
Abstract
Acinetobacter baumannii, a substantial nosocomial pathogen, has developed resistance to almost all available antimicrobial drugs. Bacteriophage therapy is a possible alternative treatment for multidrug-resistant (MDR) bacterial infections. In this study, we have successfully isolated bacteriophage active against clinical strains of A. baumannii by enrichment from hospital sewage sludge using representatives of those strains. The bacteriophage isolated against A. baumannii formed plaques against beta-lactamases producing strains of A. baumannii. The utility of bacteriophage specific for A. baumannii to resolve wound infection in uncontrolled diabetic rats was evaluated. Five groups of uncontrolled diabetic rats were used. Group I was noninfected (Control), Group II was infected with MDR A. baumannii and challenged with bacteriophage, Group III was infected with MDR A. baumannii, Group IV was infected with MDR A. baumannii and challenged with antibiotic colistin, and Group V consisted of noninfected rats and sprayed with phage (Phage control). A significant decrease in infection, period of epithelization, and wound contraction was observed in the phage-challenged group when compared with antibiotic-treated uncontrolled diabetic rats and the control group. To conclude the study, new insights are provided into the biology of the broad host range of A. baumannii phage, demonstrating that A. baumannii phage has prospects for the treatment of infections caused by the MDR A. baumannii.
Introduction
A
Materials and Methods
Ethical clearance
The study was conducted in accordance with the National Institutes of Health guidelines for the care and use of animals in research, and the protocol was approved by the Institutional Animal ethics committee, S.S. Institute of Medical Sciences and Research Center, Davangere, Karnataka.
Bacterial isolates used for the study
A. baumannii strain isolated from diabetic foot infection was used to study the bactericidal effect of the phage and was designated as AB 38 in our nomenclature. Antibiotic susceptibility testing by Kirby–Bauer's method 4 revealed that the A. baumannii 38 (AB 38) strain was resistant to most of the commonly used drugs such as ceftazidime, cefepime, ceftriaxone, amikacin, cefoperazone, imipenem, meropenem, piperacillin, ciprofloxacin, levofloxacin, cotrimaxazole, piperacillin+tazobactam, and cefoperzone+sulbactam and sensitive to colisitin and polymyxin B. Staphylococcus aureus (ATCC No. 25923) and Escherichia coli (ATCC No. 25922) were used as control strains while performing the antibiotic susceptibility test. Metallo beta-lactamase production was detected by Imipenem-EDTA-combined disc test.2,6,13
Isolation and purification of phage strains for A. baumannii
The A. baumannii phage was isolated from an untreated hospital discharge near Government District Hospital, Davangere, by the method of Smith and Huggins.23,27,28 In vitro confirmation of bacteriophage activity was done on A. baumannii.11,15,20,29
Maintenance of rats
Six-month-old healthy male Wistar rats weighing 150–200 g, bred locally in the central animal house of S. S. Institute of Medical Sciences and Research Center, Davangere, were selected for the study. They were housed under controlled conditions of temperature (23°C±2°C), humidity (50%±5%), and 10–14 hr of light and dark cycles. The animals were housed individually in polypropylene cages containing sterile paddy husk (procured locally) as bedding, and free access to food and water (animal chow) ad libitum was provided throughout the study.27,28 All the animals were maintained on a proper diet and were housed in a pathogen-free environment. 9
Induction of diabetes mellitus in rats
Diabetes is induced by injecting Alloxan hydrate (C4H2N2O4·H2O; LOBA CHEMIE Pvt Ltd.), 80 mg/kg body weight, subcutaneously in rats after 12 hr of continuous fasting. 27 Fasting blood sugar was evaluated by using a Glucometer (SD Fine Chemicals) after 72 hr. Rats whose blood glucose levels remained <300 mg/dl for more than 1 week after the initial injection of alloxan received a second dose of alloxan to maintain a blood glucose level >300 mg/dl for the duration of the study.14,19
Evaluation of minimum infective dose of MDR AB 38
The rats were randomly divided into six groups of five animals each. The areas to be depilated were marked, usually 3×the area of the wound to be created. Cold wax strips were used for depilation. All the animals were body-marked for identification. An area of about 225 mm2 was defined with a marker on the depilated back of the rat, in the dorsal interscapular region, at 1 cm away from the ears of the rats. 27 The circular marked area of the skin was excised with full thickness using a surgical sterile blade and scissors under ketamine anesthesis. Each group of diabetic rats received inoculation of 400 μl aliquots of MDR AB 38 suspension in different densities (104–109 colony forming unit [CFU]) onto the wound. The animals were observed for 100 hr. Sequential cultures were done on all animals by collecting pus samples. Gram stain and culture were done by using the pus. Grading of inflammatory cells was done by Clinical Microbiology Proficiency-Testing (CMPT) method. 7
Excision wound model for studying therapeutic effect of A. baumannii phage 38 in diabetic rats
The rats were randomly divided into five groups of six animals each. The wound excision was done by following the same procedures that were used to evaluate the minimum infection dose.
Groups
Bacteriological evaluation of the wound
Swabs were taken on day 2 to confirm the presence of the MDR AB 38 in the pus by doing Gram stain. From day 2 onward, successive sampling of the wound surface was done for culture and Gram stain till day 20 and phage count was evaluated in Group II and Group V. Blood culture was done for the animal that showed moribund status. Grading of pus for inflammatory cells was done by CMPT method. 7 Cellular infiltration was graded as 0 for absence, 1 for rare (occasional presence), 2 for few, 3 for moderate, and 4 for many.
Quantification of bacterial load in the wound
Samples collected from the wound were homogenized by vortexing for 1 min and centrifuged at 3,000 rpm for 10 min. 0.1 ml of sample was diluted in 0.9 ml of 0.9% sterile saline solution with final log dilutions of 10−1, 10−2, 10−3, 10−4, 10−5, and 10−6. The samples were then plated on sheep blood agar and MacConkey agar by using a 4 mm Nichrome wire loop (Hi-Media), which holds 0.01 ml of solution. All plates were incubated overnight at 37°C. Plates were incubated for 18–24 hr at 37°C.1,22
Phage titer
Samples from the phage-treated rats were homogenized and then filtered through a 0.22 μm pore size membrane (Acrodisk; Pall German Laboratory). The phage titer in the filtrates was determined using a soft agar overlay using MDR AB 38 as the host. 23 The resulting plaques were counted with the ProtoCol plate counter, and phage titer was calculated.
Wound contraction rate
Contraction of the wound was noted by following the progressive changes in wound area planimetrically. The size of the wounds was traced on a transparent paper every 2 days, throughout the monitoring period. The tracing was then transferred to a 1 mm two graph sheet, from which the wound surface area was evaluated.9,18
Period of epithelialization
Period of epithelialization was noted as the number of days after wound healing required for the eschar to fall off, leaving no raw wound behind.9,18
Statistical analysis
The results were analyzed using one-way ANOVA followed by Tuckey's post hoc test.
Results
Diabetic rats
Alloxane-induced diabetic rats showed a fasting blood sugar level more than 300 mg/dl and a glycosylated hemoglobin level more than 7.2%.
Acinetobacter phage antibacterial activity
Acinetobacter phages isolated from the sewage water had a plaque size ranging from 1 to 7 mm in diameter. The Acinetobacter phage was found to form plaques on MDR AB 38. The phage isolated formed plaques on 57.1% of beta-lactamases producing A. baumannii isolated from diabetic foot infection.
Electron microscopy
The Acinetobacter phage had an icosahedral head, about 80 nm in diameter, and a 100-nm long tail, thus morphologically similar to phages belonging to Siphoviridae family. 16
Minimum infection dose of MDR AB 38
Rats inoculated with MDR AB 38 with 108 CFU established infection and showed significant pus within 48 hr. Clinically, the animals were moribund, lethargic with ruffled hair. For all other work, 108 CFU of MDR AB 38 was taken as an infective dose to evaluate therapeutic utility of Acinetobacter phage in the rat model.
Excision wound
Gram stain and culture
Grading of Gram stain was done as per CMPT scale 7 and depicted in Table 1.
Grading of pus for inflammatory cell was done by CMPT method. 7 Cellular infiltration was graded as 0 for absence, 1 for rare (occasional presence), 2 for few, 3 for moderate, and 4 for many.
CMPT, Clinical Microbiology Proficiency-Testing.
Group I
Gram stain and culture did not reveal any bacteria from the swabs collected from day 2 till the end of the experiments.
Group II (infected and challenged with phage)
Swabs collected on day 2 revealed more neutrophils (Grade 4) along with Gram-negative bacilli, and culture revealed growth of MDR AB 38. Inflammatory cells reduced on day four and six (phages were administered after 48 hr), Bacterial load increased on day 4 (8.93 log10), and it reduced on day 6 (3.34 log10) (Table 2). No bacteria were cultured on day 8. Subsequent swabs did not reveal presence of any inflammatory cells or bacteria, and culture did not show growth for MDR AB 38.
SD, standard deviation.
Group III (unchallenged group)
Gram stain and culture from the swab collected on day 2 revealed Gram-negative bacilli along with many inflammatory cells (Grade 4) (Table 1). Subsequent swabs on day 4 revealed more neutrophils along with Gram-negative bacilli, and culture revealed growth of MDR AB 38. Blood culture revealed growth for MDR AB 38. All rats died on the eighth day. Bacterial load increased from 7.57 log10 to 9.10 log10 (Table 2).
Group IV (infected and challenged with antibiotic)
Gram stain and culture revealed the presence of bacteria and inflammatory cells from the swabs collected from day 2. Antibiotic was administered after 48 hr. Culture swab on day 4 and 6 showed an increase in bacterial load (8.91 log10 and 8.96 log10) along with increased inflammatory cells (Grade 4). Animals were clinically moribund on day 6. Swab collected on the eighth day showed a slight decrease in bacterial load (7.36 log10) and the inflammatory cells of Grade 3, but the clinical condition of the rats improved on day 8 compared with day 6.
On day 10, the clinical conditions of the rats were better compared with on the eighth day; the number of inflammatory cells (Grade 2) was fewer; and bacterial load dropped from 7.36 log10 to 4.93 log10 (Table 2). No bacteria were cultured from day 16 onward.
Group V
Gram stain and culture did not reveal growth for MDR AB 38 from the swabs collected from day 2 to 20.
Wound contraction
The mean area of wound contraction is shown in Table 3. The percentage of wound contraction was 5.9, 20.2, 23.6, 40.7, 71.4, and 82.0 as measured on the 4th, 6th, 8th, 10th, 12th, and 14th day correspondingly in Group I (Fig. 1). The rate of wound contraction changed significantly in groups on the 4th, 6th, 8th, 10th, 14th, and 16th day as compared with Group I at the same intervals (Fig. 1). Apart from this, we also observed a positive trend in wound contraction rate in phage-treated groups from day 4 onward and in the antibiotic-treated group from day eight onward. In Group III, wound contraction was in negative trend till day 6 and all the animals died on day eight. These observations are statistically significant on all the days when compared with homogenous groups. However, wound contraction rate favorably increased in the phage-treated group compared with Group IV. The percentage of wound contraction in the phage-challenged group was 2.4, 20.7, 22.5, 40.9, 70.8, and 81.4 on the 4th, 6th, 8th, 10th, 12th, and 14th day, respectively; whereas in the antibiotic-challenged group (Group IV), the percentage of wound contraction was −20.5, −13.3, 6, 28.9, 46.4, and 65.8 on the same days as mentioned earlier (Table 3).
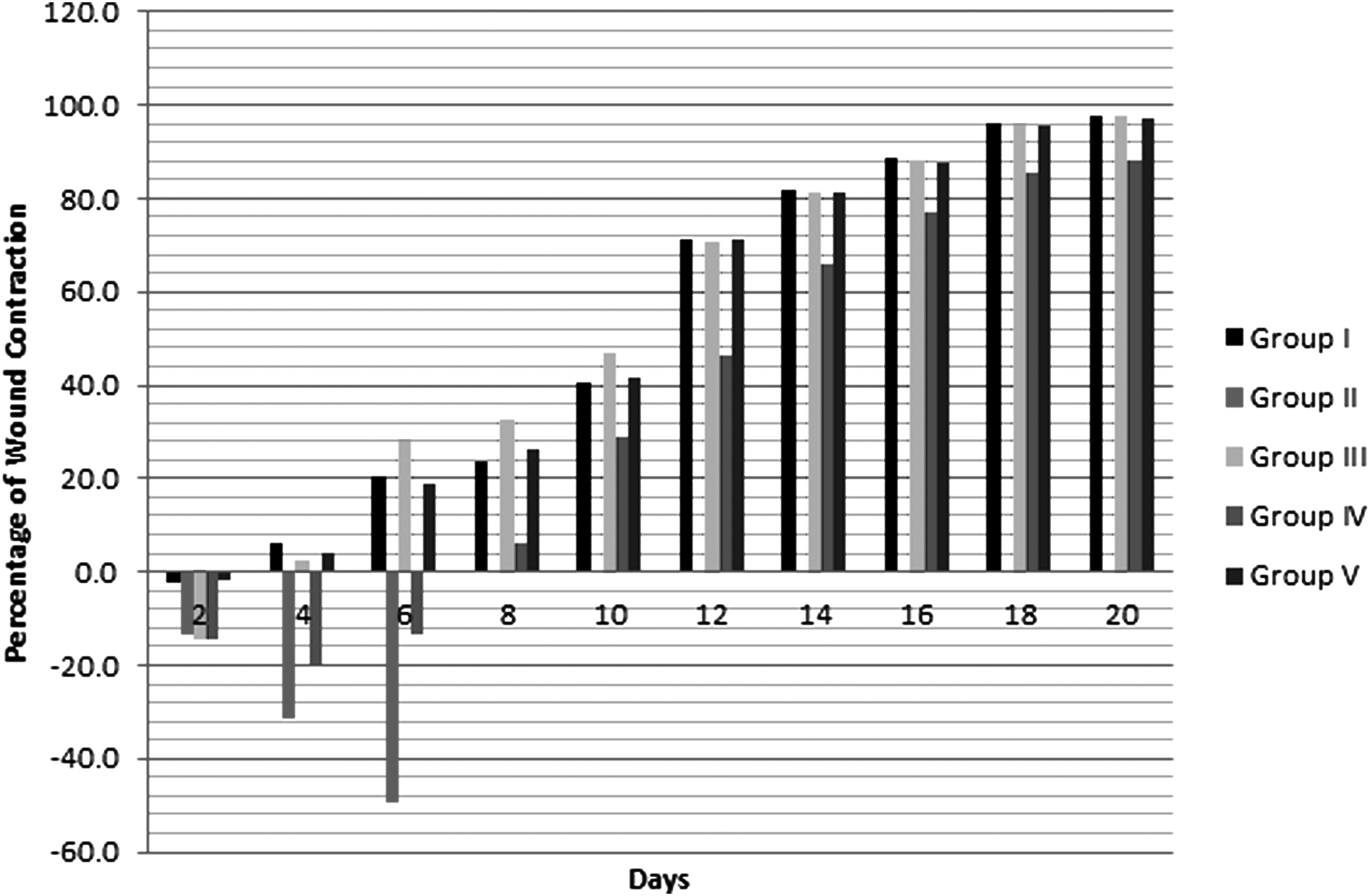
Effect of bacteriophage on percentage of wound contraction in excision wound in uncontrolled diabetic rats infected with multidrug-resistant (MDR) Acinetobacter baumannii.
One-way ANOVA test.
Tukey's post hoc test.
MDR AB, multidrug-resistant Acinetobacter baumannii.
The mean period of epithelialization was found to decrease significantly in the phage-treated group (23.4±1.08 days) compared with other groups. The duration of epithelialization in the antibiotic-treated group did not differ significantly when compared with the phage-treated group and control group. The mean±SEM of the number of days required for epithelialization in Group I was 23.5±0.99; in Group V, the duration of the epithelialization was 23.8.±0.15; and in Group IV, the epithelialization was 25.8±2.45 (data not shown in the table).
Phage titer
The phage titer was determined in Group II and Group V. In Group II, the phage count was 1.67×1014 PFU/ml, 8.92×1010 PFU/ml, 3.54×103 PFU/ml, and less than 32 PFU/ml on the 4th, 6th, 8th, and 10th day, respectively (Table 4).
PFU, plaque forming unit.
In Group V, no phages were recovered from day 2 onward.
Discussion
Since the dawn of the antimicrobial drug era, resistance has shadowed the success of infectious disease therapy. Barring the arrival in the near future of new antimicrobial drugs that are effective against disparate organisms, we are left with imperfect tools to control drug resistance, with notable exception. Infection control in health-care settings, which is essential for preventing transmission of susceptible and resistant microorganisms alike, remains imperfect. Reducing the discretionary use of antimicrobial drug when possible is helpful but even if we use these drugs with exquisite precision, resistance will continue to evolve and spread. 3 The statistics compiled as a result of surveillance efforts exemplify the emergence of many genera of bacteria that are resistant to all antibiotics. The genus Acinetobacter epitomizes this drift and deserves close attention. 17 Acinetobacter spp exhibit mechanisms of resistance of all existing antibiotics classes as well as a prodigious capacity to acquire new determinants of resistance. 3 Antimicrobial resistance greatly limits the therapeutic options for patients who are infected with this organism, especially if isolates are resistant to the carbapenem class of antimicrobial agents. Since therapeutic options are limited for MDR Acinetobacter infection, the development or discovery of new therapies, well-controlled clinical trials of existing antimicrobial regimens and combinations, and greater emphasis on the prevention of health-care-associated transmission of MDR Acinetobacter infections are essential. An alternative or supplement to antibiotic therapy, which is currently being re-examined, is the use of bacterial viruses (phage/bacteriophage) to target bacterial infections, that is, phage therapy. The A. baumannii isolate used in this study is ESBL and MBL producer. The phage isolated formed plaques on ESβL and MβL producing A. baumannii isolated from diabetic foot infection, suggesting a wide spectrum of antibacterial activity of the isolated bacteriophage.
An in vivo experiment was done to evaluate therapeutic potential of phages specific for A. baumannii to resolve wound infection in uncontrolled diabetic rats. Wound is a disruption in the continuity of the living tissues. Wound repair or regeneration or sometimes both lead to wound healing. 18 The various phases of wound healing are inflammation, angiogenesis, epithelialization, collagenation, wound contraction, and so on.9,18 In the excision wound model in rats, phages significantly reduced the duration of epithelialization and increased the percentage of wound contraction. No literature on use of bacteriophage to study wound-healing properties in uncontrolled diabetic rats is available to compare our results. Phage therapy is not a substitute for antibiotic therapy, and the simultaneous use of localized phage and systemic antibiotics can have additive or synergistic effects. However, local administration of some antibiotics can interfere with phage therapy by killing the more accessible target bacteria in ways that block their ability to serve as phage “factories” but still permit phage adsorption and injection, which is, thus, suicidal to the applied phages. If no generalized infection or its danger is present, the treatment of purulent wounds can be carried out as a monotherapy, that is, without antibiotic augmentation. Hence, in this study, the infected wound was treated with the phages alone, not in combination with antibiotics. However, a study carried out by Steven et al. 24 found encouraging results in rodents infected with Pseudomonas aeruginosa and treated with filamentous phages Pf3 and Pf1 along with a low concentration of antibiotic gentamicin and concluded that simultaneous use of localized phage and systemic antibiotics can have additive or synergistic effects.
In this study, the wounds were debrided before the application of the bacteriophage. A study carried out by Joao et al., 12 indicated that topical application of bacteriophage in debrided infected wounds was very effective against S. aureus, P. aeruginosa, and A. baumannii in rodents and less effective in the porcine model.
In rat experiments, Group II, Group III, and Group IV rats were infected with 108 CFU of MDR AB 38. After 2 days, all rats in Group II, III, and IV that had received bacteria produced abscess. The rate of wound contraction was in negative trend. At the end of the eighth day, all the rats in Group III died. In the phage control group, after day 4, the rats did not produce abscess, indicating that phages did not initiate infection in the wound.
In the phage-challenged group, no bacteria were isolated from the abscess after 6 days, indicating that Acinetobacter phage has cleared all the MDR AB 38 present in the abscess. However, in the antibiotic-challenged group, bacteria could be demonstrated in the abscess till 14 day. However, the timing of treatment is crucial for acute infections but is less crucial in chronic infections where the infectious bacterial population is found in abundance. Acinetobacter phage was cultured from all those rats that received bacteria and phage (Group II). More phages were recovered than the administered dose; this, to our awareness, is the first direct substantiation of administered phage multiplying in the tissues infected by Gram-negative bacteria. However, in Group V, the phage was not cultured, indicating that phage-specific bacteria are required for propagation of the phages.
Except the Group IV rats, the rats in other groups not only survived, but also complete epithelialization of the wound was observed and the duration of epithelialization was significantly shorter in the phage-treated group compared with the antibiotic-treated group.
Conclusion
Despite a reputation for relatively low virulence, MDR Acinetobacter infection poses a formidable threat to patients. The cause of many outbreaks, this organism is increasingly endemic in health-care settings. Antimicrobial resistance is increasing, likely as a result both of the emergence of resistance in the context of antimicrobial pressure and of health-care-associated transmission of drug-resistant strains. In this study, we were able to demonstrate phage prophylaxis against experimental MDR A. baumannii infections in uncontrolled diabetic rats similar to those that are common in humans. There was no evidence of general sepsis, and the rats, including phage controls, appeared remarkably well.
The potential of phage therapy has been the subject of several recent reviews, and this study reinforces the view that this potential is worth exploring when there are limited options for treatment.
Footnotes
Disclosure Statement
The authors declare that there are no conflicts of interest.