
Abstract
The purpose of this study was to examine the carbapenemase-encoding resistance genes and analyze homologous of multidrug-resistant Acinetobacter baumannii (MRAB) isolates from nosocomial infections. Seventy-six A. baumannii strains were collected from inpatients and object surface of devices in intensive care units from May 2008 to February 2011. Antibiotic susceptibility testing of 18 antimicrobial agents was performed. The presence of carbapenemase-encoding resistance genes was investigated by polymerase chain reaction. Genotyping and dendrogram analysis of A. baumannii strains from nosocomial infections were performed using the DiversiLab System. All of the 76 clinical A. baumannii isolates were shown multidrug resistance. The blaOXA-23 gene was identified in the 76 MRAB strains, while blaOXA-24, blaOXA-58, VIM, IMP-1, IMP-4, SIM, and blaNDM-1 were absent in all. Twenty-four A. baumannii strains from the samples with nosocomial infections were classified into four unrelated groups and nine patterns. In conclusion, production of blaOXA-23 in MRAB is one of the molecular mechanisms responsible for carbapenem resistance. The MRAB strains from unrelated groups show different drug resistance, but the homologous strains also have different drug resistance. Homologous analysis can provide scientific evidence for evaluation of epidemic status of nosocomial infection caused by MRAB.
Introduction
For epidemiological and clinical purposes, a rapid understanding of DNA fingerprints of A. baumannii isolates is necessary to develop effective strategies to control their spread. Repetitive sequence-based polymerase chain reaction (rep-PCR) has been recognized as an effective method for bacterial genotyping; however, discriminatory power and reproducibility can be poor. 6 DiversiLab Microbial Typing System is based on microfluidics detection using the reagent-specific rep-PCR amplification kits, and software for data processing and data analysis allowing determination of genetic relatedness of identified isolates. 23 This method has demonstrated good discriminatory ability in the typing of A. baumannii isolates.4,5 The aim of the present study was to characterize the carbapenemase-encoding genes and evaluate drug resistance of MRAB isolates from intensive care units (ICUs). The rep-PCR-based DiversiLab system was used to investigate the relatedness of the MRAB strains isolated from the samples with nosocomial infection and provide basic data to establish the strategy for prevention and control of nosocomial infection.
Materials and Methods
Strains
A total of 76 clinical strains were isolated from sputum, blood, intraperitoneal drainage, bronchial perfusate of inpatients and object surfaces of respirators, bedrails and bedclothes in ICUs from June 2008 to February 2011. Forty-five strains were obtained from emergency intensive care unit (EICU) patients, 3 strains from EICU ventilators, 1 strain from EICU bedrail, 1 strain from EICU bedclothes, 12 strains from each of the respiratory intensive care unit (RICU) and neurology ICU, respectively; one strain from each of the burn ICU and neurosurgery ICU, respectively.
Among these 76 A. baumannii isolates, 24 strains were identified as nosocomial infection strains using the “Diagnostic Criteria for Nosocomial Infection (Trial)” established by the Ministry of Health. 11 Eleven strains were obtained from EICU (five strains from Sichuan earthquake casualty and six strains from hospitalized patients), three strains from EICU ventilators, one strain from EICU bedrail, one strain from EICU bedclothes, five strains from RICU; one strain from each of the burn ICU, neurology ICU, and neurosurgery ICU, respectively (Table 1).
ICU, intensive care unit; EICU, emergency intensive care unit; RICU, respiratory intensive care unit; G, group; P, pattern.
Identification of A. baumannii isolates
All strains were primarily identified in the clinical microbiology laboratory by standard biochemical tests as well as the VITEK 2 system (bioMérieux, Marcy l'Etoile, France). Furthermore, the more reliable genetic method of housekeeping gene of citrate synthase (gltA) sequencing analysis was conducted.20,21 A DNA template was prepared by the boiling method 18 and quantitated using Biophotometer (Eppendorf, Hamburg, Germany). Presence of the gltA gene was screened by PCR and using specific primers: F 5′-AATTTACAGTG GCACATTAGGTCCC-3′ and R 5′-GCAGAGATACCAGCAG AGATACACG-3′. 21 PCR products were purified using a QIAquick PCR Purification Kit (Qiagen, Courtaboeuf, France) and sequenced using an ABI 3100 Automated Sequencer (Applied Biosystems, Foster, CA). Results of sequencing were then compared with the GenBank database using BLAST (www.ncbi.nih.gov). The international standard strains of Acinetobacter calcoaceticus (ATCC 23055), Acinetobacter genomic species 3 (ATCC 17922), Acinetobacter genomic species 13TU (ATCC 17903), Escherichia coli (ATCC 25922), and Pseudomonas aeruginosa (ATCC 27853) were used as control strains.
Susceptibility testing
For ampicillin (AMP), ampicillin/sulbactam (AMS), aztreonam (ATM), cefepime (FEP), cefotetan (CTT), ceftriaxone (CRO), ceftazidime (CAZ), ciprofloxacin (CIP), nitrofurantoin (NIT), piperacillin/tazobactam (TZP), cefoperazone/sulbactam (SCF), tobramycin (TOB), cefazolin (CZ), amikacin (AK), gentamicin (CN), imipenem (IMP), levofloxacin (LEV), trimethoprim/sulfamethoxazole (SXT), and Polymyxin B (PB), susceptibility testing was performed using VITEK 2 system and minimal inhibitory concentrations were determined using the broth microdilution method, according to the CLSI protocol. 2 All antimicrobials were obtained from bioMérieux (Hazelwood, MO) and stored according to the manufacturer's instructions. E. coli ATCC 25922 and P. aeruginosa ATCC 27853 were used as reference strains for susceptibility testing.
Molecular detection of carbapenemase-encoding genes
Primers were obtained from Invitrogen, Inc. (Shanghai, China) and used for amplification and sequencing of blaNDM-1, 8 SIM, 9 VIM, 25 IMP-1, 24 IMP-4, 24 blaOXA-23, 7 blaOXA-24, and blaOXA-58. 16 Positive PCR products were purified and sequenced as described above. Results of sequencing were analyzed with the GenBank database using BLAST.
Genotyping of A. baumannii strains by DiversiLab system
For 24 strains from nosocomial infection, DNA was extracted using one 5-μL loops of plated culture and the UltraClean™ Microbial DNA Isolation Kit (MO BIO Laboratories, Inc., Carlsbad, CA) according to the manufacturer's instructions. All DNA solutions were standardized to a concentration of 25 ng/μL. According to the manufacturer's recommendations, the DiversiLab™ Acinetobacter Fingerprinting Kit (Bacterial Barcodes, Inc., Athens, GA) was used for rep-PCR amplification of noncoding intergenic repetitive elements in the genomic DNA from A. baumannii isolates. PCR was performed on a Veriti™ Thermal Cycler (Applied Biosystems, Foster, CA) using the following parameters: initial denaturation at 94°C for 2 min; 35 cycles at 94°C for 30 sec, 50°C for 30 sec, and 70°C for 90 sec; with a final extension at 70°C for 3 min. Amplicons were analyzed using the DiversiLab system, which includes fragment separation using microfluidic chips (Caliper Technologies, Inc., Mountain View, CA) and the Agilent™ B2100 Bioanalyzer (Agilent Technologies Inc., Palo Alto, CA). DNA standard markers (used for normalization of sample runs) and 1 μL of the Chip Kit molecular weight ladder (consisting of concentrations of 5 ng/μL of different DNA marker) were used. Results analysis was then performed with the DiversiLab software, which uses the Pearson correlation coefficient to determine distance matrices and the unweighted pair group method with arithmetic averages to create dendrograms.
Homologues were determined by cluster analysis and manufacturer's guidelines. Isolate combinations were categorized as indistinguishable, similar, or different. Multiple sets of characterized isolates and outbreaks were compared by criterion standard analysis. Different was defined as having less than 95% similarity and ≥2 band differences for homogeneous organisms or ≥3 band differences for heterogeneous organisms. Subsequently, strains were divided into the different clone groups. Similar was defined as having 1 band difference for homogeneous organisms or ≥2 band differences for heterogeneous organisms. Strains in the same clone group were considered to be closely similar. Indistinguishable was defined as having >97% similarity and no banding differences, including no variation in the intensities of individual bands; however, overall intensities may differ. These strains were classified as a same pattern. 19
Results
Outcome of gltA PCR
The 76 strains of A. baumannii were positive for the gltA gene. The amplicon size was approximately 722 bp (Fig. 1). The sequence compared with GenBank database using the BLAST tool and was 100% identical to that of GenBank accession nos. DQ156710.1 for gltA.
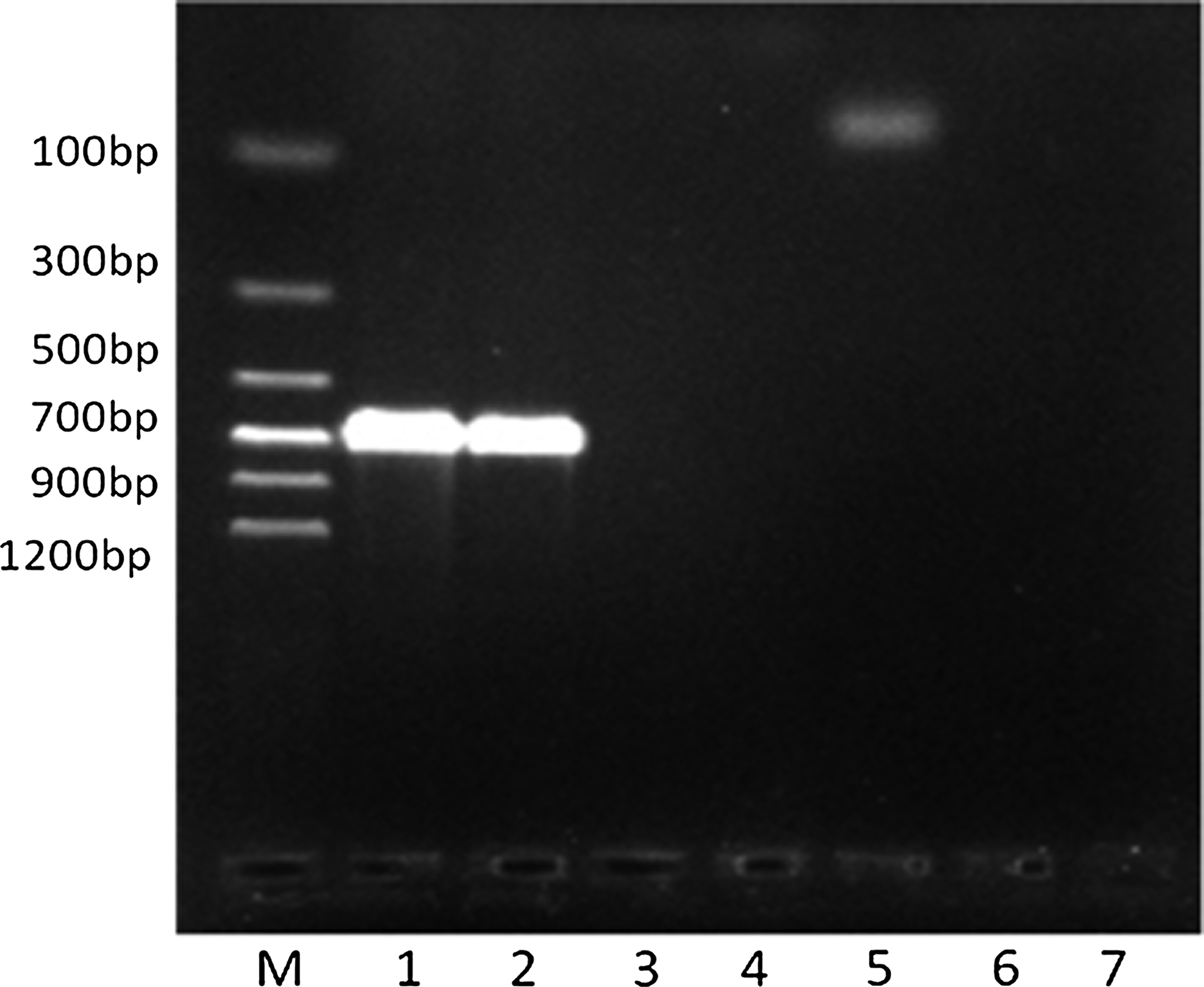
The gltA gene from clinical Acinetobacter baumannii isolates at profile of gel electrophoresis. M, DNA marker (Tian Biotech, Beijing, China); blot 1 and 2, A. baumannii; blot 3, A. calcoaceticus; blot 4, A. genomic species 3; blot 5, A. genomic species 13TU; blot 6, Escherichia coli; blot 7, Pseudomonas aeruginosa.
Results of antibiotic susceptibility testing
Results of antibiotic susceptibility testing for the 76 strains are summarized in Table 2. All of the clinical A. baumannii isolates were shown multidrug resistance. Overall, the rates of resistance to the majority of antibiotics tested varied between 65.8% and 100%: all the strains were resistant to AMP, ATM, CTT, CRO, CIP, IMP, NIT, TZP, SXT, and CZ; 97.4% of the strains were resistant to AK, 93.4% were resistant to AMS, 98.7% were resistant to FEP, CAZ, CN, and TOB, 80.3% were resistant to LEV, and 65.8% were resistant to SCF. For Polymyxin B, most of the strains were sensitive to it, only 1.3% of the strains showed resistance.
The number of sample cases.
AK, amikacin; AMP, ampicillin; AMS, ampicillin/sulbactam; ATM, aztreonam; FEP, cefepime; CTT, cefotetan; CRO, ceftriaxone; CAZ, ceftazidime; CIP, ciprofloxacin; CN, gentamicin; IMP, imipenem; LEV, levofloxacin; NIT, nitrofurantoin; TZP, piperacillin/tazobactam; SCF, cefoperazone/sulbactam; TOB, tobramycin; SXT, trimethoprim/sulfamethoxazole; CZ, cefazolin; PB, polymixin-B; MICs, minimal inhibitory concentrations.
Resistant genes to carbapenems of A. baumannii strains
The strains were checked for the presence of carbapenemase-encoding genes using the PCR methods described above. All of them were positive for the blaOXA-23 gene (Fig. 2), while blaOXA-24, blaOXA-58, VIM, IMP-1, IMP-4, SIM, and blaNDM-1 were absent in all. The gene blaOXA-23 from these strains was sequenced and compared with GenBank database using the BLAST tool and were 100% identical to that of GenBank accession nos. HQ700358 for blaOXA-23.
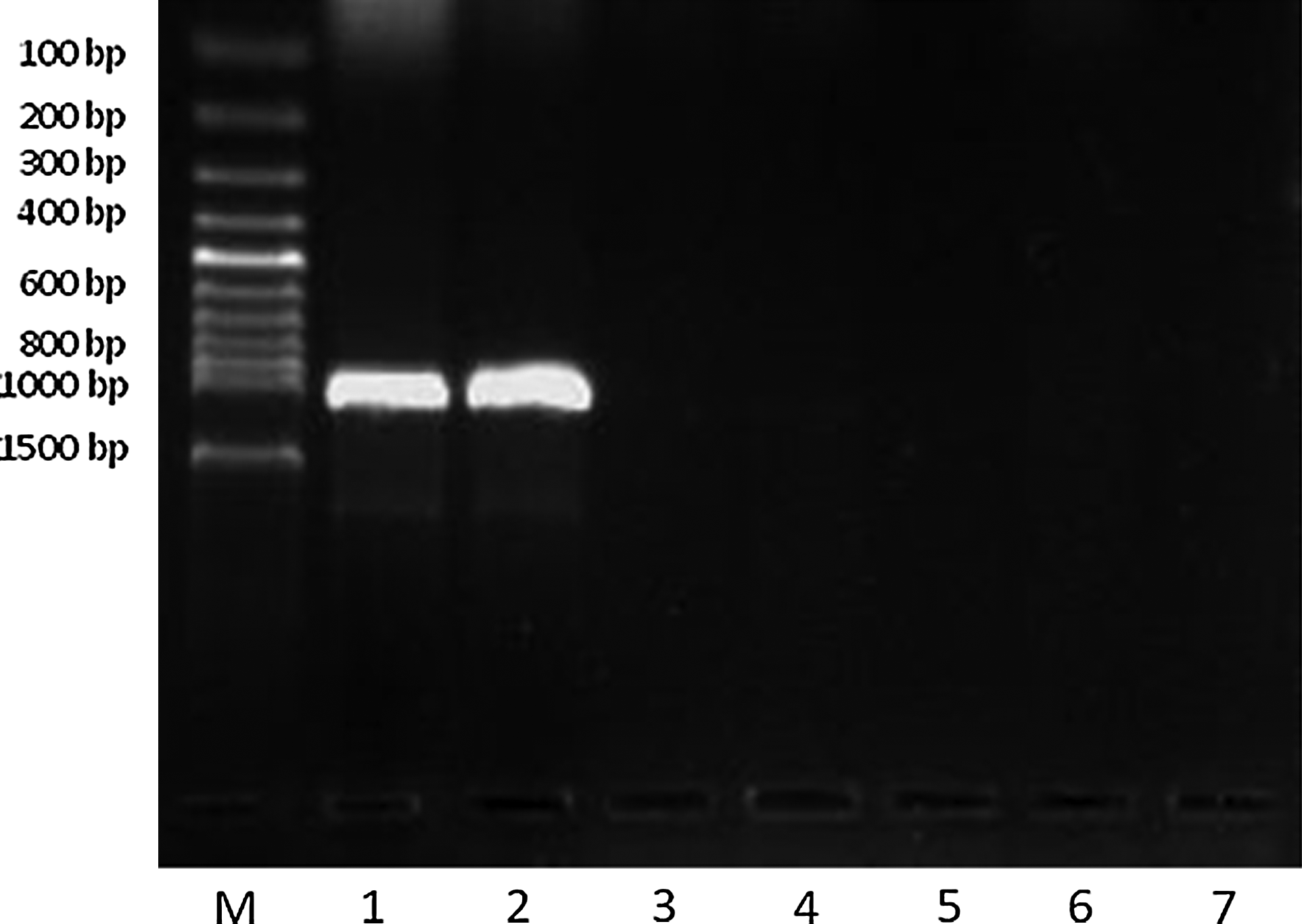
The blaOXA-23 gene from A. baumannii clinical isolates at profile of gel electrophoresis. M, DNA marker (Tian Biotech); blot 1 and 2, A. baumannii; the control strains of negative for the blaOXA-23 gene (blot 3, A. calcoaceticus; blot 4, A. genomic species 3; blot 5, A. genomic species 13TU; blot 6, E. coli; blot 7, P. aeruginosa.).
DiversiLab genotyping of A. baumannii strains
Twenty-four A. baumannii strains of nosocomial infection were classified into four unrelated groups by DiversiLab system (Fig. 3). Group 1 consisted of 16 A. baumannii strains that could be divided into four patterns. Pattern 1 to 4 had eight, four, three, and one strains, respectively. Six strains belonged to group 2 were divided into three patterns: pattern 1 included four strains; pattern 2 and 3 included one strain, respectively. Group 3 and 4 had one A. baumannii isolate, respectively (Fig. 4).
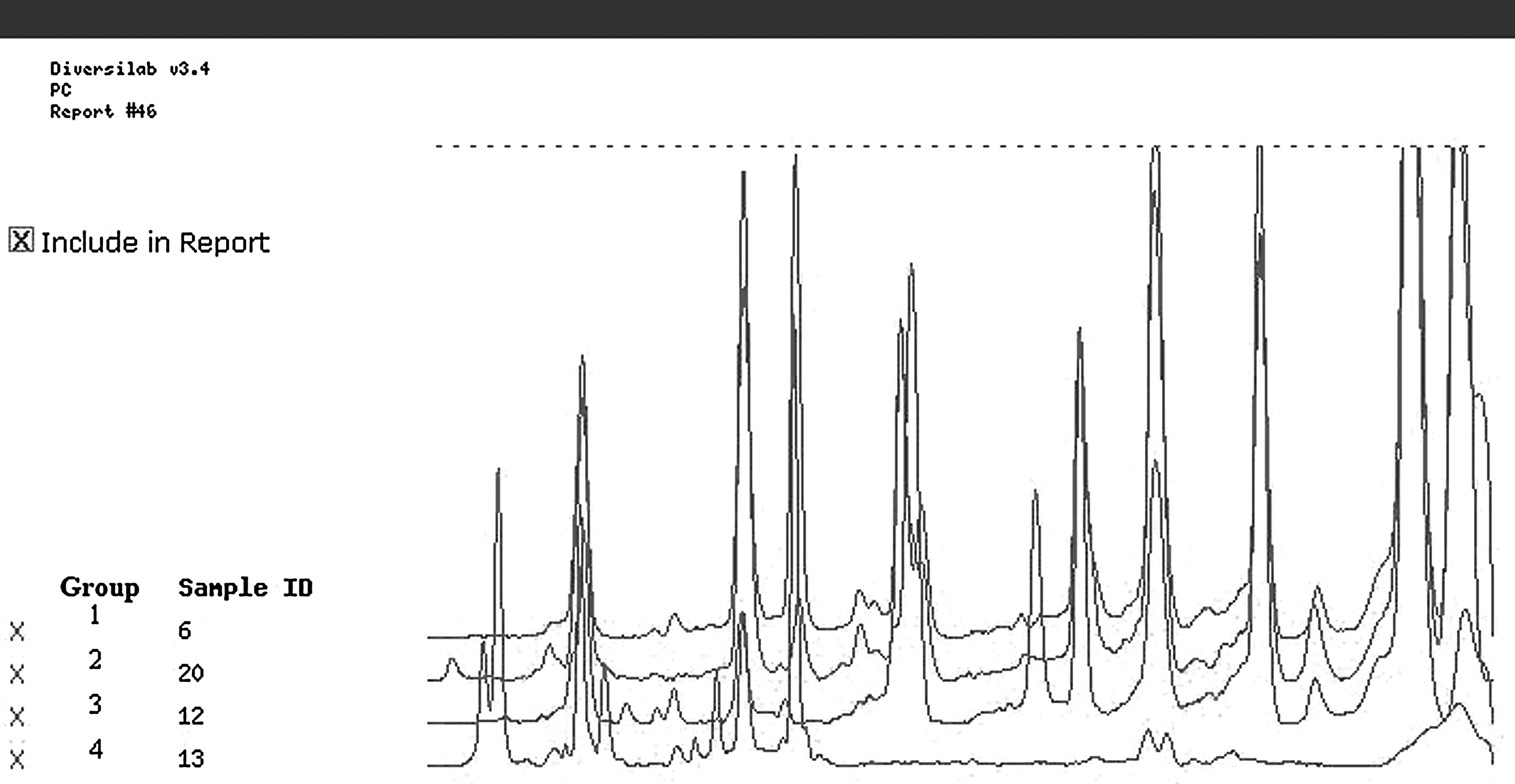
DNA fingerprints of four A. baumannii isolates from four different groups.
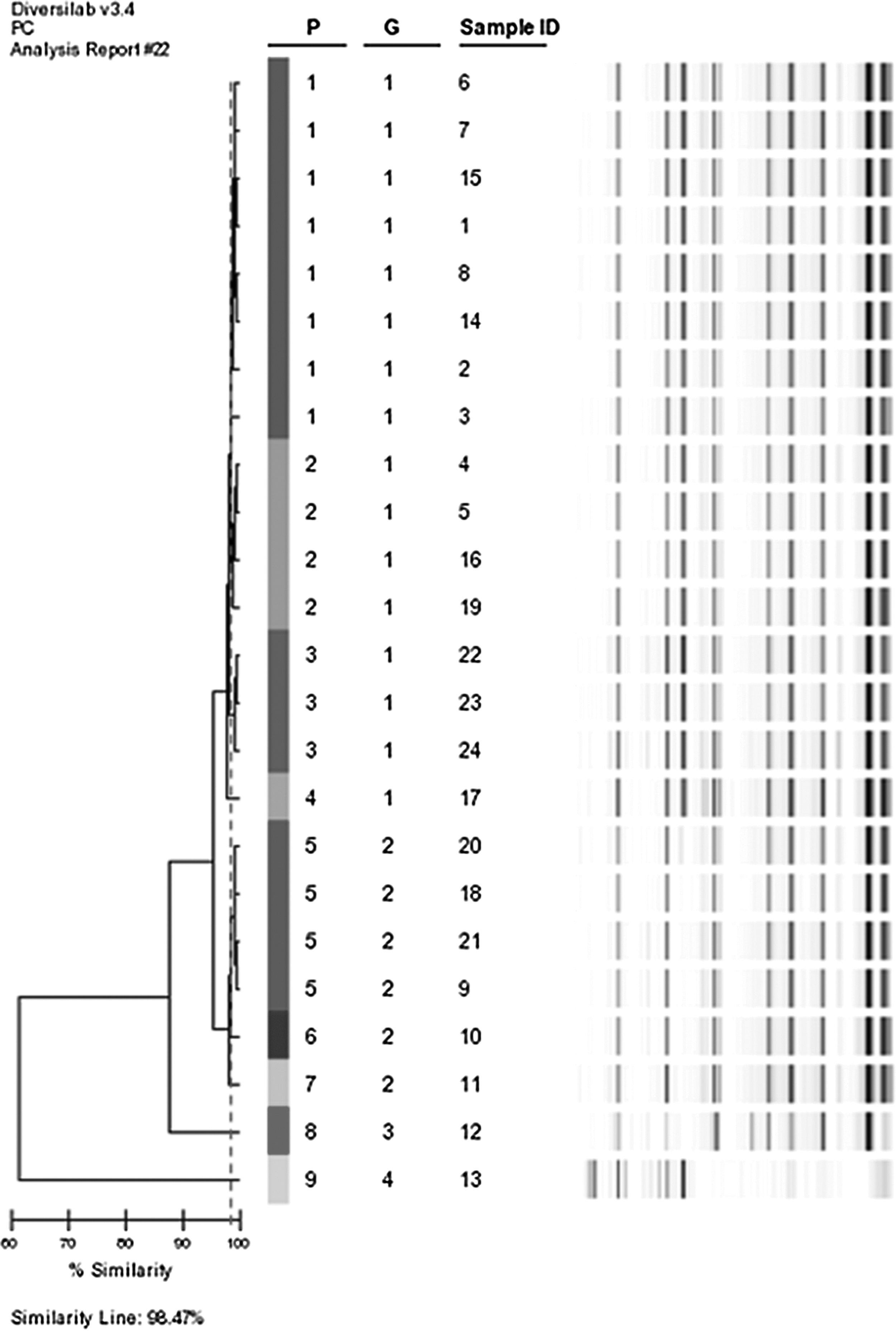
DiversiLab system homologous analysis and gel images for 24 clinical MRAB isolates from nosocomial infections. Sample ID, strain number; G, group; P, pattern; MRAB, multidrug-resistant Acinetobacter baumannii.
Drug resistance of genotyping A. baumannii strains
A. baumannii strains in Group 1 were divided into four patterns (Table 3). As to PB, most of the strains shown sensitivity, only No. 14 and No. 15 strains both from pattern 1 were moderately sensitive and resistant to PB, respectively. For other antibiotics: all strains in pattern 1 shown resistance; in addition, to one strain in pattern 2 (four strains), No. 16 strain was moderately sensitive to LEV and not susceptible to other antibiotics, the remaining strains shown resistance; in pattern 3 (a total of three strains), No. 23 and No. 24 strains were moderately sensitive to LEV and not susceptible to other antibiotics, No. 22 strain shown resistance; No. 17 strain in pattern 4 was moderately sensitive to SCF and not susceptible to other antibiotics. Six A baumannii strains belonged to Group 2 and were divided into three patterns: in pattern one (four strains), three strains (No. 18, 20, and 21) were moderately sensitive to LEV and No. 10 strain from pattern 2 was susceptible to FEP and CAZ and moderately sensitive to AK; No. 11 strain in pattern 3 was moderately sensitive to SCF, the remaining strain was resistant to other antibiotics. Two strains from Group 3 (No. 12) and Group 4 (No. 13) were resistant to all the other antibiotics.
R, resistance; I, intermediate-sensitivity; S, sensitivity.
Discussion
MRAB has been reported increasingly during the last decade, probably as a consequence of extensive use of antimicrobial agents. Carbapenem resistance in A. baumannii is now considered as a significant health problem because of limited options for antibiotic treatment.13,17 In our study, all strains were resistant to AMP, ATM, CTT, CRO, CIP, IMP, NIT, TZP, SXT, and CZ, and only 11.8% of the strains were susceptible to SCF, while less than 6% of the strains were susceptible to other antimicrobials: AK, AMS, FEP, CAZ, and TOB, and only 1.3% of the strains were resistant to PB. From the results, it is likely that PB will be an important antimicrobial option against MRAB. Thus, as to the infections caused by MRAB, maybe the clinician should first consider to use PB.
The mechanisms underlying resistance to carbapenems in A. baumannii are still poorly understood, but they would be expected to be similar to those described in other Gram-negative bacteria: production of carbapenem-hydrolyzing β-lactamases, alterations in penicillin-binding proteins, decreased outer membrane permeability caused by the loss or reduced expression of porins, over expression of multidrug efflux pumps. 19 In A. baumannii, class D carbapenemases are most popular, blaOXA-23, blaOXA-24, blaOXA-51, blaOXA-58 genes are predominant. Recently, it has been suggested that enzymes belonging to the BlaOXA-51 subgroup are intrinsic to A. baumannii. 12 Thus, the blaOXA-51 gene was not included in the study. From the results, the blaOXA-23 gene was found in all isolates, indicating the importance of this gene in carbapenem resistance in our ICU settings.
The surveillance systems of nosocomial infections must be rapid, reliable, and capable of distinguish between related and unrelated bacterial strains, especially in highly critical areas, such as ICUs. This article was to look for genotypic similarities among phenotypically similar clinical MRAB strains and investigate the epidemic situation of A. baumannii in ICUs using DiversiLab system, and to provide evidence for prevention and control of nosocomial infection. The results indicated that there were four different groups of A. baumannii in our hospital from June 2008 to May 2010, some strains had affinity with the A. baumannii isolated from the injured in 5.12 Sichuan earthquake. The A. baumannii isolated from some patients in RICU (strain No. 20 and 21) and EICU (strain No. 18) in May 2010 were homologous strains, suggesting that the epidemic of homologous A. baumannii in the two ICUs appeared once again. The main reason was the transfer of EICU patients into RICU and the EICU A. baumannii was carried into the RICU with patients. The A. baumannii isolated from the EICU ventilator and bed rails had affinity with the A. baumannii isolated from some patients in May 2010 and some strains were homologous strains, indicating that part of the equipments or objects surfaces in EICU have long A. baumannii colonization. Furthermore, the different A. baumannii isolates in the same clone group could have different resistant phenotypes and the different A. baumannii isolates in the same pattern may also have different drug resistance.
In conclusion, the MRAB is an increasing problem in ICUs, with many strains now resistant to most of the available antibiotics. BlaOXA-23-like acquired carbapenemase gene plays an important role in the resistant mechanism of A. baumannii. Our study confirms that the genotyping of A. baumannii offers us accurate and reproducible results to support the infection control team in routine A. baumannii surveillance and outbreak investigations.
Footnotes
Acknowledgments
We thank all patients who donated their samples for this study, Qiao Ning for assistance in field work, Guo Lu for her guidance in the test and helpful discussions. A special thanks to all the participants in this study.
Disclosure Statement
All authors state that no competing financial interests exist.