
Abstract
This report describes two subsequent liver-small bowel-pancreas-kidney (multivisceral) transplantations in a child colonized with multidrug-resistant Pseudomonas aeruginosa. We discuss the dilemma concerning the transplantation of patients colonized with multidrug-resistant Pseudomonas spp., its potential consequences, and the peri and postoperative management of these patients.
Introduction
Case Report
A 4-year-old female with short-bowel syndrome secondary to intestinal aganglionosis, TPN-induced liver failure, and renal failure due to renal dysplasia underwent a liver-small bowel-pancreas-kidney transplant with postoperative prophylaxis consisting of fluconazole and piperacillin tazobactam (TZP) as per hospital protocol. Her sputum was colonized before transplantation with P. aeruginosa (isolate 1). The clinical course, pertinent cultures, and antibiotic treatments are summarized in Fig. 1; note that P. aeruginosa isolates are defined as those having unique antibiotic susceptibility phenotypes. She required reinterventions for hematoma evacuation and washout and peritoneal cultures grew P. aeruginosa (isolate 1). Repeat washout grew two isolates of P. aeruginosa (isolates 1 and 2). On repeated exploratory laparotomy and repair of the gastro-jejunostomy perforation, P. aeruginosa persistently grew in the culture (isolate 2). She was subsequently started on IMP. The patient required another repair of the anastomotic leak and the peritoneal culture grew P. aeruginosa (isolate2). She underwent two more surgical procedures with repair of the perforations. After 19 days on IMP, the treatment was changed to daptomycin (DAP) and TZP for abdominal cellulitis and possible peritonitis. At the same time, after prolonged mechanical ventilator support, she was diagnosed with ventilator-associated pneumonia with P. aeruginosa (isolate 3), and was treated with CST. She developed P. aeruginosa bacteremia (isolate 3*) and she was treated with CIP. The line was removed; bacteremia initially cleared but reoccurred after 8 days. The subsequent P. aeruginosa isolate became CST intermediate and CIP resistant (isolate 4); she was treated with CST and TOB with minimal increase in creatinine. Three weeks later she again developed P. aeruginosa bacteremia (isolate 5); she was initially treated with 3 days MEM and TOB, but she completed the treatment with CIP and TZP. To optimize the pharmacokinetics-pharmacodynamics of carbapenems and TZP, we extended each infusion over 3 hours to maximize free time >minimum inhibitory concentration (MIC).
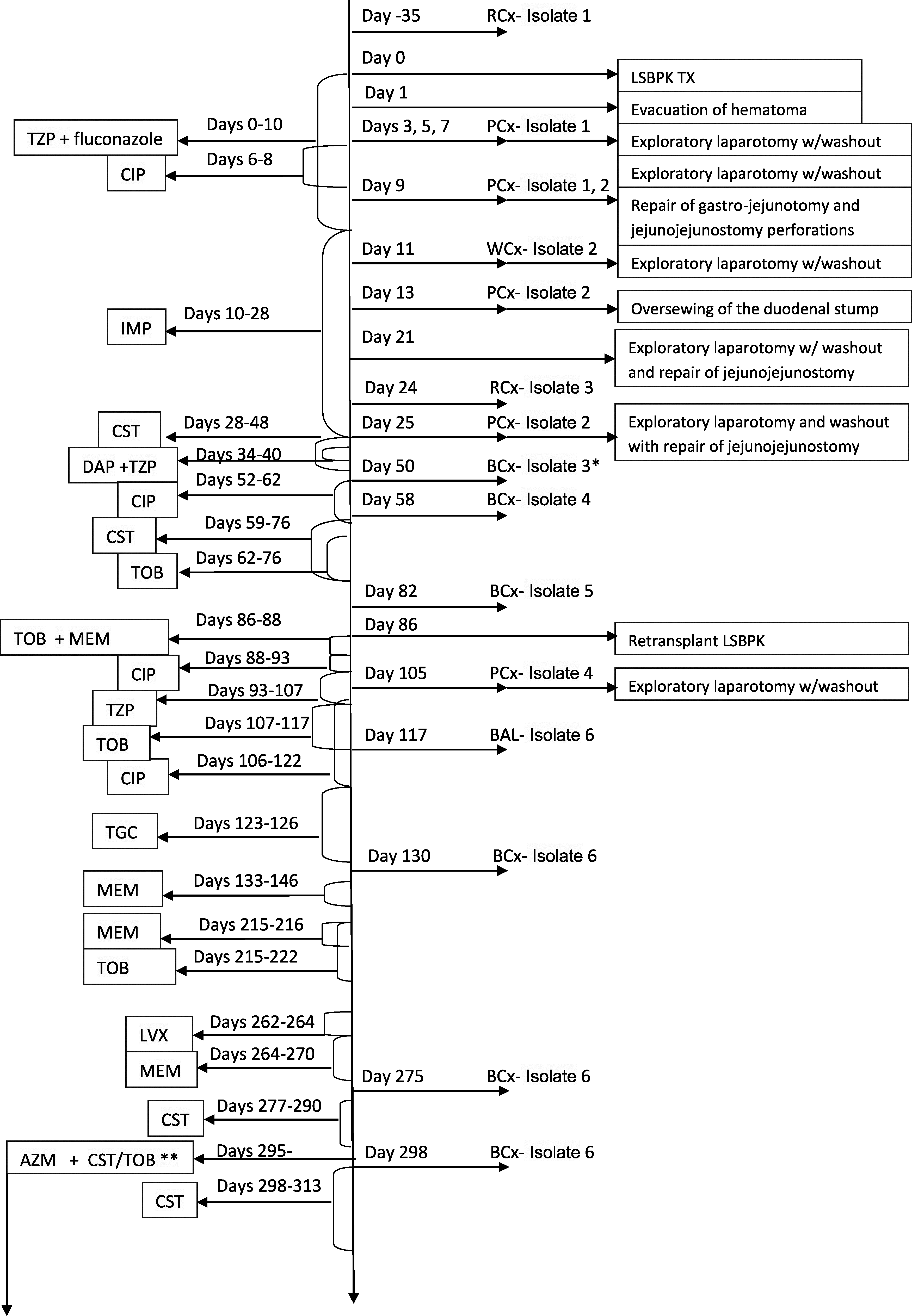
Diagram of the clinical course, relevant cultures, and antibiotic treatment for our patient.
She developed severe rejection of the small bowel allograft and renal failure requiring a second combined liver-small bowel-pancreas-kidney transplant 3 months after the first transplant. The patient received TZP for perioperative prophylaxis after completing treatment for bacteremia. After second transplant she developed peritonitis with P. aeruginosa (isolate 4), while she was on TZP prophylaxis, and was treated with TOB and CIP. Four weeks later, while she was being treated with tigecycline for polymicrobial ventilator acquired pneumonia, she developed P. aeruginosa bacteremia (isolate 6) and was subsequently treated with MEM. She slowly improved and was discharged to her parents' care.
She has been readmitted several times during the following 3 months for P. aeruginosa bronchitis and every time responded to a short course of antibiotics (MEM, levofloxacin, TOB). Six months after the second transplant she was readmitted with fever and increased oxygen requirements. A computer tomography of the chest showed multiple bilateral pulmonary nodules, patchy pulmonary consolidations, and bilateral hilar lymphadenopathy (Fig. 2). Sputum culture was positive for P. aeruginosa (isolate 6). She was started on voriconazole, MEM, and TOB. Patient was found to have inguinal lymphadenopathy; biopsy of the lymph node was performed and histology was negative for post-transplant lymphoproliferative disorder; special stains were negative for fungal elements. Histoplasma capsulatum urine antigen, Cryptococcus neoformans blood antigen, and Aspergillus galactomannan antigen were negative. Bronchoalveolar lavage was performed after a few days of antibiotics and all the cultures were negative. The blood cultures became positive for P. aeruginosa (isolate 6) and she was discharged on CST. One week after discontinuation of therapy, she was readmitted for fever and was again bacteremic with P. aeruginosa (isolate 6). Repeat computer tomography of the chest showed increasing confluence of the pulmonary opacities (Fig. 3). She received a 3 week-course of intravenous CST with resolution of the pulmonary infiltrates. Since the most likely source of recurrent infections was the lung she was started on monthly alternating nebulized treatment with TOB and CST and daily oral azithromycin for anti-inflammatory properties. With this antibiotic regimen she did not have any pulmonary exacerbation or episodes of P. aeruginosa bacteremia in the following 6 months.
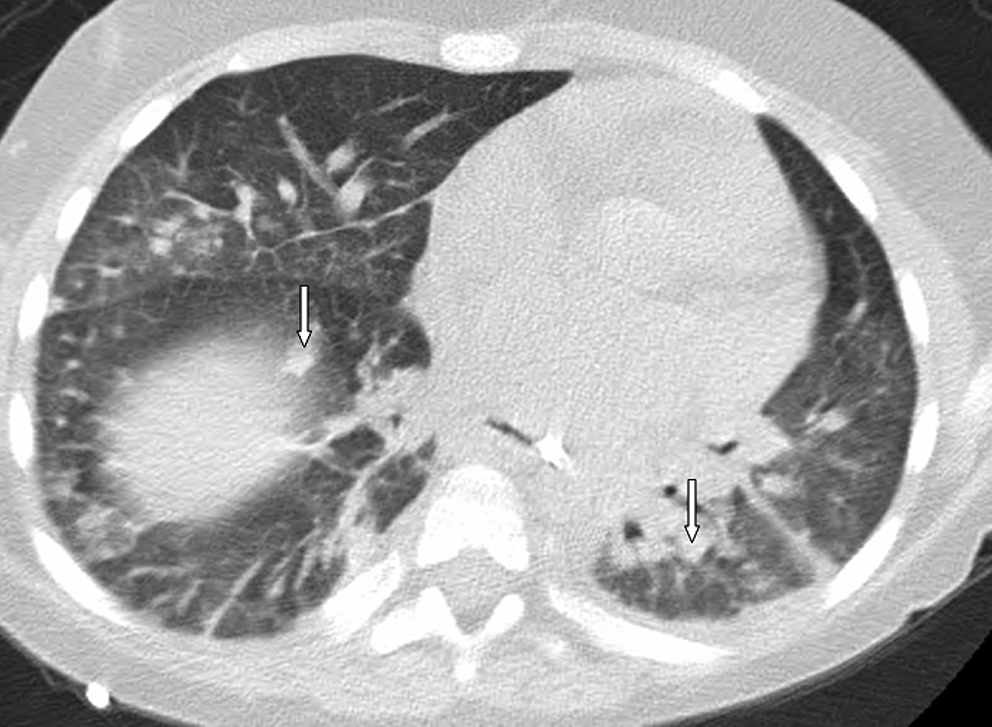
Computer tomography of the chest without contrast showing bilateral pulmonary nodules (arrows). Courtesy of Dr. David Poage.

Follow-up computer tomography of the chest without contrast showing increased patchy multifocal consolidation, with nodular appearance (arrows). Courtesy of Dr. David Poage.
Discussion
Many transplant recipients have multiple infections (pneumonia, intra-abdominal, and line infections) before transplantation and have been exposed to various courses of antibiotics, promoting colonization with MDR bacteria and subsequent infections with these organisms. MDR P. aeruginosa colonizing the bowel can persist for a prolonged time, even after the removal of the selecting antibiotic agent and can be rapidly reselected under antibiotic pressure. 14
Optimal treatment of MDR Pseudomonas spp. systemic infections is not well defined; it may include one antibiotic or combination of antibiotics. Also the use of certain antibiotics to treat these infections might be limited by nephrotoxicity, especially post-transplant when renal failure is not uncommon in patients already receiving other nephrotoxic drugs. Carbapenems have been considered the drugs of choice for the treatment of Pseudomonas spp. infections, but carbapenem resistance is becoming a therapeutic problem worldwide.15,20 Extended infusion strategies for carbapenems, penicillins, and cephalosporins should be considered for patients with serious Gram-negative infections, MDR infections, to optimize pharmacokinetic-pharmacodynamic parameters, especially in children who have increased drug clearance compared with adults. In the absence of new antibiotics to treat MDR Pseudomonas spp., CST or a combination of antibiotics could be a viable option.6,7,13,22 Clinical isolates of P. aeruginosa with reduced susceptibility to the polymyxin B and CST have been previously reported.3,7,8,18 With the emergence of polymyxin B resistant MDR P. aeruginosa isolates, clinicians might need to consider combination therapy to achieve a favorable clinical outcome. What should we do when the bacteria is resistant or intermediate susceptible to our last line of therapy, CST? Various antibiotic combinations (i.e., β-lactams-fluoroquinolones, MEM-CIP, MEM-CST, IMP-polymyxin B, polymyxin B-rifampin) might have synergistic or additive activity as previously demonstrated by time-killing experiments.6,7,13,22 However, despite synergistic or additive effect in vitro of these combinations, the clinical significance is not defined and definitive recommendation cannot be made. For our patient, we administered IMP, MEM, and TZP as extended infusion to maximize fT>MIC. We also used different antibiotic combinations (CST-TZP, CST-TOB, MEM-TOB, CIP-TOB) with the hope we might achieve synergistic activity. In our case, resistance to CIP emerged, possible due to increased expression of efflux pumps or mutations in either parC or gyrA. 2 Emergence of carbapenem resistance could be explained by a combination of increased expression of multidrug efflux pumps, AmpC derepression, and mutation of the membrane porins. 16
Our patient was started on azithromycin because of its known properties to modulate inflammatory pathways by interfering with neutrophils recruitment, chemotaxis, and oxidative burst12,17,19 and to downregulate pro-inflammatory cytokines production.12,24 Even more, azithromycin inhibits a key enzyme in the biofilm synthesis pathway, 10 modulates the production of bacterial virulence factors, 11 inhibits the bacterial protein synthesis, 23 and interacts with the outer membrane of the bacteria. 5 We also alternated administration of aerosolized CST and TOB since most of the infections originated from the lung, with the goal to decrease the frequency of infections and hospitalization. Since CST and TOB are concentration-dependent drugs, we chose them as maintenance aerosolized therapy to maximize the antibacterial effects and prevent recurrent infections.
In conclusion, is multivisceral transplantation contraindicated in patients colonized with MDR Pseudomonas? Based on our experience, if patients still have one or two alternative antibiotics that can be used to treat the infection, transplantation should not be contraindicated. The decision to transplant such a patient should also be individualized based on the presence of other comorbidities, patient's response to antibiotics, the type of procedures to be performed, and the ability of the recipient to tolerate the available therapeutic agents, especially if they would be used in combination. Targeted prophylaxis with antibiotics to cover the MDR Pseudomonas spp. or combination of antibiotics that proved efficient for the MDR organism in a specific situation should be perioperatively administered. Several treatment options should be considered in patients infected with MDR Pseudomonas spp.: use of CST, maximize pharmacokinetic-pharmacodynamic parameters of antibiotics and use of combination of antibiotics. Strict isolation precautions should be reinforced to avoid spreading of the multiresistant bacteria.
Footnotes
Acknowledgment
The authors thank Mrs. Ashley Calhoon for the preparation of the manuscript.
Disclosure Statement
The authors of this manuscript have no conflicts of interest to disclose.