
Abstract
Vancomycin-resistant enterococci (VRE) are common nosocomial pathogens; however, until now they have been rarely encountered in Hungary. In the present study, we investigated the prevalence of VRE in the teaching hospitals of the University of Debrecen. Of 7,271 Enterococcus-containing clinical samples collected between 2004 and 2009, we identified 16 VRE. Species-specific polymerase chain reaction was used to detect Enterococcus faecalis, Enterococcus faecium, Enterococcus casseliflavus, and Enterococcus gallinarum. Multiplex polymerase chain reaction was performed to identify the vancomycin resistance genes: vanA, vanB, vanC1/C2, vanD, vanE, and vanG. Restriction digestion with SalI and HindIII was introduced to differentiate the vanC1 and vanC2 genes from each other. Genetic relationships between the strains were investigated by pulsed-field gel electrophoresis. Overall, we identified the vanC1 resistance gene in 14 E. gallinarum and the vanC2 resistance gene in two E. casseliflavus strains. Except for two samples, the isolates had different pulsed-field gel electrophoresis types, suggesting sporadic emergence of the resistant bacteria. In addition, antibiotic resistance profile was determined by E-test. Three E. gallinarum strains proved to be resistant to gentamicin because of the presence of the aacA-aphD gene. Although the prevalence of VRE in Debrecen is rather low, the appearance of multiple resistances is of concern.
Introduction
Materials and Methods
Bacterial strains
Clinical samples were analyzed by routine laboratory procedures. 12 Gram-positive, catalase-negative cocci were tested for growth on bile-esculin agar (Oxoid). Enterococci were further subcultured on brain heart infusion screen agar plates containing 6 mg/L vancomycin (Oxoid). The minimum inhibitory concentrations of vancomycin, teicoplanin, linezolid, ampicillin, tigecycline, daptomycin, gentamicin, and amoxicillin/clavulanate were determined by E-tests (AB Biodisk). The results were interpreted according to EUCAST breakpoints 11 except for daptomycin, which was evaluated according to CLSI. 5
Polymerase chain reaction
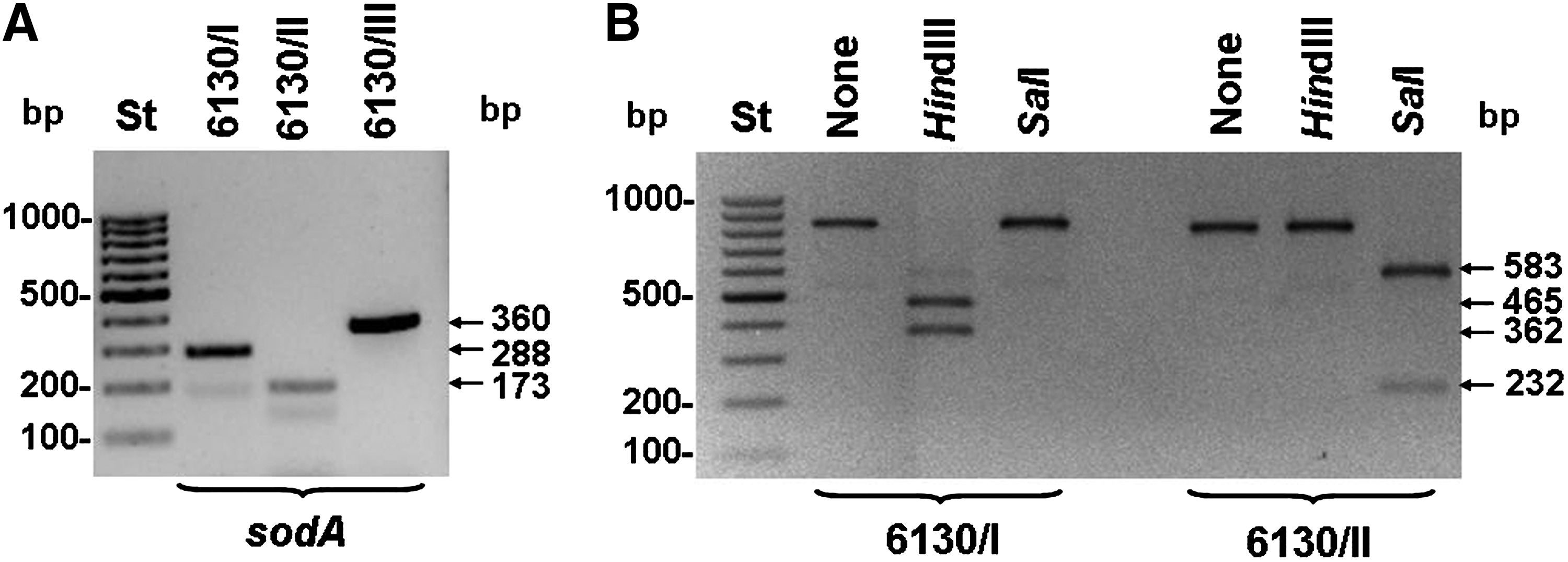
Cell lysates were prepared by boiling cultured bacteria pellets in DNase-free water for 10 minutes. 27 Multiplex polymerase chain reaction (PCR) was performed with the primer pairs specific for the vancomycin resistance genes: vanA, vanB, vanC1/C2, vanD, vane, and vanG as well as the E. faecalis and E. faecium D-alanine:D-alanine ligase (ddl) genes for species identification. 7 In addition, E. faecalis, Enterococcus casseliflavus, and Enterococcus gallinarum species were identified using superoxide dismutase (sodA) gene-specific primers.7,15 High-level gentamicin resistance was confirmed by PCR 27 with the modified aacA-aphD primer pair (acph-F: GATTTGCCAGAACATGAATTACAC and acph-R: ATCATAACCACTACCGATTATTTC).
Restriction fragment length polymorphism
To differentiate the vanC1 and vanC2 genes from each other, samples producing amplicons of 815 or 827 bp (vanC1 or vanC2) in the multiplex setup were further investigated by a separate PCR performed with vanC1/C2-specific primers followed by restriction analysis with 2 U of SalI or HindIII at 37°C for 2 hours. The vanC1 PCR product was specifically cleaved by SalI, whereas HindIII cut only the vanC2 PCR product (Fig. 1B). DNA sequencing confirmed the validity of our restriction fragment length polymorphism approach (Table 1).
Identification of enterococci in clinical sample No. 6130.
Confirmed by DNA sequencing.
DNA sequencing and multilocus sequence typing
Multilocus sequence typing of one E. faecalis species was performed by sequencing internal gene fragments for seven housekeeping genes (gdh, gyd, pstS, gki, aroE, xpt, yiqL) according to Aanensen and Spratt. 1 Each gene was amplified with Pfu DNA polymerase. PCR products were purified either with the Microcon Ultracell YM-100 column (Amicon) or with the Wizard SV Gel and PCR Clean-up System (Promega) and were sequenced on both strands. Gene identification was done by the blastn algorithm, 2 and DNA sequences were compared with ClustalW2. 4
Pulsed-field gel electrophoresis
Pulsed-field gel electrophoresis (PFGE) was performed as previously described for Staphylococcus aureus, 23 with the following modifications: The bacteria were resuspended in 300 μl of cell suspension buffer (1 M NaCl and 10 mM Tris [pH 8.0]) and the plugs were incubated at 37°C for 3 hours in 3 ml of EC lysis buffer, containing 25 U mutanolysin, 0.5 mg/ml lysozyme, and 166 μg/ml of RNase A. The second incubation was at 54°C for 19–20 hours in 3 ml ES buffer (0.5 M EDTA and 1% N-lauroyl sarcosine) containing 133.3 μg/ml proteinase K. Each plug was digested with 15 U of SmaI (Promega) for 4 hours at 25°C. PFGE profiles were analyzed with the BioNumerics program version 2.5 (Applied Maths BVBA) using the UPGMA/Dice coefficient with 2% optimization and 2% band position tolerance.
Results
In a 6-year period from 2004 to 2009, our diagnostic laboratory isolated overall 7,271 enterococci from clinical samples and 16 of them grew on VRE screening plates. According to the multiplex PCR, only one isolate harbored the vanA gene, which was previously published. 8 In addition, 15 clinical samples contained the vanC resistance gene. The distribution of enterococcal isolates by sample number, year of isolation, specimen type, species, and the detected resistance genes are presented in Table 1. Initially, we confirmed the vanC genes by DNA sequencing (Table 1). The sequences of 815 or 827 nucleotides turned out to be identical to the corresponding segments of the published vanC1 or vanC2/3 genes of E. gallinarum and E. casseliflavus (GenBank accession numbers: EU151772 and EU151764, respectively). Later on, we differentiated the two genes with a new method based on restriction analysis. Instead of MspI, which cleaves both vanC1 and vanC2 PCR fragments, 17 we introduced two specific restriction enzymes SalI and HindIII. With this method we found one clinical sample (No. 6130) that was affected by both enzymes, suggesting the presence of both vanC1 and vanC2. By spreading the original clinical sample and picking single colonies, we separated three subcultures. According to the sodA-specific PCR, we identified them as E. casseliflavus (No. 6130/I), E. gallinarum (No. 6130/II), and E. faecalis (No. 6130/III) (Fig. 1A). As it is unusual that one patient can be affected with three Enterococcus species at the same time, we investigated this case in detail. In a subsequent screening with 6 mg/L vancomycin-containing agar plates, only the E. casseliflavus and E. gallinarum strains proved to be VRE. The restriction analysis revealed that isolate 6130/I contained the vanC2 and isolate 6130/II harbored the vanC1 resistance gene (Fig. 1B). The accompanying vancomycin-susceptible E. faecalis was genotyped by multilocus sequence typing. It represented a novel ST, because by sequencing the acetyl-CoA acetyltransferase (yiqL) gene we found a single-nucleotide replacement of C to T at position 187 when compared with allele yiqL-8. The new allele and sequence type were termed yqiL-64 and ST-336, respectively. 1 We found 1 more vanC2-carrying E. casseliflavus and 13 vanC1-carrying E. gallinarum strains (Table 1). To determine the genetic relatedness of the resistant strains, we performed PFGE (Fig. 2). PFGE patterns were analyzed according to Tenover et al. 24 Two E. gallinarum isolates (Nos. 8043 and 3834) were found to have indistinguishable genotypes, and six formed one cluster with >90% identity. The rest of the E. gallinarum were genetically unrelated and the E. casseliflavus strains also had no genetic relationships (Fig. 2). The resistance of the 16 vanC-positive isolates was tested against the following panel of antibiotics: linezolid, ampicillin, tigecycline, daptomycin, gentamicin, and amoxicillin/clavulanate. Beside the vancomycin resistance, three E. gallinarum were also highly resistant to gentamicin. The bifunctional aminoglycoside resistance gene (aacA-aphD) was identified by PCR in the latter samples (Table 1).
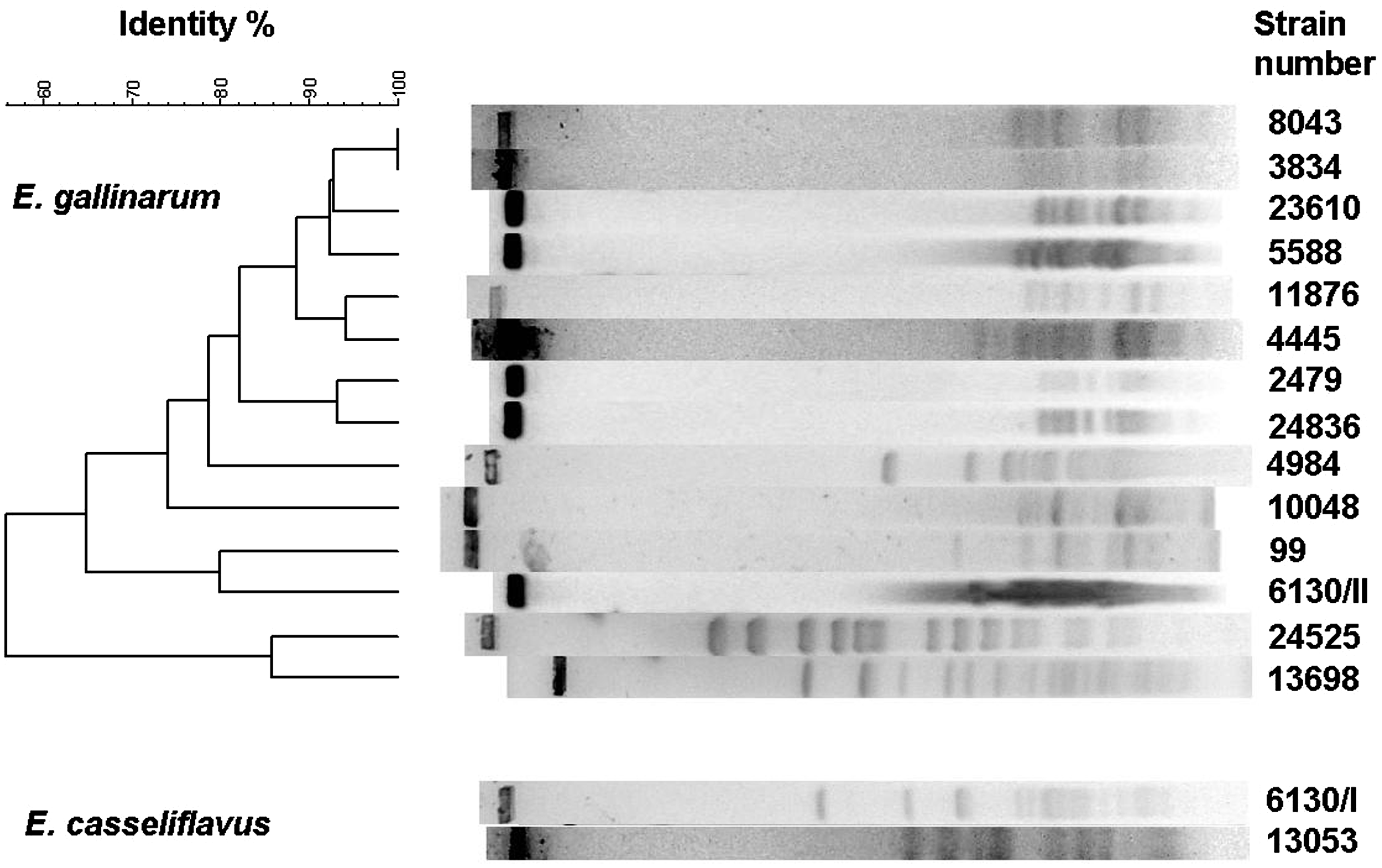
Pulsed-field gel electrophoresis analysis of vancomycin-resistant enterococci strains. VanC1-containing E. gallinarum and vanC2-containing E. casseliflavus were tested separately. The dendrogram was constructed with the BioNumerics program; the software normalized the positions of the lanes to get a correct comparison.
Discussion
Serious VRE infections occur usually in patients with compromised immune defense. This condition underlines the importance of effective antimicrobial treatment. Rapid detection of resistant phenotypes is essential for adequate empirical therapy and controlling transmission. 20 For susceptibility testing, the most appropriate method is the E-test, which requires 24 hours of incubation. Although, the VITEK 2 system provides susceptibility results in approximately 8 hours, its 3.01 software version is not always suitable to identify low-level glycopeptide resistance in Enterococcus strains. 9 Therefore, the best method for the rapid detection of vancomycin resistance is the identification of van genes by PCR.
In the clinical practice, the molecular characterization of resistance genes focuses on the identification of vanA and vanB, because these strains have higher levels of resistance to vancomycin. The vanA and vanB operons are located on mobile genetic elements, which allow resistance to spread clonally and laterally; therefore, they are of special epidemic concern. In contrast, vanC-type strains encode low-level resistance and the gene is located in the bacterial chromosome. 26 Although the vanC genotype is somewhat neglected, vanC-carrying enterococci can cause just as much serious clinical infections as any other VRE. 18 Inadequate empirical use of vancomycin in these cases can result in therapeutic failure, prolonged hospitalization, and increased costs of medical care.
In agreement with earlier European data, 14 our study demonstrates that the prevalence of vanC1 was higher than vanC2 in Debrecen, Hungary. A similar ratio between the two genes was found earlier in an American study. 19 Multiple infections caused by different resistant Enterococcus species are of special interest, because most of these cases remain unrecognized in conventional routine laboratory testing. The molecular investigation of one clinical sample revealed that one of our patients was affected by three different kinds of enterococci, two of which were VRE. Three other patients were infected by vancomycin-resistant E. gallinarum, which were also highly resistant to gentamicin. These strains carried the aacA-aphD in addition to the vanC1 resistance gene. As the three strains were genetically unrelated by PFGE, it is likely that they acquired double antibiotic resistance independently. The PFGE profiles also support the hypothesis that most of the VRE strains appeared sporadically. Only two E. gallinarum strains isolated in 2009 had identical PFGE profiles. Both samples (Nos. 3834 and 8043) were collected from the surgery departments of the hospital, but the patients were treated in different wards and in different time periods, and thus a direct contact between them can be excluded. Fortunately, the incidence of vanC-harboring enterococci is rather low (0.22%) in Debrecen, Hungary, and multiple resistance was encountered only in a few cases (0.04%). Susceptibility testing identified several antibiotics that were effective, allowing the successful treatment of the patients.
Footnotes
Acknowledgments
The authors are grateful to the staff of the Bacteriological Diagnostic Laboratory, University of Debrecen, Hungary, for the isolation of enterococci from clinical samples. The authors thank Dr. József Kónya (Department of Medical Microbiology, University of Debrecen, Debrecen, Hungary) for his valuable suggestions during the preparation of the manuscript. The present study was supported by a Postgraduate Research Grant of the University of Debrecen, Hungary.
Disclosure Statement
No competing financial interests exist.