
Abstract
The emergence of infections caused by multidrug-resistant Gram-negative bacteria, in particular Pseudomonas aeruginosa, Acinetobacter baumannii, and Klebsiella pneumoniae, has necessitated the search for alternative therapy by either introducing new agents or renewing interest in old agents. This study compares the in vitro activity of tigecycline (TIG), recently introduced to Egyptian market, to other potentially active antimicrobials as Colistin (COL), imipenem (IPM), levofloxacin (LEV), and piperacillin/tazobactam (PIP/TAZ) against 67 Gram-negative clinical isolates obtained from El- Meery Hospital in Alexandria, Egypt. El-Meery Hospital is a 1,500-bed tertiary teaching hospital where TIG has not been previously used. Based on MIC90s, TIG was found to be a comparator to IPM and COL (MIC90 = 8 μg/ml). LEV and PIP/TAZ were less active than TIG exhibiting high MIC90s. TIG inhibited 100% of Escherichia coli and K. pneumoniae and 60% of Ps. aeruginosa and A. baumannii isolates. In time-kill studies against IPM-resistant isolates, TIG showed bactericidal activity after 6 hours of contact against the Enterobacteriaceae isolates and after 3 hours for the tested Ps. aeruginosa isolates at 4 × and 8 × MIC. Against A. baumannii, TIG exerted a bacteriostatic effect. TIG demonstrated variable ability to suppress biofilm formation affecting mainly E. coli and A. baumannii isolates. These results point TIG to be a promising agent in treatment of infections caused by strains for which adequate therapy has been limited. As far as we know, this is the first report evaluating the in vitro activity of TIG against Egyptian clinical isolates.
Introduction
Tigecycline (TIG), the 9-t-butylglycylamido derivative of minocycline, is the first recently licensed glycylcycline designed to evade both ribosomal- and efflux-mediated resistance common to classical tetracyclines 21 and possessing activity against most Enterobacteriaceae and Acinetobacter spp. 32 Colistin (COL), almost abandoned for many years due to its reported toxicity, has been recently reintroduced as a drug of last resort for treating infections caused by multidrug resistant isolates. 13 For the empirical therapy of severe infections, imipenem (IPM), the first carbapenem developed more than two decades ago, continues to play a leading role. 31 An efficacious and safe alternative to IPM-cilastatin, frequently prescribed for the treatment of nosocomial pneumonia and peritonitis, is the combination of piperacillin and tazobactam (PIP/TAZ). 11 With its excellent pharmacokinetic and pharmacodynamic features, levofloxacin (LEV) has demonstrated effectiveness in the treatment of community-acquired respiratory tract infections and acute bronchitis. 35
Nevertheless, it seems that the implication of an adequate antimicrobial therapy is threatened by an additional barrier: bacterial biofilms that impact the treatment by adhering to foreign surfaces and forming a matrix-like coating, preventing the penetration of antibiotics. 24 In addition, it has been demonstrated that biofilm-grown bacteria have an inherent lack of susceptibility to antibiotics, which has led to problems in their eradication complicating even more the never-ending global battle against bacterial resistance. 19
This study was performed to compare the in vitro activity of TIG to other potentially active antimicrobials; COL, IPM, LEV, and PIP/TAZ, against different Gram-negative isolates collected from hospitalized inpatients admitted to El-Meery hospital, a 1,500-bed tertiary teaching hospital in Alexandria, Egypt, where TIG has not been previously used. In addition, this work assessed the effect of these antimicrobials on the biofilm formation by the tested isolates.
Materials and Methods
Test organisms
A total of 69 Gram-negative microorganisms were used in this study. Sixty-seven were collected in a clinical microbiology laboratory affiliated with El-Meery tertiary teaching hospital over 3 months (from March to May 2010). The clinical specimens were obtained from wounds (n = 7), blood (n = 11), urine (n = 19), sputum (n = 14), and broncho-alveolar lavage (n = 16). The microorganisms were 23 Escherichia coli, 14 K. pneumoniae, 15 Ps. aeruginosa, and 15 A. baumannii isolates. E. coli NCTC 10418 and Ps. aeruginosa ATCC 9027 were used as quality control strains.
Antibiotic powders
IPM (Merk Sharp & Dohme Limited), LEV (Amoun Pharmaceutical Company), PIP/TAZ (Wyeth Pharmaceuticals), and TIG (Wyeth Pharmaceuticals) were purchased from pharmaceutical markets. Colistin sulfate (COL; Sigma-Aldrich) was obtained as a gift from Pharco Pharmaceutical Company.
Bacterial identification
Identification was carried out by means of conventional methods and included morphological, tinctorial, and cultural properties and also biochemical characteristics that were estimated by API system (BioMérieux). For A. baumannii isolates, a growth temperature of 44°C was used to confirm identity of these isolates. The identified strains were stored frozen at −70°C in nutrient broth (Oxoid) containing 20% glycerol until needed for further tests.
Antimicrobial susceptibility testing
The in vitro activity of the five antimicrobial against the tested isolates was determined by the broth microdilution method in accordance with Clinical and Laboratory Standards Institute (CLSI) guidelines. 5 TIG powder was dissolved in situ and prepared according to instructions from the manufacturer. Microtiter plates (ROLL sa.s.), containing serial dilutions of each antimicrobial agent in Mueller-Hinton broth (Oxoid), were inoculated with each organism to yield the appropriate density (105 CFU/ml) in a final volume of 180 μl. The plates were incubated for 24 hours at 35°C. The MIC was defined as the lowest concentration of antimicrobial agent that completely inhibits the growth of the organism as detected by the unaided eye. Tests for TIG susceptibility were performed using fresh Mueller-Hinton broth (<12 hours old). 3 Susceptibility rates were determined using CLSI breakpoints except for TIG. 5 The U.S. Food and Drug Administration (US FDA) criteria were followed for susceptibility interpretation of TIG (≤2 μg/ml susceptibility; ≥8 μg/ml resistance according to TIG package insert).
Comparative biocidal activity of TIG and COL against selected strains
In vitro bactericidal activity of each of TIG and COL against eight IPM-resistant isolates was evaluated using time-kill assays. Probe tubes contained TIG or COL at concentrations corresponding to the MIC, four and eight times the MIC for each strain. Tubes were incubated aerobically at 35°C for 24 hours. Aliquots were removed from each tube and serial dilutions were plated in duplicates onto Mueller-Hinton plates after 0, 3, 6, and 24 hours of incubation. Colony counts were performed after 24 hours of incubation at 35°C. Bactericidal activity was defined as a 3 log10 reduction compared with the initial inoculum. In each case, an antibiotic-free control was included in the procedure.
Effect of subinhibitory and minimum inhibitory concentrations of the tested antibiotics on biofilm formation
Dilutions of the five tested antibiotics, corresponding to ¼, ½, and 1 × MIC, were prepared. Aliquots of 90 μL of each dilution were distributed, in duplicates, in the wells of a sterile 96-well microtiter plate. Equal volumes of double-strength nutrient broth, inoculated with the test microorganism, were transferred to each of the wells. Controls in which the antibiotic solution was replaced by 90 μL of sterile water were included. The plates were wrapped in aluminum foil and incubated overnight at 35°C. After incubation, the planktonic cultures were discarded and the plates were washed with saline. The attached biofilm was then stained using 1% crystal violet (100 μL per well) for 15 minutes. The stain was discarded; the plates were washed with saline and left to dry. The stained plates were then examined by recording the optical density at 630 nm using the absorbance microplate reader (Biotek) according to Dobinsky et al. 7 Average of two readings was calculated and used to draw the histograms.
Results
Antibiotic susceptibility testing
The in vitro activity of the five antimicrobials against the collected Gram-negative isolates is summarized in Table 1. The results show that 80.6% of the isolates (n = 67 strains) were IPM susceptible and a comparable susceptibility of 73.2% for TIG was observed. Moderate activity with a percentage of susceptibility equal to 62.7% was noticed for COL. Low activity, with MIC90 values of 64 and ≥512 μg/ml, was exerted by LEV and PIP/TAZ (percentages of susceptibility were 43.3% and 40.3%, respectively). Eight isolates (11.9%) were resistant to IPM (MICs 16–512 μg/ml); all but two were susceptible to TIG with MICs ranging from 0.5 to 2 μg/ml. Among the 21 isolates (31.3%) resistant to COL, 16 were still susceptible to TIG (MIC range was ≤0.5–2 μg/ml). For the 36 isolates (53.7%) displaying resistance to LEV, only 5 were also resistant to TIG. Thirty isolates (44.8%) were resistant to PIP/TAZ, among which 22 remained susceptible to TIG. Conversely, among the 12 isolates (17.9%) resistant to TIG, 4 isolates were susceptible to PIP/TAZ.
MIC50 and MIC90, MICs (μg/ml) for 50% and 90% of isolates tested, respectively.
Regarding the different types of isolates tested in this study (Table 2), the activity of COL and PIP/TAZ was rather similar for E. coli isolates with 13.0% resistance. IPM showed 4.4% resistance. TIG inhibited all of the E. coli tested isolates (MIC50 and MIC90 values were 1 and 2 μg/ml, respectively). Sixteen E. coli isolates (69.6%) displayed resistance to LEV with MIC range of 16–128 μg/ml. No K. pneumoniae isolates were resistant to TIG (MIC50 was 1 μg/ml), whereas 14.3% of these isolates were resistant to IPM. All but three of the K. pneumoniae isolates showed resistance to LEV and very low susceptibility (7.1%) was observed, as well, when testing PIP/TAZ. At a concentration of 8 μg/ml, 80.0% of the Ps. aeruginosa isolates were inhibited by TIG as well as IPM, whereas the same concentration of PIP/TAZ inhibited only 53.3% and a higher concentration of LEV (32 μg/ml) was needed to inhibit the same percentage. The MIC90 values for both IPM and COL were 32 μg/ml against A. baumannii isolates as compared to 16 μg/ml for TIG. Two A. baumannii isolates were resistant to IPM, one of them showed susceptibility to TIG. About 44.4% of A. baumannii isolates resistant to COL showed susceptibility to TIG.
Bold figures indicate CLSI breakpoints applied for resistant isolates; colistin: 4 μg/ml; levofloxacin, tigecycline (FDA-approved breakpoint): 8 μg/ml; imipenem: 16 μg/ml; piperacillin/tazobactam: 64 μg/ml.
MIC for these isolates was greater than or equal to the indicated value.
CLSI, Clinical and Laboratory Standards Institute; FDA, Food and Drug Administration.
Time-kill studies
The in vitro bactericidal activity of COL and TIG, at concentrations corresponding to one, four, and eight times the MIC, against eight IPM-resistant isolates was evaluated using time-kill assays. At all tested concentrations, COL showed bactericidal activity after 3 hours with a re-growth after 24 hours for the tested isolates. At TIG concentrations of 4 × and 8 × MIC, a decrease in the viable count by ≥3 log10 cfu/ml was observed after 6 hours of contact for the Enterobacteriaceae isolates and after 3 hours for the tested Ps. aeruginosa isolates. In contrast, TIG displayed only bacteriostasis against the tested A. baumannii isolates. Similarly to COL, re-growth occurred after 24 hours at 1 × MIC of TIG with all of the isolates included in the study.
Effect of MIC90 of COL, IPM, and TIG on biofilm formation by tested isolates
The influence of the MIC90 of COL, IPM, and TIG, for each type of organism, on the biofilm formation was investigated in microtiter plates (Fig. 1a–d). The results were read colorimetrically and a value of 0.1 or higher was taken as a positive indication for biofilm formation. All biofilms formed in presence of the tested antibiotics showed lower absorbance reading than the corresponding control. Biofilm formation was prevented by IPM and COL in almost all isolates with few exceptions: most notably observed with E1 and E9 in E. coli, K206 in K. pneumoniae, P3651 in Ps. aeruginosa, and A9 in A. baumannii isolates. TIG demonstrated a variable ability to suppress biofilm formation affecting mainly E. coli (except E3B and E102) and A. baumannii isolates. On the other hand, K. pneumoniae isolates mostly retained their ability to form biofilms in the presence of MIC90 of TIG yet to a lower extend than their corresponding controls.
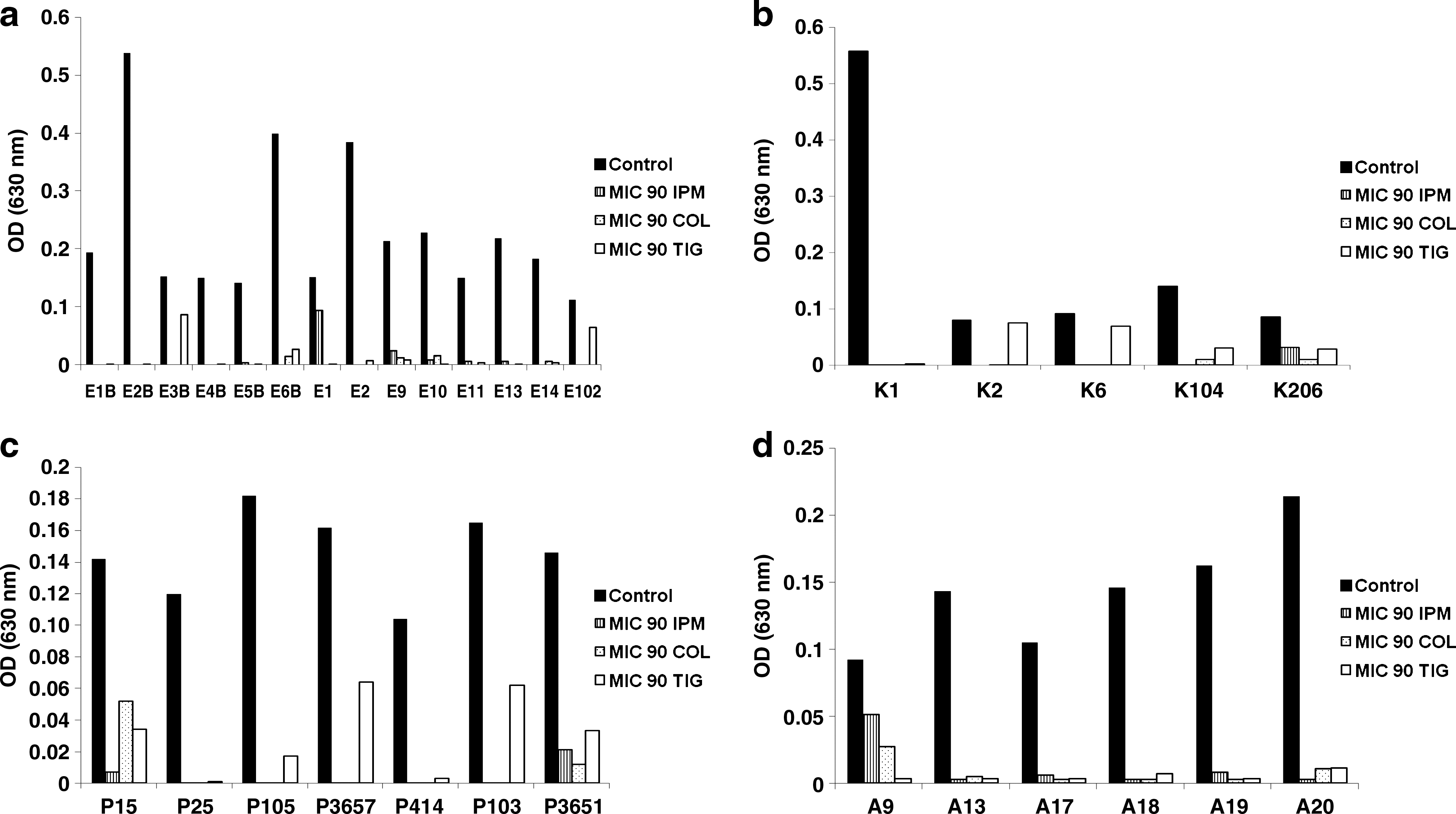
Effect of MIC90 of COL, IPM, and TIG on the biofilm formation by isolates of
Discussion
The rate of antimicrobial drug resistance among Enterobacteriaceae, Ps. Aeruginosa, and A. baumannii is increasing rapidly, thus limiting the armamentarium of potentially active antimicrobial agents.15,18 Although the re-evaluation of older agents is important, 16 there is a critical urge for the introduction of new antimicrobial agents to clinical settings to keep in pace with the development and spread of resistance mechanisms among Gram-negative bacteria. 36
The US FDA has approved the use of TIG, for complicated intra-abdominal and complicated skin and skin structure infections. 14 TIG enters bacterial cells through energy-dependent pathways and reversibly binds to the 30S subunit of the ribosome. It acts by blocking the incorporation of tRNA into the A site of the ribosome, thus inhibiting protein synthesis. 29
In Egypt, this agent has not yet been widely introduced to clinical settings. Therefore, the present study was designed to evaluate the in vitro activity of TIG against different Gram-negative isolates and to compare this activity to other potential antimicrobial agents available on the Egyptian market.
The overall activity of TIG against the tested isolates (n = 67) was comparable to that of IPM and COL with MIC90s of 8 μg/ml for the three antibiotics. The highest susceptibility rates were displayed by IPM and TIG. Nevertheless, the comparison of MIC average for both antibiotics revealed that TIG had an MIC average of 3.4 μg/ml, a value that is by far lower than that of IPM (MIC average was 16.9 μg/ml) (Table 2). Further, TIG showed a superior activity over LEV and PIP/TAZ and its MIC90 was lower by 8 and at least 64-fold when compared to MIC90s of LEV and PIP/TAZ, respectively. Several studies have reported TIG as a comparator for IPM against Enterobacteriaceae and A. baumannii in the treatment of complicated intra-abdominal and skin-structure infections.17,23,30 Other studies have considered polymixins and TIG to be the remaining effective therapy against E. coli, 22 K. pneumoniae, 4 and A. baumannii multiresistant isolates.8,34
The tested E. coli and K. pneumoniae isolates showed no resistance to TIG, which was the most active antimicrobial evaluated in this study against these microorganisms with an MIC50 of 1 μg/ml. The results reported by Souli et al. 33 were in accordance describing TIG as a very potent agent that inhibited 100% of E. coli and 97% of K. pneumoniae isolates they tested at a concentration of 2 μg/ml. Kelesidis et al. 15 reported a comparable TIG susceptibility rate (99.6%) for E. coli isolates according to the FDA criteria.
As expected, against Ps. aeruginosa, TIG was less active with MIC90 of 16 μg/ml, a value also reported by others 2 ; an even higher value of MIC90 reaching 32 μg/ml was obtained by Bradford et al. 3 In their study, Dean et al. 6 explained that Ps. aeruginosa carry inherently encoded resistance-nodulation-division efflux pumps conferring decreased susceptibility to TIG.
Against A. baumannii isolates, the MIC50 and MIC90 of TIG were 2 and 16 μg/ml, respectively, and the MIC range was 0.5–16 μg/ml. Navon-Venezia et al. 26 reported an MIC90 of TIG against A. baumannii of 32 μg/ml with a wider range of 1–128 μg/ml. In general, decreased susceptibility to TIG in Acinetobacter spp. might be associated with the overexpression of the AdeABC multidrug efflux pump, which confers resistance to various classes of antibiotics. 8
Findings were somewhat different using the interpretative MIC breakpoints of susceptibility of Enterobacteriaceae to TIG issued by the European Committee on Antimicrobial Susceptibility Testing (EUCAST) for K. pneumoniae where 21.4% of isolates would count as resistant with MIC of >2 μg/ml, whereas no difference in the percentage of resistance for E. coli isolates was observed using EUCAST breakpoints. Since EUCAST considers that to date there is insufficient evidence to establish TIG breakpoints for Acinetobacter and no breakpoints are available for Pseudomonas, the FDA-approved breakpoints for these microorganisms were used as published in previous studies.6,28
When dealing with an infection caused by IPM-resistant Gram-negative isolate, the remaining treatment option available for a clinician is the prescription of COL or TIG. 8 Therefore, a comparative bactericidal activity of TIG and COL against eight IPM-resistant isolates has been provided in this study through the kinetics approach. COL showed a rapid bactericidal activity after 3 hours with a re-growth after 24 hours at 1 × MIC for all tested isolates. Similarly, Owen et al. 27 reported an extreme rapid killing activity of COL with a significant re-growth after 24 hours even at concentrations of 32 × MIC or 64 × MIC for A. baumannii isolates. The re-growth could be attributed to the presence of COL heteroresistance, where the more resistant sub-populations have probably led to the substantial re-growth. 20 TIG showed a bactericidal activity at the higher concentrations after 6 hours of exposure against E. coli and K. pneumoniae isolates. Bratu et al. 4 demonstrated a bactericidal activity of TIG against 13% of the carbapenemase-producing K. pneumoniae isolates they tested. In contrast, TIG displayed only bacteriostasis against tested A. baumannii isolates, an effect also reported by Pachon-Ibanez et al. 28 Re-growth occurred after 24 hours at 1 × MIC of TIG with all isolates included in the study at hand, a phenomenon common with other tetracycline derivatives. 1
In human medicine it has been estimated that 60% of bacterial infections are biofilm associated and they are 10 to 1,000 times more resistant to the effects of antimicrobial agents. 19 Little is known about the ability of TIG to inhibit biofilm formation in Gram-negative isolates. Therefore, an experiment was designed to investigate the effect of TIG MIC90 on the biofilm formation by the isolates tested in this study and to compare it to that of IPM and COL (Fig. 1a–d). Different protocols have been proposed for the study of biofilm susceptibility due to the absence of a single standard method.9,19 One of these techniques include the use of automated confocal laser scanning microscopy to determine the antibiotic efficiency on bacterial biofilms 25 ; nevertheless, a simple method providing a fast quantitative measure of the mass of biofilm cells and described by Dobinsky et al. 7 is adopted in this study. TIG exerted its most biofilm-inhibiting ability against E. coli and A. baumannii isolates. On the other hand, IPM and COL almost prevented biofilm formation in the tested isolates. This is in accordance with findings reported by Hill et al. 10 stating that COL and meropenem, at a concentration of 32 μg/ml, were very effective agents inhibiting biofilm formation in Ps. aeruginosa isolates.
In conclusion, the uncontrolled spread of resistance in Gram-negative isolates, particularly among A. baumannii, Ps. aeruginosa, and K. pneumoniae isolates, presents a tremendous challenge to physicians trying to prescribe optimal therapy for infections caused by these pathogens. This challenge increases with high proportions of strains becoming more resistant to older commonly used antibiotics. To confront this challenge, the introduction and the use of new agents has become a major necessity. The results of the present study suggest that TIG is a promising antimicrobial agent that will most likely play a key role in the treatment of infections caused by strains for which adequate therapy has been limited.
Footnotes
Acknowledgments
We would like to profusely thank the staff of microbiology laboratory affiliated with El-Meery teaching hospital for their cooperation in the collection of isolates used in this study.
Disclosure Statement
No conflict of interest exists.