
Abstract
Introduction
M
Materials and Methods
Specimens and bacterial isolates
One hundred nonrepetitive patient isolates of multidrug-resistant A. baumannii (MDR-AB) were collected from the ICU patients of Imam Khomeini Medical Center (IKMC) and Children Medical Center (CMC) in Tehran, Iran. The IKMC and CMC centers are affiliated with the Tehran University of Medical Sciences (TUMS), and both provide tertiary patient care to patients referred from various regions of Iran. To compare the phenotypic and genotypic changes among MDR-AB isolates, samples were collected within a 5-year period, from 2006 to 2011 (50 isolates per year). The 2011 patient specimens were collected from the same ICU that provided samples during 2006. About 10% of the MDR-AB isolates were isolates from our recent report. 3
The MDR-AB strains were isolated from several sources, including wound (n=42), respiratory tract (n=36), urine (n=9), blood (n=7), and CSF (n=6). A. baumannii were initially identified using the API20NE system (bioMérieux) and later confirmed by gyrB multiplex PCR, as previously described (Supplementary Fig. S1; Supplementary Data are available online at www.liebertpub.com/mdr). 13
Antimicrobial susceptibility tests
The Clinical Laboratory Standards Institute (CLSI) guideline 21 for minimum inhibitory concentrations (MICs) using the E-test was used to assess the susceptibility of MDR-AB isolates to ampicillin–sulbactam (SAM, 0.016–256/0.008–128 μg/ml; 2:1 ratio), cefepime (FEP, 2–256 μg/ml), ceftazidime (CAZ, 2–256 μg/ml), ciprofloxacin (CIP, 0.01–240 μg/ml), colistin (CST, 0.01–240 μg/ml), co-trimoxazole (COT, 0.01–240 μg/ml), imipenem (IPM, 4–256 μg/ml), levofloxacin (LVX, 0.01–240 μg/ml), minocycline (MIN, 0.01–240 μg/ml), piperacillin (PIP, 0.01–240 μg/ml), piperacillin–tazobactam (TZP, 0.01–240 μg/ml, each dilution contains 4 μg of tazobactam), rifampicin (RIF, 0.01–240 μg/ml), tetracycline (TET, 0.01–240 μg/ml), tigecycline (TGC, 0.016–192 μg/ml), and tobramycin (TOB, 0.01–240 μg/ml).
All antimicrobial E-Test® strips (HiMedia Laboratories Pvt. Ltd.), including SAM E-Test® strips (bioMérieux), were used according to the manufacturer's recommendations. For tigecycline susceptibility tests, the criteria of the European Committee on Antimicrobial Susceptibility Testing (EUCAST) for members of Enterobacteriaceae were used (i.e., MIC of ≤1 mg/L defined as susceptible and >2 mg/L as resistant). 37 Also, rifampicin susceptibility was interpreted according to CLSI criteria using breakpoint values suggested for Staphylococcus aureus (susceptible and resistant defined as ≤1 mg/L and ≥4 mg/L, respectively). 21 MIC determinations included MIC range, MIC50, and MIC90 for each isolate using Escherichia coli ATCC 25922, Pseudomonas aeruginosa ATCC 27853, and E. coli ATCC 35218 as quality control organisms. Isolates were defined as multidrug resistant (MDR), extended spectrum drug resistant (XDR), or pandrug resistant (PDR) according to the International Expert proposal for Interim Standards guidelines. 20 The MDR-AB strain was defined as nonsusceptibility to at least one member of the three antimicrobial classes, and tigecycline and rifampicin susceptibilities were excluded from MDR definition.
Molecular typing
Clonal lineage of MDR-AB isolates was determined by amplified restriction fragment polymorphism (AFLP) by a ligation-PCR method, as previously described (Supplementary Fig. S2). 3 Briefly, genomic DNA from isolates were double digested with MboI and MseI (Fermentas), ligated to adaptors (Table 1), and used as templates for preliminary PCR using Mbo- and Mse-specific primers (Table 1). Preliminary PCR products were amplified by selective PCR to generate AFLP profiles, determined by image analysis of gel-resolved bands using BioNumerics version 5.10 (Applied Maths) with A. baumannii NCTC 12156 as a normalization reference. The similarity between band patterns was calculated using the Dice coefficient (with an optimization of 0.5% and a position tolerance of 1%). The AFLP clusters and type identification were defined by groups formed at 60% and 90% Dice similarity cutoffs, respectively, on a dendrogram constructed by the unweighted pair group method using average linkages (UPGMA).
Nucleotide.
AFLP, amplified fragment length polymorphism.
Determination of International clonal types
International clone (IC) types were determined using two complementary multiplex PCR assays (primers, Table 1), as previously described. 42 Multiplex PCR assays selectively amplified the outer membrane protein A (ompA), chaperone–subunit usher E (csuE), and intrinsic carbapenemase (blaOXA-51-like) genes of MDR-AB isolates. Standard AB strains belonging to IC type I, II, and III served as controls. Strains positive for all three ompA, csuE, and blaOXA-51-like allele amplicons were identified as IC type I, and isolates not assigned as either IC type I, II, or type III were reported as the variant (V) clonal type.
Results
Antimicrobial susceptibility testing
Overall, resistance against all test antimicrobials (10 classes) among MDR-AB isolates from ICU patients increased, except for tobramycin. During a 5-year period, the frequency of resistant MDR-AB isolates against each antimicrobial increased by 11–30% (Table 2). By 2011, all MDR-AB isolates had become completely resistant to group A ceftazidime and three other group B antimicrobials, namely, piperacillin, cefepime, and co-trimoxazole. In contrast, all 2006 isolates were only resistant against ceftazidime. In addition, Table 2 shows that MDR-AB isolates from 2011 had the lowest frequency of resistance to colistin (6%), tigecycline (8%), and minocycline (8%).
Most antimicrobial agents were selected according to CLSI-defined grouping of A, B, and O antimicrobial groups.
CAZ, ceftazidime; CIP, ciprofloxacin; CLSI, Clinical Laboratory Standards Institute; CMC, Children Medical Center; COT, co-trimoxazole; CST, colistin; FEP, cefepime; IKMC, Imam Khomeini Medical Center; IPM, imipenem; LVX, levofloxacin; MIC, minimum inhibitory concentration; MIN, minocycline; PIP, piperacillin; RIF, rifampicin; SAM, ampicillin/sulbactam; TET, tetracycline; TGC, tigecycline; TOB, tobramycin; TZP, piperacillin–tazobactam.
MIC determinations of MDR-AB isolates, 2006 versus 2011, revealed a rising trend of higher MIC ranges across all test antimicrobial agents (Table 2). Although for most antibiotics, MIC ranges showed a twofold increase in the high-end of MIC range; the increases for colistin, tigecycline, and imipenem were 32-, 30-, and 4-fold, respectively. Within 5 years, MIC50 for all test antimicrobials also increased, except for piperacillin, tobramycin, minocycline, and tetracycline. MIC90 concentrations against A. baumannii isolates also increased for all antimicrobials, and by 2011, MIC90 concentrations of test antibiotics were two to six times higher than MIC90 of isolates from 2006. Notably, MIC90 concentrations against tobramycin increased twofold, despite the decline in frequency of isolates resistant to this antimicrobial.
Table 2 also compares the MIC of antimicrobial agents against A. baumannii isolates according to the location of their isolation. While among A. baumannii isolates from both IKMC and CMC, the resistance rates to ceftazidime, cefepime, co-trimoxazole, and rifampicin were similar, overall, the isolates from IKMC showed upto threefold higher resistance rates than the CMC isolates during 2011. In fact, all tigecycline-resistant A. baumannii isolates were isolated from IKMC (Table 2).
Table 3 shows the changes in antimicrobial resistance rates among MDR-AB isolates, between 2006 and 2011. The highest increase in frequency of resistant MDR-AB was against piperacillin (30%) and rifampicin (24%), whereas the smallest increase among isolates was against co-trimoxazole (2%) and minocycline (4%). While all 2006 isolates were susceptible to tigecycline and colistin, by 2011, MDR-AB resistance to these antibiotics had emerged and 6% of MDR-AB isolates were resistant to tigecycline and colistin (Table 3).
Antimicrobial agents are categorized according to CLSI-defined grouping as A, B, and O antimicrobial groups.
According to CLSI guideline, considerations in the assignment of agents to Groups A, B, and O include clinical efficacy, prevalence of resistance, minimizing emergence of resistance, cost, FDA clinical indications for usage, and current consensus recommendations for first-choice and alternative drugs. Group A are considered appropriate for inclusion in a routine, primary testing panel, as well as for routine reporting of results for the organism. Group B comprises agents that may warrant primary testing. However, they may be reported only selectively, such as when the organism is resistant to agents of the same class, as in Group A. Group O (other) includes agents that have a clinical indication for the organism, but are generally not candidates for routine testing and reporting in the United States.
MDR-AB, multidrug-resistant Acinetobacter baumannii.
Table 3 also shows that while 52% of 2011 isolates remained susceptible to imipenem, carbapenem resistance rose by 18%, as compared to the 2006 isolates. Resistance to other first-line drugs (group A), for example, levofloxacin and ampicillin–sulbactam, also increased in 2011 by 14% and 10%, respectively. However, rates of resistance to ceftazidime and tobramycin remained unchanged or decreased slightly (Table 3).
AFLP analysis
AFLP analysis of MDR-AB isolates indicated drastic changes in genotypic patterns within a 5-year period. These changes were evidenced by the finding that novel IC variants comprised 36% of MDR-AB isolates in 2011.
Figure 1 shows the frequency of MDR-AB AFLP genotypes in 2006 and 2011, in addition to their antimicrobial resistance profile. Twelve distinct AFLP genotypes (A through L) were identified among all MDR-AB isolates with predominance of D, F, I, and J genotypes. Genotypes I and F (42% and 38%) were the most frequent genotypes in 2006 and 2011, respectively. In 2006, genotypes I and J comprised 62% of MDR-AB isolates, whereas in 2011, genotypes D and F accounted for 62% of isolates. While 98% of AFLP types included >1 MDR-AB isolate, only a single isolate of genotype A (in 2006) or G (in 2011) was isolated.
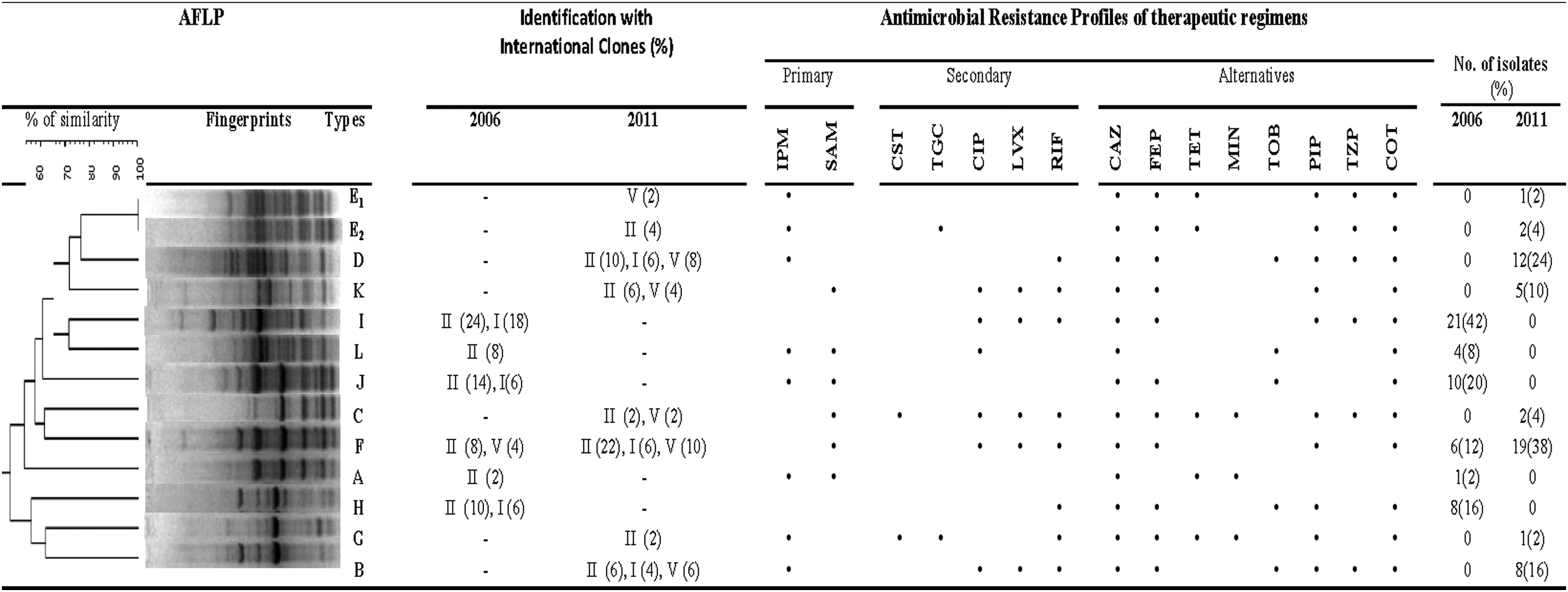
Dendrogram analysis of AFLP fingerprint patterns, and the international clone (IC) determination of MDR-AB isolates depicting the genetic relatedness of MDR-AB isolates from 2006 to 2011. Resistance to antimicrobial agents is indicated by closed black circle (•); antimicrobials are classified as primary, secondary, or alternative therapeutic regimens, according to Sanford guide® for antimicrobial therapy (http://webedition.sanfordguide.com/sanford-guide-online/disease-clinicalcondition/Acinetobacter baumannii, accessed September 18, 2012). AFLP, amplified fragment length polymorphism; CAZ, ceftazidime; CIP, ciprofloxacin; COT, co-trimoxazole; CST, colistin; FEP, cefepime; IPM, imipenem; LVX, levofloxacin; MDR-AB, multidrug-resistant Acinetobacter baumannii; MIN, minocycline; PIP, piperacillin; RIF, rifampicin; SAM, ampicillin–sulbactam; TET, tetracycline; TGC, tigecycline; TOB, tobramycin; TZP, piperacillin–tazobactam; V, variants of IC.
The F genotype was the only genotype observed in both 2006 and 2011, and its frequency increased by 14% among 2011 MDR-AB isolates. The scarcity of 2006 genotypes among 2011 isolates (and vice versa) suggests that dramatic clonal changes have occurred among MDR-AB isolates. It is notable that genotypes F and K showed the same antimicrobial susceptibility profile, despite their different AFLP profile; however, genotype E1 and E2 isolates had different antibiotic resistance patterns (i.e., E2 genotype resistance to tigecycline), despite showing an identical AFLP profile (Fig. 1).
MDR-AB isolates of genotype A (2006) were the most susceptible isolates being resistant to only 5 (33%) of the test antimicrobials; however, MDR-AB genotype B, C, and G isolates (2011) showed the broadest resistance profiles, showing resistance to 10–12 (66–80%) of antimicrobials. Although two of the 2011 isolates (genotype C) were defined as XDR-AB isolates (with an extended resistance profile), they remained susceptible to imipenem, tigecycline, and/or tobramycin (Fig. 1). MDR-AB genotypes with resistance to most (8 or 10) antimicrobial agents were isolated in 2011 (i.e., genotypes B, D, E2, F, G, and K). Interestingly, the only isolate resistant to both colistin and tigecycline (genotype G) remained susceptible to several conventional agents, including members of the primary (ampicillin–sulbactam), secondary (ciprofloxacin, levofloxacin), and alternative (piperacillin–tazobactam, tobramycin) groups (Fig. 1).
Figure 1 also compares the susceptibilities of MDR-AB isolates, which were resistant to first-line or last-resort drugs, against various conventional antimicrobials. For instance, in 2011, all carbapenem-resistant MDR-AB isolates as well as 98% of TGC+CST-resistant isolates were susceptible to either minocycline or tobramycin. In addition, analysis of simultaneous susceptibility of MDR-AB isolates to ≥2 antimicrobials revealed that all 2011 isolates were simultaneously susceptible to the following antimicrobials: ciprofloxacin–levofloxacin+tigecycline and colistin+tobramycin. Surprisingly, while 28% of 2006 isolates were simultaneously resistant to ampicillin–sulbactam and tobramycin, none of the isolates from 2011 showed simultaneous resistance to these antimicrobials. In other words, all 2011 MDR-AB were susceptible to either ampicillin–sulbactam or tobramycin (Fig. 1).
Further analysis of simultaneous susceptibility of MDR-AB genotypes showed that all imipenem-resistant 2011 isolates were susceptible to either ciprofloxacin–levofloxacin or tobramycin, except for genotype B isolates (16%). Although MDR-AB genotype A, J, and L isolates were resistant to both the primary (IPM and SAM) antimicrobials, they all remained susceptible to ≥4 of the secondary drugs (i.e., CST, TGC, CIP, LVX, or RIF). Only 2% of isolates were susceptible to either rifampicin or tigecycline (Fig. 1), signifying that 98% of MDR-AB isolates might be susceptible to a combination of these drugs, which remains to be tested.
Figure 2 shows the distribution of MDR-AB genotypes based on type, the year, and site of specimen collection from ICU patients. While in 2006, genotype I comprised most (35%) MDR-AB isolates from respiratory sites, the imipenem-resistant genotype D predominated among the respiratory 2011 MDR-AB isolates (31%). Interestingly, the predominant MDR-AB genotypes I (2006—42%) and F (2011—38%) were both imipenem susceptible and mostly isolated from wounds (Fig. 2). In fact, an increasing trend of carbapenem resistance was observed among MDR-AB recovered from all sites. For example, imipenem resistance rose by 10% and 19% in among respiratory and wound MDR-AB isolates, respectively. Genotypic profiles of 80% of MDR-AB isolates from 2011 (AFLP types C, D, E2, F, and G) were similar to the genotypes of isolates from our previous report, 3 which examined MDR-AB isolates from other parts of Iran and other patients in Tehran (Supplementary Table S1; Note: specimen overlap between studies was about 10%, unpublished data).
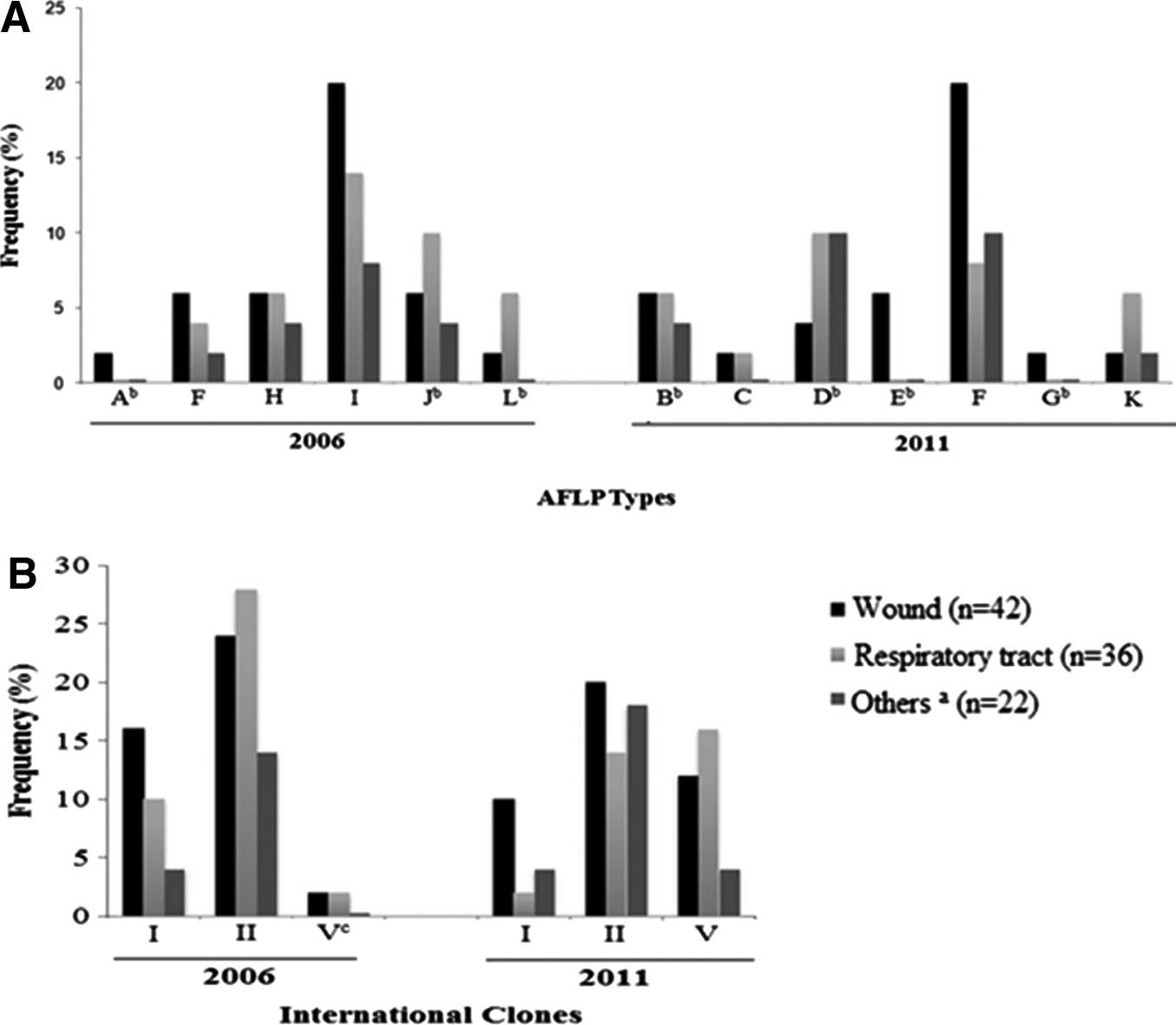
Frequency and distribution of AFLP genotypes of MDR-Acinetobacter baumannii (n=100) according to
Figure 2 also shows that the main IC type among MDR-AB isolates was IC type II (66% in 2006 and 52% in 2011). None of the isolates was identified as IC type III; however, IC type I isolates comprised 30% and 16% of MDR-AB from 2006 to 2011, respectively. While 36% of the 2011 MDR-AB isolates were assigned as “novel IC variant” type (not corresponding to the IC I, II, or III definitions), only 4% of the 2006 isolates were identified as novel IC variants. Among MDR-AB isolates from 2011, the novel variants of IC strains were most frequently (16%) isolated from the respiratory tract specimens.
Discussion
MDR-AB has emerged as a morbidly successful nosocomial pathogen, especially among the ICU patients with respiratory complications. 19 Widespread carbapenem-resistant MDR and XDR-AB isolates in ICU wards present grave challenges to clinicians facing a dearth of treatment options against severe MDR-AB infections. In developing countries like Iran, these challenges are magnified by barriers in obtaining the newly approved antimicrobial agents like tigecycline, compounded by growing MDR-AB resistance to drugs of last resort.3,6,14 Consequently, several studies have focused on approaches that may potentiate the activity of available antimicrobials to effectively treat MDR-AB infections.4,5,26,33
Recent reports have declared an urgent need for effective therapeutic regimens to control MDR-AB outbreaks in hospitals throughout the world,6,38 but given that MDR-AB susceptibility often depends on the isolate's origin, successful control measures necessitate epidemiologic knowledge of genotypic and antimicrobial susceptibility profile of local isolates.11,24,38 To address this need, our 5-year study compared the susceptibility patterns and the genotypic changes among MDR-AB isolates of two medical centers in Tehran, Iran.
Overall, we report an alarming trend of increase in MDR-AB resistance against a wide spectrum of antimicrobial agents in Tehran, Iran. If not controlled, this trend promises to eventually render even the last-resort antimicrobials inadequate while treating patients with severe MDR-AB infections. Among our greatest concerns is the recent emergence and growing number of MDR-AB strains, which are resistant to both tigecycline and colistin, as reported recently. 3 Fortunately, while the rising number of TGC+CST-resistant MDR-AB isolates reveals a worrisome trend of high frequency of XDR and PDR-AB cases, so far, all TGC+CST-resistant isolates have remained susceptible to a few conventional drugs, like tobramycin or ciprofloxacin–levofloxacin.
Generally, our findings are consistent with recent studies from Iran that show a growing trend of widespread carbapenem resistance among MDR-AB isolates.1,9,31,36 However, contrary to these reports, all imipenem-resistant MDR-AB isolates, in the present study, remained sensitive to conventional antimicrobials such as ciprofloxacin–levofloxacin or minocycline, which are readily available in Iran. The unexpected susceptibility of all 2011 MDR-AB isolates to either ampicillin–sulbactam or tobramycin and complete susceptibility of carbapenem-resistant isolates to either minocycline or tobramycin (despite their rising MIC90 values) deserve further evaluation. This effort might lead to potential therapeutic approaches for PDR-AB infections in Iran, especially since the prospects of availability of novel antimicrobials against PDR-AB infections seem bleak.4,5 We recently tested 200 additional MDR-AB isolates, which were 100% susceptible to either tobramycin or minocycline (Bahador, A. et al., unpublished data), and plan to verify these results in an in vivo model. Rising colistin resistance and poor clinical outcome 43 combined with high cost of tigecycline underscore the value of such assessments for developing countries. Combination therapy has reduced the risk of emergence of resistant strains in HIV disease, tuberculosis, as well as malaria39,40; some results of combination antibiotics against PDR-AB strains are promising.4,5,15,26
Taken together, our MDR-AB resistance and genotypic profile data suggest that MDR-AB isolates from IKMC and CMC represent a dynamic population whose members undergo marked clonal and susceptibility changes during a 5-year period. These clonal changes have given rise to novel MDR-AB variants, which present serious infection control challenges in Iran because resistance has probably contributed to their spread.12,22,41 This underscores the importance of enforcing continuous molecular epidemiologic monitoring programs in Iranian hospitals; however, method variation in studying the MDR-AB genotypic diversity from different parts of Iran1,9 has complicated data comparisons rendering the analyses inconclusive. Our recent finding of similar MDR-AB genotypes from Tehran (various areas of Iran 3 ) highlights the critical need for implementation of concerted monitoring and infection control policies, as well as local standardization of MDR-AB genotypic data analysis at the national level in Iran.
Additionally, at a regional level, the predominance of IC type II among our MDR-AB isolates is consistent with reports from other Asian countries, including China, Pakistan, South Korea, and Taiwan. 12 However, the high number of novel IC variants, from 2011, suggests that MDR-AB isolates from our sites may share similarities with local A. baumannii strains collected from regions closer to Tehran, as reported recently.3,16 Although the A. baumannii IC grouping was devised using mostly isolates from Europe and the United States, 18 identification of novel IC variants in Iran and several European countries 41 highlights the need for a comprehensive global system to group MDR-AB isolates.
In conclusion, we present evidence that MDR-AB isolates from Iran represent a dynamic population that undergoes marked genotypic and antimicrobial susceptibility change over 5 years. While these changes lead to development of resistance to several first-line and last-resort drugs, a majority of resistant MDR-AB remain sensitive to conventional agents, such as tobramycin and minocycline, which are viable agents in controlling MDR-AB outbreaks, especially in developing countries. Our findings highlight the importance of a comprehensive, national, susceptibility review program, which evaluates MDR-AB isolates from various parts of Iran. It also contends that effective global control measures against MDR-AB depend on vigilant epidemiologic monitoring of susceptibility profiles and novel IC clone variants of MDR-AB from all regions of the world, including Iran.
Footnotes
Acknowledgments
The authors would like to thank the dedicated ICU staff and laboratory personnel at the IKMC and CIDC hospitals (Tehran University of Medical Sciences Complex), who helped collect specimens for this study. They are also grateful to Dr. M.M. Feizabadi for the kind gift of A. baumannii NCTC 12156 as well as several clinical A. baumannii isolates.
Funding: This study was funded, in part, by the Office of Vice Dean for Medical Research at the Tehran University of Medical Sciences; grant No. 89. 01-30-10430.
Ethical approval: not required.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.