpoints.5,25 Further, once the carbapenem resistance has been detected, the commercial systems cannot correctly infer the mechanism of carbapenem resistance (carbapenemase vs. noncarbapenemase producers). 28 Agar diffusion methods such as Etest and disk diffusion have been noted to be more accurate in the detection of carbapenem resistance. 6 Detection of KPC also relies on the carbapenem used for screening. Bratu et al. reported that ERT was the most sensitive indicator for the detection of KPC-producing KP. 6 Anderson et al. reported similar results with the use of ERT MIC > 1 μg/ml as a screening method; however, these authors also reported the lack of specificity of ERT susceptibility compared to imipenem and meropenem. 1 In a study by Marschall et al., ERT screening showed a low positive predictive value (43%) compared to imipenem (100%). 16 Similar results were also reported by McGettigan et al., showing that KPC screening with ERT had a false-positive rate of 21% in KP. 18 To overcome the lack of specificity of ERT, the modified Hodge test has been implemented in clinical microbiology laboratories to confirm the presence of carbapenemases in isolates with decreased susceptibility to carbapenems. 1 Although CLSI recommended in 2009 to performed a Hodge test on all Enterobacteriaceae with reduced susceptibility to carbapenems, 11 errors with this test have also been documented since carbapenem resistance can be mediated by a variety of mechanism9,22 and relies on laboratory technologists skill and assessment. Boronic acid compounds are β-lactamase (serine-type) inhibitors that have been used for the detection of KPC among Enterobacteriaceae. Phenylboronic acid and 3′-aminophenylboronic acid have shown synergistic effect with carbapenem that have been used for the phenotypic detection of KPC among Enterobacteriaceae.12,23,26,27 This new approach seems to be a promising method for the accurate detection of KPC-producing isolates, but not yet widely available for routine clinical used.
Unlike the previous mentioned studies, our experience with ERT susceptibility testing as a screening method has showed a specificity of 86% and a false-positive rate of 14% (3/21). Until June 2009, all isolates of KP with an ERT MIC > 2 μg/ml were KPC positive and maintained excellent specificity for KPC detection. This may indicate that the predominant cause of decreased carbapenem susceptibility in our institution was mediated by KPC. In the second half of 2009, we encountered three ESBL-positive isolates with decreased ERT susceptibility, which were KPC negative. Although the presence of other carbapenemases and/or porin mutations was not assessed in these isolates, these may be additional factors contributing to the results of these isolates.
We believe that the specificity and positive predictive value of ERT susceptibility will depend on the mechanism of carbapenem resistance prevalent in clinical isolates. In a study from the United Kingdom, 30 a reference laboratory found no KPC among 95 carbapenem-resistant KP isolates suggesting other mechanisms. It was not until 2008 that KPC was detected in KP in the United Kingdom. 29 In our institution the predominant mechanism of carbapenem resistance, up to June 2009, was mediated by KPC. Although the findings of three carbapenem-resistant KPC-negative isolates decreased the ERT specificity from 100% to 86%, we believe that it is still an effective screening test. However, with the new CLSI breakpoints for ERT, the low specificity compromise the utility of ERT by itself as a screening test and the need of the modified Hodge tests as confirmation. The modified Hodge adds specificity to KPC detection in conjunction with ERT susceptibility testing; however, false-positive results in isolates producing ESBL or AmpC enzymes that are able to hydrolyze carbapenems have also been reported.9,22
DOR is the newest member of the carbapenem class of antibiotics approved in the United States. It is stable to hydrolysis by ESBLs and AmpC enzymes and is hydrolyzed slower than imipenem by KPC. 24 DOR performed as well as ERT, showing slightly higher sensitivity and specificity to detect KPC in KP, which may be due to the lower breakpoint established by the FDA. CLSI have now released breakpoints for DOR susceptibility testing. When adapting the CLSI breakpoints to our study, DOR seems to perform better than ERT as a screening test for the presence of KPC with a similar sensitivity (96%) and a better specificity (90%). As there was a very high rate of KPCs in carbapenem-resistant KP in this study, the specificity of DOR in KP mediated by other mechanisms needs to be further assessed.
Although KPC-producing KP showed higher MIC values for ERT and/or DOR when compared to KPC nonproducing KP, a variable MIC range was encountered. Instead of using the reference CLSI broth microdilution to determine the MIC, Etest was used, which has some inherent problems. Etest tend to give higher MIC values among KPC producing Enterobacteriaceae, which could have accounted for the false-positive results seen in this study. 7 However, a recent study showed that Etest tends to have a lower sensitivity for detecting KPC-producing KP when compared to broth microdilution. 13 Also, scatter growth within the zone of inhibition can make interpretation of the MIC difficult. 28
Tenover et al. reported a daily variability of the carbapenem-resistant pattern in KPC-positive KP. 25 We encountered similar findings, as 11 isolates that were originally ERT resistant reverted back to ERT susceptible during cold storage. Although this change of susceptibility pattern could have been due to loss of plasmid during storage of these isolates in media without carbapenem pressure, most isolates regained the carbapenem resistance pattern after exposure to carbapenems. This observation is more consistent with an inherited variability of KPC expression than with loss of the KPC-containing plasmids, which could make the detection of KPC from storage isolates difficult without utilizing molecular methods. Kitchel et al. recently reported on several factors that can influence the level of carbapenem resistance. 14 Mutations of the upstream region of the Tn4401 transposon, number of blaKPC copies, and/or porin mutations can cause variations in carbapenems resistance among KPC-producing isolates. The authors also described the instability of blaKPC-carrying plasmids, as one of the isolates lost the blaKPC-carrying plasmids during passages in vitro. In our study, three specimens lost the KPC gene during storage.
In the United States, a dominant strain of KPC-producing KP, which correlates with a multilocus sequence type 258, has been found in 10 different states and in other countries, including Israel and Belgium.2,3,15 The international dissemination of this strain poses a major threat to healthcare systems on a global scale. PFGE analysis showed three predominant clones in our institution. One of these clones had a PFGE pattern with 100% similarity to several NYQH strains, indicating the possible clonal spread of KPC-producing KP. 10 This is the first study to our knowledge that demonstrated that certain KPC-negative KP are related to KPC-positive strains. Even though multilocus sequencing was not performed, these KPC-negative KP could represent the source of the ST258 type strain that could more efficiently retain the KPC gene; however, more studies are needed to confirm this. If this has indeed occurred, it is of great concern as it has been shown that carbapenem-sensitive KP strains can acquire the KPC gene and that clonal spread is not necessary for the proliferation of the KPC gene. This in turn will make infection control measures more difficult in attempting to contain the spread of carbapenem-resistant KP.
Clinical microbiology laboratories are still coping with detection of organism producing KPC enzymes. We and others have shown that molecular methods are necessary to accurately detect specific enzymes responsible for carbapenem resistance but are not routinely performed in clinical laboratories. Even if the enzymes are detected by PCR, susceptibility testing may not reflect the presence of these enzymes because of lower levels of expression when testing isolates in the laboratory. Therefore, no single method will detect for the presence of these enzymes. Without improved methods of accurately identifying such enzymes, patients infected with KPC bearing isolates may fail therapy with carbapenems.
Footnotes
Disclosure Statement
No competing financial interests exist.