
Abstract
The objectives of this study were to investigate antibiotic resistance in urinary pathogens from Korean patients with uncomplicated acute pyelonephritis (UAPN), and to determine the effect of fluoroquinolone (FQ) resistance on clinical outcome in those patients with UAPN initially treated with FQ. Clinical and microbiologic data for all the APN patients attending 14 hospitals in South Korea in 2008 were collected retrospectively. Urinary pathogens were identified in 719 cases, and Escherichia coli was the most common pathogen (661/719, 91.9%). Antibiotic susceptibilities to several E. coli antibiotics were as follows: ciprofloxacin, 84.1%; trimethoprim-sulfamethoxazola (TMP-SMX), 67.2%; and extended-spectrum beta-lactamase-negative, 92.4%. FQ was the most frequent antibiotic prescribed for UAPN (45.3% intravenously and 53.9% by mouth). We compared clinical outcomes and hospital days in patients with FQ-resistant (32) and FQ-sensitive E. coli (173) who received FQ as initial empirical therapy. Clinical cure was higher in the FQ-sensitive group (78% vs. 91%, p=0.027), and hospital days were longer in the FQ-resistant group (9.6±5.5 days vs. 7±3.5 days, p=0.001). In conclusion, FQ-sensitivity of E. coli from UAPN was 84.1%. FQ treatment of UAPN caused by FQ-resistant E. coli has a lower cure rate and involves longer hospital stay than FQ treatment of cases caused by FQ-sensitive E. coli.
Introduction
Current Infectious Disease Society of America guidelines for treatment of UAPN without knowledge of microbiologic data or susceptibility profiles recommend oral or intravenous fluoroquinolones (FQ), such as ciprofloxacin (CIP), if the resistance of community uropathogens to FQ is <10%. 4 Unfortunately, there has been a recent trend of increasing resistance to FQ among uropathogens in many countries. The CIP resistance rate of Escherichia coli from urine in the outpatient clinic of Denver Health in the United States increased from 1% in 1998 to 9% in 2005 with the wide use of levofloxacin (LEV). 6 In Portugal and Spain, the CIP resistance rates of E. coli in community-acquired acute uncomplicated UTI were found to be 5.8% and 14.7%, respectively. 7 A report from Korea showed that the rate of resistance to CIP was 23.4% among E. coli strains, causing acute uncomplicated cystitis in female outpatients. 8
In UTI, the disappearance of bacteriuria is closely correlated with sensitivity of the microorganisms to the concentrations of the antimicrobial agent achieved in the urine rather than in the blood, 13 which suggests that it is important to examine the clinical impact of antimicrobial resistance on treatment outcomes in UTI. Small trials of women with UTI treated with trimethoprim-sulfamethoxazole (SXT) have shown that approximately 50% had bacteriological failure, and 40% had clinical failure, if the causative pathogen was resistant in vitro.10,11 Since CIP is abundantly excreted in the urine and usually has a concentration of 100–300 mg/L, which far exceeds the minimal inhibitory concentration (MIC; 4 mg/L) for CIP-resistant E. coli, 2 a study looking at the clinical relevance of in vitro CIP resistance in UTIs appeared desirable.
Thus, our aims in this study were twofold. The first aim was to identify the etiologic agents of UAPN and their antibiotic susceptibility profile in Korea. The second was to determine the effect of CIP resistance on clinical outcome in patients with UAPN treated with CIP or LEV.
Patients and Methods
Setting and study design
This was a retrospective cohort study of UAPN patients in South Korea, to assess the antimicrobial susceptibility of uropathogens and the clinical outcomes for patients with antibiotic-resistant bacteria. The study was conducted through the cooperation of 14 hospitals with 32 to 1,552 beds (13 hospitals >500 beds) in South Korea in 2008. The hospitals that participated in the study were: St. Vincent Hospital, Gachen University Gill Hospital, Aju University Hospital, Jeju University Hospital, Gangbuk Samsung Hospital, Gangdong Sumshing Hospital, Daegu Fatima Hospital, Dong-A University Hospital, Korea University Kuro Hospital, Daejon University Hyehwa Hospital, Korea University Ansan Hospital, Gyemyeong University Hospital, Inha University Hospital, and Hanyang University Hospital.
Patient population
All the patients who visited the participating hospitals between January 1, 2008 and December 31, 2008 who had a discharge diagnosis of acute pyelonephritis were enrolled in the study. Patients with a diagnosis of acute pyelonephritis for more than 48 hours after admission were excluded, as these were thought to be healthcare-associated infections. To select for patients with UAPN, we excluded all patients who had complicated pyelonephritis, namely patients with either systemic underlying disorders or urologic conditions complicating the infection. Systemic conditions were: cerebrovascular disease, kidney transplantation, diabetes mellitus, liver disease, renal disease, malignancy, pregnancy, and immunosuppression. Urologic conditions were benign prostatic hyperplasia, neurogenic bladder, urolithiasis, hydronephrosis, polycystic kidney, indwelling urinary catheters, and intermittent catheterization.
Data collection
Medical records of all eligible patients were retrospectively reviewed. Information from follow-up visits was used whenever available. Data gathered on the patients included demographic data, history of previous UTIs during the previous 1 year, antibiotic usage in the current episode before visiting the hospital, treatment regimens in hospital, reason for switching antibiotics as either no response on the day of antibiotic switch or availability of antimicrobial susceptibility report, days to defervescence, days of hospital stay, and clinical cure versus failure.
Clinical cure was defined as absence of symptoms or signs at completion of therapy and/or at 4–10-day follow-up, when available. Clinical treatment failure was defined as recurrence of symptoms at 4–10 days' follow-up after treatment, or constancy of, or deterioration in, any of the clinical parameters at 3 days after initiation of therapy.
Microbiologic data
Urine and blood cultures were processed in the routine laboratory. Etiologic agents were determined when ≥105 CFU/ml of organisms were identified on urine culture,14,15 and/or isolation of urinary pathogens from blood culture. Species identification and susceptibilities to antimicrobial agents were determined by means of either a semiautomated system (VITEK, bioMerieux, Hazelwood, Mo. or Microscan, DADE Behring, West Sacramento, CA) or disk diffusion susceptibility tests according to the criteria of the Clinical and Laboratory Standard Institute (CLSI). 1
Statistical methods
SPSS version 19.0 for Windows (SPSS, Inc., Chicago, IL) was used for statistical analysis. Categorical variables were analyzed by chi-square test or Fisher's exact test. Continuous variables were analyzed by independent t-test or Mann–Whitney test. Logistic regression analysis was performed to evaluate the effects of independent variables on clinical outcome. A p-value of <0.05 by the two-tailed test was considered statistically significant.
Results
Patient characteristics
During the study period, 2,502 patients with a final diagnosis of acute pyelonephritis were identified. Of these, 1,237 were excluded because of underlying systemic or urologic conditions that defined them as having complicated pyelonephritis. Of the 1,265 patients with UAPN, 719 cases gave positive results in either urine and/or blood culture, and they were included in the analysis. The number of cases per hospital ranged from 1.4% (10/719) to 15.7% (113/719).
The mean age was 50.6 years. 98.3% (707/719) of the patients were women. 18.3% (127/694) of the patients had been prescribed antibiotics before their hospital visit. History of UTIs within 1 year before admission was present in 28.2% (184/652) of the patients.
Microbiologic data
Of the 1,265 patients enrolled in the study, 16 did not have any cultures done and 527 had negative culture results. Seven hundred nineteen patients (56.8%) had positive culture results, and 211 of them (29.3%) also had positive blood cultures. Table 1 shows the etiologic agents of the acute pyelonephritis in our study population. E. coli was overwhelmingly the most common pathogen (661/719, 91.9%). Klebsiella pneumoniae (15/719, 2.1%), Streptococcus species (7/719, 1.0%), and Enterococcus species (11/719, 1.6%) were also identified.
The antimicrobial susceptibility profiles of the 660 E. coli isolates are displayed in Table 2. The number of isolates tested for susceptibility per antimicrobial agent ranged from 397 (extended-spectrum beta-lactamase [ESBL]) to 660, because each hospital altered the antimicrobial susceptibility panel for Gram-negative urinary pathogens from that specified in the CLSI guidelines 1 and the ESBL test was performed in hospitals using a semi-automatic system for antimicrobial susceptibility. Susceptibilities of the E. coli for various antibiotics were as follows: CIP, 84.1%; SXT, 67.2%; ceftriaxone (CRO), 95.4%; ceftazidine (CAZ), 94.2%; and ESBL-negative, 92.4%. Sixty-nine of 649 E. coli (10.6%) isolates were resistant to both CIP and SXT, and 4.3% (16/397) were resistant to CIP, SXT, and extended-spectrum cephalosporins. The antimicrobial susceptibilities of the E. coli from urine and blood had similar values for most antibiotics (CIP, 84% vs. 85%: CRO, 93.8% vs. 94.9%: CAZ, 93.8% vs. 92.6%: ESBL, 92.4% vs. 91.1%, respectively). However, their susceptibilities to SXT, tobramycin (TOB), and ampicillin (AMP) differed by >5% (SXT, 66% vs. 72.2%: TOB, 78.6% vs. 73%: AMP, 34.4% vs. 40.5%, respectively). There was no statistically significant difference in antibiotic susceptibility according to age or previous history of UTI (data not shown).
The number of isolates tested for susceptibility of each antimicrobial agent ranged from 397 (ESBL) to 660, because each hospital modified antimicrobial susceptibility panel for Gram-negative urinary pathogens from CLSI guideline1 and ESBL test was not performed in hospitals that used the disk diffusion test for antimicrobial susceptibility.
AMK, amikacin; AMP, ampicillin; ATM, aztreonam; CAZ, ceftazidime; CEF, cephalothin; CIP, ciprofloxacin; CRO, ceftriaxone; ESBL, extended-spectrum β-lactamase; FEP, cefepime; GEN, gentamicin; SAM, ampicillin/sulbactam; SXT, trimethoprim/sulfamethoxazole; TOB, tobramycin; TZP, piperacillin/tazobactam.
Antibiotic usage
Intravenous antibiotics were used in 696 of the 719 patients, and oral antibiotics were used in 657 patients. CIP was the most commonly used antibiotic by both the intravenous (45.3%) and oral (53.9%) route. Third-generation cephalosporins and aminoglycosides were the next most commonly used antibiotics. For oral antibiotics, β-lactam and SXT were used in 257 (39.1%) and 52 cases (7.9%), respectively. LEV was used in 0.8% of intravenous antibiotics and 6.0% of oral antibiotics, respectively. In 719 patients, IV antibiotics were used for 5.29±3.01 days, and oral antibiotics were used for 9.21±7.49 days.
Clinical characteristics and treatment outcomes of CIP-resistant E. coli
A total of 661 patients was found to have E. coli as the cause of the pyelonephritis. Of these patients, 244 were treated initially with CIP or LEV. Clinical outcome is known for 205 patients. Thirty-two patients had CIP-resistant E. coli UTIs, while 173 patients had CIP-sensitive E. coli UTIs (Fig. 1). Table 3 shows the demographic data of the two groups. There were no significant differences in age, previous history of UTI, antibiotic usage before hospital visit, fever duration before hospital visit, and presence of bacteremia.
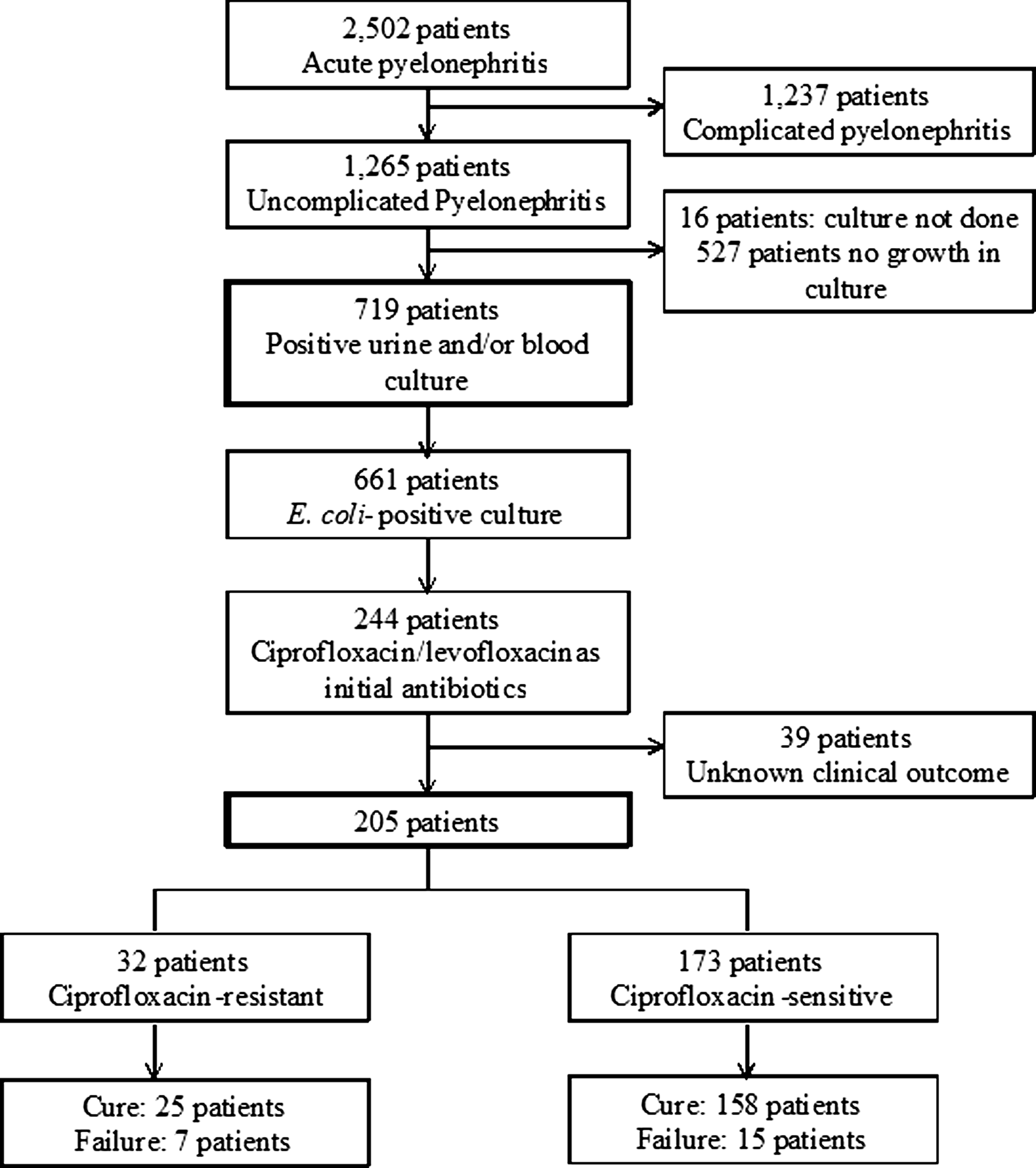
Consort diagram (total uncomplicated acute pyelonephritis retrospective cohort). Thirty-nine patients with unknown clinical outcome missed their follow-up visit after discharge.
Data are shown as N (%) or mean±standard deviation as appropriate.
By Mann–Whitney U test.
By Pearson Chi-square test or Fisher's exact test.
UTI, urinary tract infection.
We compared clinical outcomes in the two groups (Table 3). The CIP-resistant (CIP-R) group was found to have a worse outcome (clinical cure: CIP-R group 7/32 (78%) vs. CIP-susceptible [CIP-S] 158/173 (91%), p-value=0.027). No mortality occurred in either group.
The duration of IV antibiotics was 5.0±2.9 days in the CIP-R group and 5.1±2.7 days in the CIP-S group, and durations of oral antibiotic use were 9.3±7.7 and 8.3±4.5 days, respectively. Total duration of antibiotic treatment did not differ in the two groups (14.3±8.3 days in the CIP-R group and 13.5±5.3 days in the CIP-S group; p=0.72). Eighteen of the 32 patients in the CIP-R group (56%) and 20 of the 173 patients in the CIP-S group (12%) had their intravenous antibiotics changed during treatment. Mean days to change of antibiotic were 6.5 days (1–15 days) in the CIP-R group and 4.6 days (2–12 days) in the CIP-S group. Fourteen and 153, respectively, of the patients in the two groups were treated with CIP or LEV without antibiotic change. There was no statistically significant difference between the clinical outcomes of the subgroups of patients treated with CIP or LEV without antibiotic change in the CIP-R and CIP-S groups (12/14 [85.7%] in the CIP-R group, 147/153 (96%) in the CIP-S group, p=0.137).
Ten of the 32 CIP-R patients (31.3%) and 51 of the 173 CIP-S patients (29.5%) developed bacteremia on the day of admission. Three of the 10 CIP-R patients (30%) and 3 of 51 (5.9%) CIP-S patients in each group failed to give a clinical response after 3 days of treatment (p=0.050).
Days to defervescence showed a trend toward longer periods of fever in the resistant group (4.1±3.0 vs. 3.2±1.7, p-value=0.280). Days to defervescence were distributed differently in the two groups (Fig. 2). Duration of hospital stay was significantly longer in the patients with resistant bacteria (9.6±5.5 vs. 7.0±3.5, p-value=0.001).

Days to defervescence by ciprofloxacin resistance. CIP-R, ciprofloxacin-resistant; CIP-S, ciprofloxacin-susceptible.
We performed multivariate analysis using logistic regression to evaluate the effects of independent variables on clinical failure (Table 4). Age, antibiotic use before visit, CIP resistance, and presence of bacteremia were the variables analyzed. CIP resistance had a significant effect, with a p-value of 0.044. The rest of the variables had no effect on clinical failure.
Discussion
Using data from a 1-year survey of 14 hospitals in South Korea, we were able to identify the most common causative organisms of UAPN, as well as their antimicrobial susceptibilities. E. coli was the most common organism, which is consistent with other studies,3,5,7 although their predominance was even more pronounced in our case, which may be attributed to the fact that all complicated pyelonephritis cases were excluded.
We were also able to confirm a high rate of resistance to CIP in UTI. The prevalence of CIP-resistant E. coli in our study was 15.9%, which is lower than that in previous studies, 8 but still warrants caution in selecting the empiric treatment for UTI. Another worrying finding was the high frequency of ESBL-producing E. coli in UAPN. Considering that only UAPN cases were included in this study, the ESBL frequency of 7.6% is surprisingly high, although it may be an overestimate, because 8 of the 14 hospitals participating in the study were tertiary centers, and tertiary centers test ESBL-production in Gram-negative urinary pathogens. Taking into account the rates of resistance to CRO, ceftazidime, cefepime, and aztreonam, the rate of resistance to extended-spectrum cephalosporins would range from 5.5% to 7.6%, still a high rate of resistance. Furthermore, 4.3% (16 of 397) of the patients were infected with E. coli co-resistant to CIP, SXT, and extended-spectrum cephalosporins. Fortunately, susceptibilities to amikacin and piperacillin-tazobactam remains high. Given the high rate of resistance to SXT and FQ, piperacillin-tazobactam and the extended-spectrum cephalosporins, amikacin or carbapenem, would be the best choices for empirical treatment of severe UAPN in Korea.
We were able to demonstrate a significantly worse outcome when patients with FQ-resistant E. coli were treated with FQs than with FQ-sensitive E. coli as with the study of SXT,10,11 which demonstrated the clinical relevance of microbiologic data. Among the patients with bacteremias, clinical outcomes were worse in the CIP-R group than in the CIP-S, as expected. 9 On the other hand, in patients who were treated with CIP or LEV without switching antibiotics, regardless of susceptibility to CIP or LEV, the clinical outcomes were not significantly different in the CIP-S and CIP-R groups, which suggests that mild diseases are reasonably responsive to CIP or LEV, regardless of susceptibility, although the numbers compared were small. Indeed, the number of days to defervescence of the patients in the CIP-R group who did not switch antibiotics were less than those of the patients who switched antibiotics with marginal significance (3.9 days vs. 4.9 days, p=0.052, data not shown). A recent report by Lee et al. clearly shows that the clinical outcomes of community-acquired bacteremic acute pyelonephritis were worse in patients receiving discordant empirical therapy (empirical treatment with antibiotics to which the pathogens are resistant) than in those receiving concordant therapy (empirical treatment with antibiotics to which the pathogens are susceptible) at 34.5% and 82.2%, respectively, when they evaluated clinical response after 3 days of treatment. 9 In that report, CIP was empirically used as the initial treatment regimen in 80.5% of cases. The clinical impact of discordant therapy was more significant than in our data, perhaps because bacteremic pyelonephritis cases were included in that study and 73% of the patients had underlying diseases such as diabetes, cerebrovascular diseases, chronic liver diseases, chronic kidney diseases, malignancy, urinary tract stone diseases, neurogenic bladder, and so on. Therefore, in areas with a high resistance to CIP, the disease severity and comorbidity of the patients needs be considered before determining the empirical treatment regimen. Furthermore, clinical impact of CIP or LEV resistance to lower UTI is certainly necessary.
Another important finding in this study was the longer hospital stays of CIP-R patients, which suggest that the medical costs of UAPN due to resistant bacteria are higher than those due to susceptible bacteria. The distribution of days to defervescence was not normal in the FQ resistant group; instead, it had two peaks (Fig. 2). On examination, patients with previous antibiotic use (n=7) had defervescence times between 0 and 3 (days mean: 1.57, standard deviation: 0.98), while patients with no previous antibiotic use (n=23) had defervescence times ranging from 0 to 11 with a mean of 4.87 (p=0.016). Nevertheless, it would be interesting to examine the correlation between the CIP or LEV MIC of uropathogens and clinical outcomes.
There are limitations to this study, namely, the small sample size and retrospective nature of the study. Therefore, the diagnosis of acute pyelonephritis could not be verified by the study group, because we included cases according to their final diagnosis in the medical records. In addition, the data for previous use of antibiotics for UTI before the current hospital visit, and for UTI history in the previous year, might be underestimated, as we noticed a higher culture negative rate than previous use of antibiotics before the hospital visit. Another limitation is that the APN cases in this study may be a selected sample, because 656 of the 719 cases (91.2%) were hospitalized, and the sepsis rate was as high as 30% in our study. Although many patients with APN with fever are hospitalized in Korea because medical insurance covers hospitalization costs, mild APN cases with minimal fever may not have been included in the study. In order to control for these limitations, a prospective study with larger numbers of cases is warranted.
In conclusion, the frequency of CIP sensitivity among E. coli isolates from Korean patients with UAPN was 84.1%. CIP or LEV treatment of UAPN caused by CIP-resistant E. coli had poorer clinical outcomes, with a lower cure rate and longer hospital stays than treatment of CIP-sensitive E. coli.
Footnotes
Acknowledgments
Funding: This work was supported by a grant of the Korea Healthcare Technology R&D Project, Ministry of Health and Welfare, Republic of Korea (A084063).
Disclosure Statement
None to declare.