
Abstract
Introduction:
Infections with carbapenem-resistant enterobacteria are an emerging threat. This study reports the microbiologic, clinical, and epidemiologic features and the therapeutic outcomes of the infections caused by carbapenem- and pandrug-resistant Klebsiella emerged in our hospital. Fingerprinting analyses by automated repetitive extragenic palindromic-polymerase chain reaction (rep-PCR) and matrix-assisted laser desorption/ionization-time of flight (MALDI-TOF) mass spectrometry are also compared.
Materials and Methods:
Carbapenem-resistant Klebsiella spp. affecting 13 patients were investigated using automated rep-PCR (DiversiLab System) and MALDI-TOF. Species identification was performed by Vitek 2 System and MALDI-TOF. Antimicrobial susceptibility testing was made using Vitek 2 System and Etest. Screening for extended spectrum beta-lactamase (ESBL) and carbapenemase production was made by double disk synergy and Hodge tests, respectively. Synergy studies were performed using Etest. DNA array was used for detection of KPC and ESBLs. blaVIM-1 gene was amplified by PCR and sequencing. Use of carbapenems in the hospital was studied.
Results:
A total of 13 patients were found to be colonized/infected with carbapenem-resistant Klebsiella. All patients were previously submitted to surgery and/or presented with severe underlying disease. After carbapenem-resistant Klebsiella isolation, the majority of the patients were treated with amikacin plus carbapenem, tigecycline, or fosfomycin. All Klebsiella isolates (n = 14), except two, had the blaVIM-1 gene and all Klebsiella pneumoniae also had blaSHV gene associated with ESBL production. DiversiLab system showed higher discriminatory power than MALDI-TOF for strain typing.
Conclusions:
The risk of a rapid dissemination and the persistence of these multidrug-resistant strains through the time determine the need to implement routine procedures for metallo-beta-lactamase detection and measures for prevention of the spread of these microorganisms. The combined use of MALDI-TOF for species identification and DiversiLab System for clonal strain typing may be a useful tool for fast and accurate management of nosocomial outbreaks. The potential clinical utility of fosfomycin in this matter should be considered in future studies.
Introduction
Infections with gram-negative MBL-producing bacteria are an emerging threat in healthcare institutions. The number of Enterobacteriaceae isolated from clinical samples carrying MBLs in Europe has increased over the last few years4,31,32,35 but, so far, it remains uncommon worldwide, except in Greece.13,21
Nowadays, few reports and clinical data are available for the management and empirical treatment of infections due to bacteria resistant to all empiric used antibiotics (pandrug-resistant bacteria [PDR]).12,14,33 Because of the increasing number of multidrug-resistant (MDR) bacteria and spread of plasmids with resistance genes in gram-negative bacteria, fast techniques for routine strain typing in the clinical microbiology laboratory such as automated rep-polymerase chain reaction (PCR) or whole-cell matrix-assisted laser desorption/ionization-time of flight mass spectrometry (MALDI-TOF MS), are useful tools.15,17,18,26
We report the microbiologic, clinical, and epidemiologic features and the therapeutic outcomes of the infections caused by carbapenem-resistant and PDR Klebsiella emerged in our hospital. We also compare fingerprinting analysis results obtained by automated rep-PCR and MALDI-TOF MS.
Methods
Patients and bacteria
From September 2009 through May 2010, a total of 13 patients were found to be colonized or infected with carbapenem-not-susceptible Klebsiella isolates (9 patients with Klebsiella oxytoca [KOXY] and 4 with Klebsiella pneumoniae [KPN]). All patients had surgical procedures and presented with severe underlying disease, mainly immunosuppression and/or neoplasia. Six patients were located in critical care units at the moment of MDR-Klebsiella isolation. The isolates were recovered at University Hospital Complex of Santiago de Compostela (Spain), a 1,120-bed teaching hospital in the northwest of Spain. All patients were from Spain.
Phenotypic study
Species identification was performed by Vitek 2 System (ID-GN card) (BioMérieux) and by MALDI-TOF-MS using MS AXIMA (Shimadzu) coupled with the SARAMIS software for spectra analysis (BioMérieux). MALDI-TOF MS spectra were acquired using cells from a single bacterial colony grown on sheep blood agar for 24 hr that were transferred to a target spot of a steel target plate and overlaid with 0.5 μl of 2,5-dihydroxybenzoic acid matrix (BioMérieux). Protein mass fingerprinting were obtained with detection in the linear model at a laser frequency of 50 Hz within a mass range of 2,000–20,000 Da. A minimum of 20 laser shots per sample was used to generate each ion spectrum. For each sample, a total of 50 mass fingerprints were averaged and processed. Calibration was done for each target plate using spectra of the reference strain Escherichia coli CCGU10979 provided by the manufacturer.
Antimicrobial susceptibility testing of isolated bacteria was assayed using Vitek 2 System (AST-N113 card) (BioMérieux) and Etest (BioMérieux). Results were interpreted according to the Clinical and Laboratory Standards Institute guidelines.5,6
In vitro synergy testing for carbapenems and amikacin plus fosfomycin was performed by Etest combination strips fixed ratio method, which is based on replacing the Etest strip on the plate, calculation of the fractional inhibitory concentration index (FIC index), and interpretation according to manufacturer's instructions (BioMérieux).
Extended spectrum beta-lactamase (ESBL) production was studied by modified double disk synergy test. 24
Carbapenemase production was screened by modified Hodge test 19 and MBL production by Etest MBL strips (BioMérieux) with 0.5 McFarland inoculum.
Molecular detection of beta-lactamases
PCR assays were carried out to amplify the entire sequences of the blaIMP and blaVIM genes with the oligonucleotide primers and PCR conditions described by Yan et al. 36 The amplicons were purified and sequenced with the primers previously described. 36
The Check-Points KPC/ESBL array (Check-Points) was used for identification of the presence of KPC and TEM, SHV, and CTX-M ESBLs and the mutations leading to extended spectrum for TEM and SHV variants based on carefully selected single-nucleotide polymorphisms markers. 7 This is an efficient, fast, reliable assay, able to detect the most important ESBLs and to distinguish between ESBL and non-ESBL TEM and SHV variants.10,23
Strain typing of carbapenem-resistant isolates
The DiversiLab DNA fingerprinting kit (BioMérieux) was used for rep-PCR amplification of noncoding intergenic repetitive elements in the genomic DNA of Klebsiella. Rep-PCR conditions were as proposed by the manufacturer. The amplicons were analyzed using the DiversiLab system (BioMérieux). Data analysis was performed with the web-based software using the Pearson and Kullback-Leibler coefficients to determine distance matrices and the unweighted pair group method with arithmetic mean to create dendrograms. Reports were automatically generated and included in the dendrogram, electropherograms, virtual gel images, scatter plots, and selectable demographic fields to aid in interpretation of the data. Sample relationships for rep-PCR were designated as follows: indistinguishable, >97% similarity and no band differences; similar, >95% similarity and one to two band differences; and different, <95% similarity and three or more band differences, as done by other authors1,17 and recommended by the manufacturer. Carbapenem-sensitive K. pneumoniae from our private collection was included as unrelated strain control.
Cluster analysis was also done based on comparison of strain-specific mass spectra obtained using MALDI-TOF MS, as previously described, by applying the single link agglomerative algorithm of SARAMIS™. 26 Allowed mass deviation was 800 ppm. Distance trees were compared with those obtained by DiversiLab System.
Carbapenem usage data
We examined the pattern of carbapenem usage in the hospital as a whole. The defined daily dose (DDD) of carbapenem was 2 g for imipenem and meropenem and 1 g for ertapenem. Data were expressed as the DDDs per 100 patient-days of bed occupancy in the hospital.
Results
Patients and bacterial isolates
Epidemiological data of the patients are shown in Table 1. One patient (no. 351) was an outpatient but had been admitted to the hospital a month before to undergo kidney transplant. Only one patient (no. 352) had been previously treated with carbapenem (imipenem) and three patients (nos. 354, 361, and 362) had no antibiotic treatment, at least, in the 3 months before Klebsiella isolation. After carbapenem-resistant Klebsiella isolation, the majority of the patients were treated with a combination of amikacin and meropenem, ertapenem, tigecycline, or fosfomycin.
CoCU, coronary critical care unit; GS, general surgery; ICU, intensive care unit; NEU, neurology; NEUS, neurosurgery; NO, nephrology outpatient; PSCCU, postsurgery critical care unit.
Six patients (nos. 351, 362, 364, 365, 380, and 386) had MDR Klebsiella in more than one body site (patient 351: urine and peritoneal fluid; patient 362: urine and tracheal aspirate; patient 362: wound, peritoneal fluid, blood, urine, and catheter tip; patient 365: tracheal aspirate and catheter tip; patient 380: tracheal aspirate, catheter tip, blood, peritoneal fluid, and feces; patient 386: lung and liver biopsy, blood, pleural fluid, tracheal aspirate, and catheter tip).
The timing of isolation of the MBL producer in relation to the patient's admission ranged between 11 and 28 days, with a median value of 19 days. The index case was not identified.
Detection of MBL and ESBL
The modified Hodge test and MBL Etest strip yielded positive results for all isolates except for the K. oxytoca no. 354, for which only the ESBL synergy test was positive. Table 2 shows the results of the molecular studies. The blaVIM-1 gene was found in all K. oxytoca isolates except one (KOXY354). An ESBL-producing K. pneumoniae isolate, which lacks blaVIM-1 gene (KPN365h), was recovered from feces and peritoneal fluid of the patient 365. All K. pneumoniae were also positive for SHV ESBL and TEM non-ESBL by microarray analysis.
MICs were determined by Etest except for CI and SXT (Vitek 2).
Strain isolated from feces and peritoneal liquid of patient 365.
IP, imipenem; MP, meropenem; ETP, ertapenem; DOR, doripenem; AT, aztreonam; CI, ciprofloxacin; GM, gentamicin; TM, tobramycin; AK, amikacin; CL, colistin; TGC, tigecycline; C, chloramphenicol; FOS, fosfomycin; SXT, trimethoprim/sulfamethoxazole; MIC, minimal inhibitory concentration.
The prevalence rate of carbapenem-resistant and MBL-positive isolates among Enterobacteriaceae between 2006 and 2010 in our institution is shown in Table 3. As seen, MBL-producing strains emerged in 2009 with a prevalence rate of 0.25. In 2010, the prevalence rate was more than six times higher than that in 2009. During the 9 months of this study, 520 Klebsiella isolates were recovered in the laboratory, of which 13 had reduced susceptibility to carbapenem (2.5%).
Antimicrobial susceptibility
Minimal inhibitory concentrations (MICs) of imipenem and ertapenem were in all cases above the breakpoint for susceptibility proposed by the recently published CLSI guidelines. 6 Imipenem displayed higher MICs than the other carbapenems assayed. All isolates were resistant to all penicillin-inhibitor combinations and broad-spectrum cephalosporins. MBL-producing K. oxytoca isolates had sensitivity to amikacin and colistin; however, MBL-producing K. pneumoniae isolates were highly resistant to aminoglycosides and colistin (Table 2). In all but three isolates, fosfomycin MIC was ≤64 μg/ml, but colonies were observed within the ellipse around the Etest strip.
Synergy studies
No synergy relation was seen between imipenem, ertapenem and amikacin plus fosfomycin. Additive relation between carbapenem plus fosfomycin, and indifference between amikacin plus fosfomycin was found.
Treatments of the patients
The treatments initiated in the infected patients after isolation of MDR-Klebsiella are shown in Table 1. Most of them (8/10) were treated with amikacin ± carbapenem or tigecycline. The majority of colonized patients were not treated with antibiotics. Five of the 10 infected patients had a favorable outcome after the treatment.
Clonal relationship
As shown in Fig. 1, using DiversiLab System we found two clusters for MBL-producing Klebsiella isolates: one for K. oxytoca and a second one for K. pneumoniae. The percentage of similarity between the only non–MBL-producing strain (KOXY354) and other K. oxytoca isolates was 53.4%. So, the ESBL-producing K. oxytoca isolate from patient 354 was clonally unrelated to the remaining MBL-producing K. oxytoca isolates. The KPN365H isolate showed a different rep-PCR fingerprinting profile.
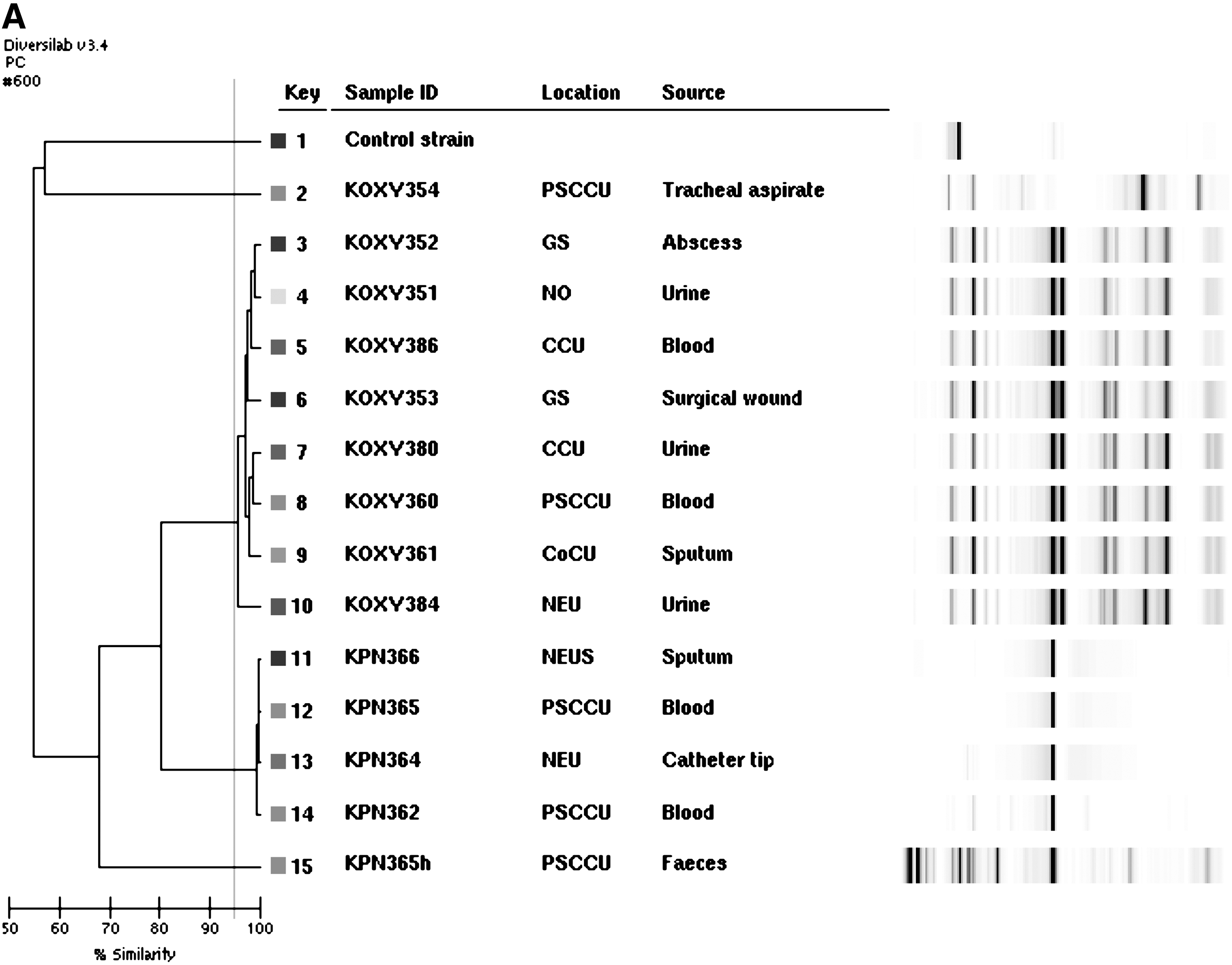
Dendrogram obtained by rep-polymerase chain reaction of carbapenem-resistant Klebsiella spp. from 13 studied patients using Pearson coefficient
Phylogenetic analysis based on MALDI-TOF spectra comparison showed one cluster for MBL-producing K. oxytoca and one cluster for nosocomial K. pneumoniae, with similarity above 65% and 70%, respectively (Fig. 2). The clustering results were similar to that obtained by DiversiLab except for isolate KPN365h, which was considered as a different strain by rep-PCR but not by MALDI-TOF spectra analysis. The similarity between KOXY354 and MBL-producing K. oxytoca was over 40%.
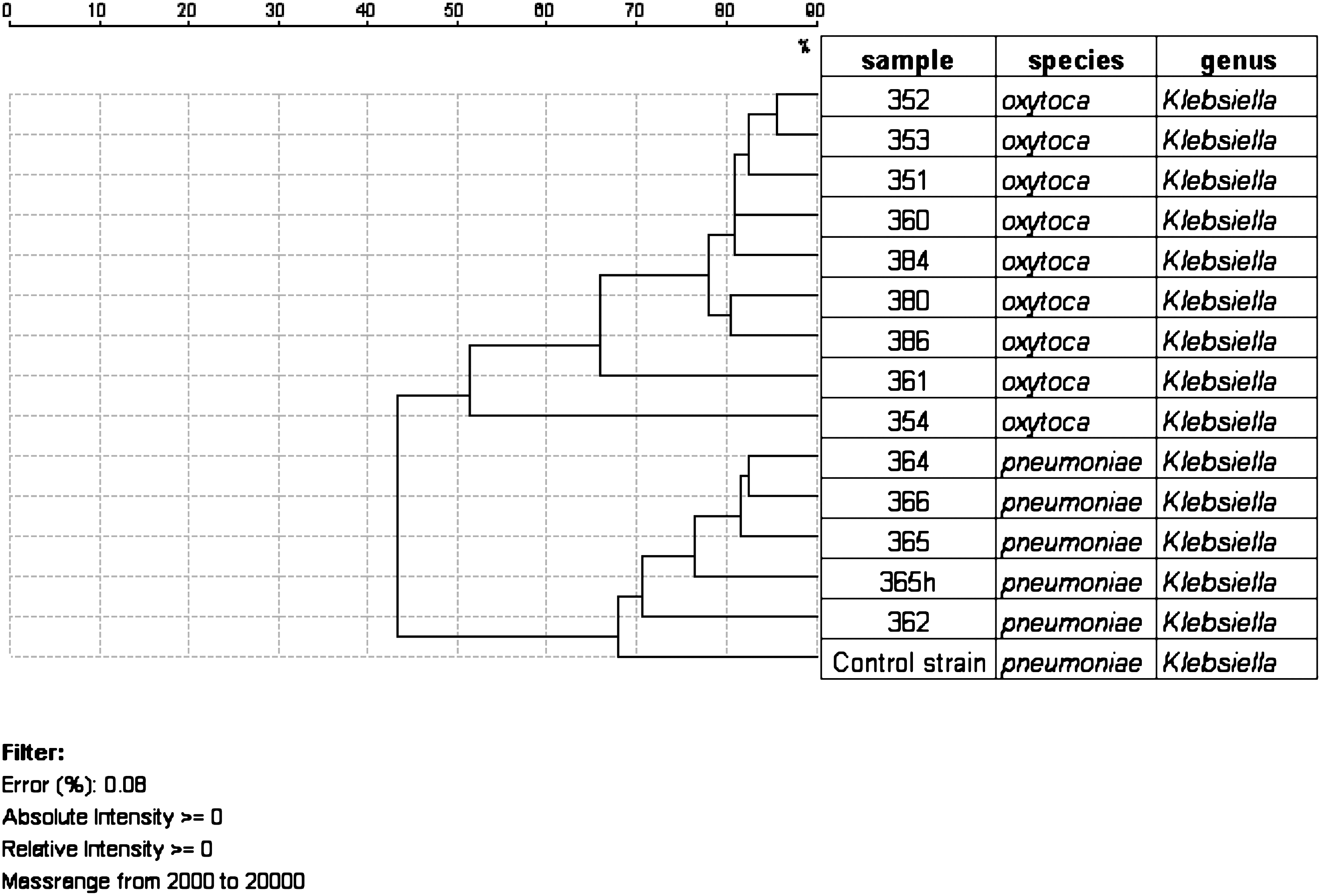
Dendrogram created by matrix-assisted laser desorption/ionization-time of flight spectra analysis of carbapenem-resistant Klebsiella spp. from 13 studied patients.
Carbapenem usage
Carbapenem consumption in our institution has steadily increased over the 2 years before emergence of carbapenem-resistant enterobacteria. The numbers of DDDs of imipenem, meropenem, and ertapenem per 100 patient-days increased from 3.29, 2.69, and 0.53 in 2008 to 4.70, 3.65, and 0.73 in 2010, respectively.
Discussion
Association between severe underlying diseases, mainly neoplasia, and a higher risk for infections with MDR bacteria have been established and can be seen,2,9 also, in our study. However, unlike observations of Daikos et al., 9 wherein staying in intensive care unit and extensive exposure to antibiotics, especially carbapenems, were independent risk factors for VIM-producing Klebsiella, in our cases, only one patient had been previously treated with carbapenem and less than half of them were admitted at a critical care unit at the moment of MDR-Klebsiella isolation. One patient had been formerly treated with ciprofloxacin, which is considered by other authors as an independent predictor for isolation of carbapenem-resistant organisms.11,28 All MBL-producing isolates had the blaVIM-1 gene, which is the most prevalent MBL reported in Enterobacteriaceae in Europe.30,34 In our study, in most cases, imipenem showed higher MICs than ertapenem and meropenem. This was just the reverse in ESBL-producing K. oxytoca isolate, in which the high MIC values for carbapenems were most probably due to combined production of ESBL and loss of porin as observed by other authors.16,29,37
All isolates showed imipenem and ertapenem MICs over the breakpoints recently established as susceptible by CLSI. 6 However, in two cases, MIC values of meropenem and doripenem were below the breakpoints (i.e., susceptible). The finding that MBL-producing Enterobacteriaceae strains may be susceptible to carbapenems may have important clinical consequences, because infections caused by these organisms may not favorably respond to carbapenem treatment because of a sudden increase of blaVIM expression during treatment. 8 On the other hand, this reduced and changeable susceptibility to carbapenems and the possible expression of other beta-lactamases make the phenotypic detection of MBL-producing Enterobacteriaceae difficult in the routine clinical laboratory testing. We found differences in the carbapenem resistance levels among isolates of the same fingerprinting profile as has also been observed by other authors. 31 Differences in the carbapenem resistance levels observed may be due to the variable expression of the MBL gene as a consequence of different promoters or differences in the gene copy number. 20 All K. pneumoniae were resistant to aztreonam, although this drug is not hydrolyzed by MBLs, because these isolates also produced an SHV-type ESBL. The presence of genes encoding ESBL was detected by using microarray technology. This method has been previously evaluated7,10,23 and provides definitive results within the same working day, allowing rapid implementation of isolation measures and appropriate antibiotic treatment being an interesting tool for routine laboratory testing.
Six patients with MDR-K. oxytoca infection were treated with amikacin plus/less carbapenem and four of them had a successful outcome. Because of acute renal failure, patient 386 could not be treated with amikacin and was treated with tigecycline. He died because of septic shock. The patients who were infected with PDR-K. pneumoniae did not favorably evolve with the prescribed treatments. Patient 366 was considered colonized by MDR-K. pneumoniae and meropenem was used for broad-spectrum coverage.
Two of the patients infected with MBL-producing strains that were treated with carbapenems died. It is very important to highlight that there is a risk of using cabapenems for treatment when carbapenemase production is detected despite intermediate MIC values were tested.
Patient 362 initially had a poor outcome and treatment was changed to fosfomycin plus amikacin but, after 11 days, the bacterial isolate recovered from surgical wound showed higher fosfomycin MIC (128 μg/ml). Fosfomycin is an old antibacterial drug with various clinical indications. 12 There are few studies on fosfomycin in vitro antimicrobial activity against clinical MDR and PDR Enterobacteriaceae isolates and clinical data are very scarce.12,14 Because of the high risk for development of resistance in the course of treatments with fosfomycin, this drug is usually administered in combination with other antibiotics, although no studies have demonstrated a consistent synergistic effect against Enterobacteriaceae. In our case, despite the use of fosfomycin in combination with amikacin, the bacterial strain developed resistance in few days of treatment perhaps because of inefficacy of amikacin. However, we do not have enough experience to recommend or not the treatment with fosfomycin.
The detection, as soon as possible, of the possible spread of these MDR strains within the hospital is very important because blaVIM-1 gene is usually associated with other determinants of resistance such as qnrS and aac-(6′)-Ib-cr genes that cause quinolone and aminoglycoside resistance and difficult-to-treat infections.22,30 Clonal dissemination of an MDR strain or dissemination of plasmids with the resistance genes from one species to another could have happened in our hospital. In our case, this situation is especially serious, because the K. pneumoniae strain is a PDR bacterium.
Automated rep-PCR using DiversiLab system has been proved as a rapid and reliable laboratory method for molecular confirmation of suspected nosocomial outbreaks. 15 DiversiLab fingerprinting profiles demonstrated that all MBL-producing KOXY and KPN isolates were genetically related, respectively. In the dendrogram, KOXY354 strain could seem to be closer to K. pneumoniae strains than to the other K. oxytoca, but, taking into account the similarity percentage, KOXY354 is closer to the K. oxytoca cluster than to the K. pneumoniae strains. We must keep in mind that the dendrogram provided on the DiversiLab software is not a tool for phylogenetic classification of bacteria but is a help to identify clusters and compare the graphs within one cluster. DiversiLab System results may be analyzed using different coefficients: Pearson (PC) and Kullback-Leibler (KL). In PC analysis, both the band presence and the intensity are important. In KL analysis, the band presence is more important than the band intensity. Either way, the interpretation should be the same because it is based on the number of band differences.
On the other hand, MALDI-TOF is a modern technique that has been evaluated for rapid identification of bacteria. So far, there are very few studies that evaluate the usefulness of this technique for phylogenetic classification at the strain level.18,26 In the present case, the dendrogram constructed from data provided by MALDI-TOF spectra shows, as with DiversiLab, one cluster for MBL-producing K. oxytoca and one cluster for nosocomial K. pneumoniae. Also, as with rep-PCR, the similarity between KOXY354 and MBL-producing K. oxytoca is higher than between KOXY354 and K. pneumoniae strains. However, in the present study, rep-PCR exhibited greater power of discrimination than MALDI-TOF as it can be seen in the case of the strain KPN365h. This strain, which had different antibiogram and resistance mechanisms, is considered as a different cluster with the rep-PCR analysis but not when MALDI-TOF spectra are compared. The reason is, probably, that rep-PCR covers all bacterial chromosome; however, the main signals reported in MALDI-TOF MS belong to ribosomal proteins. 27 Other authors have also reported good discriminatory power of automated rep-PCR.15,25
At the moment, MALDI-TOF is an accurate and very fast tool for microbial identification but, regarding strain typing, more studies with bigger strain collections are needed to establish the correlation between the coefficients of similarity obtained by MALDI-TOF and other strain typing methods such as rep-PCR.
Carbapenem use at our institution has steadily increased over the 2 years before the worrying emergence of carbapenemase-producing enterobacteria (42%, 35%, and 37% for imipenem, meropenem, and ertapenem, respectively). This increase has occurred in parallel with the emergence of carbapenem-resistant and MBL-producing enterobacteria.
As a result of the serious increase in MBL-Klebsiella rates, the interventions made to control the outbreak were to reinforce hand-washing procedure, 2% clorhexidine gluconate baths for colonized/infected patients, intensification of the environmental cleaning measures, surveillance cultures at admission and twice per week for previously admitted patients in critical care units, and isolation precautions. Stricter control of carbapenem-prescribing practices was instilled: imipenem and meropenem treatment is reserved for serious infections after failure with other antibiotics, immunosuppressed patients, infection caused by MDR–gram-negative bacilli, and monotherapy treatment of acute pancreatitis. Reasonable use of this group of antibiotics, escalating whenever possible, is essential to safeguard its usefulness in the immediate future. From May to November 2010, five new cases of MBL-producing Klebsiella have been detected in our institution. Probably, there is only little time to assess the effectiveness of the measures adopted.
Conclusions
The emergence of MDR and PDR Enterobacteriaceae is a serious problem for the treatment of nosocomial infections, which are, moreover, associated with a high rate of mortality. As treatment with carbapenems may lead to treatment failure in MBL-producing enterobacteria, although CMI values are low, we consider a priority to implement in the laboratory routine procedures for MBL detection. The combined use of MALDI-TOF for species identification and DiversiLab System for clonal strain typing may be a useful tool for fast and accurate management of nosocomial outbreaks, avoiding the dissemination of these organisms with the transfer of patients to different wards and the persistence of these strains through time. As therapeutic options for MDR and PDR Enterobacteriaceae have not been well established, the potential clinical utility of fosfomycin in this matter should be considered in future studies.
Footnotes
Disclosure Statement
The authors declare that they have no competing financial interests.