
Abstract
The aim of this study was to investigate the infections due to OXA-48 carbapenemase-producing bacteria in tertiary hospitals in Kuwait (September 2011 to April 2013) and to determine the sequence types (STs) of the corresponding isolates. Eleven OXA-48 carbapenemase-producing Enterobacteriaceae isolates were recovered from patients treated in nine different hospitals in Kuwait. Susceptibility testing to eighteen antibiotics was done using the E-test. PCR assays were performed for the detection of genes encoding extended-spectrum β-lactamases (ESBLs) (blaCTX-M, blaSHV, and blaTEM) and carbapenemases (blaOXA-48, blaVIM, blaNDM, blaIMP, blaGIM, and blaKPC). STs were determined by Multilocus Sequence Typing. Seven Klebsiella pneumoniae, two Escherichia coli, one Enterobacter cloacae, and one Morganella morganii harbored the blaOXA-48 gene. The K. pneumoniae and E. coli belonged to seven and two different STs, respectively, which were not related to those reported from this region. The majority of the isolates carried either blaCTX-M or blaSHV genes and showed a multidrug-resistant phenotype, including resistance to tigecycline. Multidrug-resistant Enterobacteriaceae harboring the blaOXA-48 gene are emerging in Kuwait with different STs compared to those identified in other countries of the region. Detection of OXA-48-producing Enterobacteriaceae in Kuwait is important to prevent its rapid spread.
Introduction
E
Carbapenem resistance in Enterobacteriaceae is emerging and it is mostly related to the production of carbapenemases. In addition, carbapenem resistance may be due to other resistance mechanisms such as porin loss in combination with AmpC and/or extended-spectrum β-lactamase (ESBL) production.8,11,15,27 Carbapenemases are enzymes that hydrolyze the great majority of β-lactam antibiotics. 15 They are diverse and belong to Ambler class A (e.g., Klebsiella pneumoniae carbapenemase; KPC), class B (e.g., imipenemase; IMP, Verona intergron-encoded metallo-β-lactamase; VIM and New Delhi metallo-β-lactamase; NDM), or class D (OXA-48 and its variants). 17
OXA-48 carbapenemase was first isolated from a clinical K. pneumoniae strain in Istanbul, Turkey, in 2001. The gene encoding this carbapenemase originated from the environmental Shewanella spp., in which it was chromosomally encoded.20,21 Subsequently, OXA-48-producing bacteria have been reported from many countries in Europe, the Middle East, North Africa, and Japan.9,23,33 In 2013, OXA-48 producers were reported in North America,12,13 while the closely related OXA-163 and OXA-181 carbapenemase-producers have been reported in South America and India, respectively. 23 Enterobacterial isolates producing OXA-48 have even been found in the final effluent of wastewater treatment plant 29 and from pet dogs in Germany. 28 The blaOXA-48 gene, encoding the enzyme, has been detected in different Enterobacteriaceae genera. 23 The spread of the blaOXA-48 gene is usually associated with Tn1999-like transposons, which are inserted into an epidemic 62-kb IncL/M-type plasmid. 23
Recent reports have highlighted the occurrence of OXA-48-producing isolates in infected patients in some of the GCC (Gulf Cooperation Council) countries (i.e., Saudi Arabia, Oman, UAE, and Qatar)5,7,33 An OXA-48-producing K. pneumoniae has also been reported from a screening rectal swab culture of a patient transferred from Kuwait to France for medical treatment. 19 The aim of the current study was to investigate the occurrence of OXA-48-like producers among enterobacterial isolates recovered from infected hospitalized patients in nine different tertiary hospitals in Kuwait and to determine their STs.
Materials and Methods
The isolates originated from nine major public hospitals in Kuwait serving the catchment areas of the majority population (Adan, Al Razi, Amiri, Jahra, Farwaniya, Ibn Sina, Maternity, Mubarak Al kabeer, and Sabah hospitals) were included in the study during the period, September 2011 to April 2013. A total of 1335 patients had growth of Enterobacteriaceae in their clinical specimens. Only one isolate per patient was used and if a patient had more than one isolate, only the first one was selected. Isolates from 66 patients were carbapenem resistant (CRE-for carbapenem-resistant Enterobacteriaceae) with a prevalence rate of 4.94%. Even though there is no national reference laboratory for antimicrobial resistance in Kuwait, data generated from research projects such as ours are used to formulate the national antibiotic policy guidelines.
Bacterial isolates
These 66 isolates were nonsusceptible to at least one of the carbapenems with a minimum inhibitory concentration (MIC) >1 mg/L for imipenem or meropenem, or >0.5 mg/L for ertapenem, according to the Clinical and Laboratory Standards Institute (CLSI), 2012. 3 They were stored at −70°C in 1% protease/peptone broth containing 7% glycerol for further evaluation. Species identification was initially performed with the VITEK II automated system (bioMérieux, Marcy l'Etoile, France) and then, when necessary, confirmed by VITEK MS (bioMérieux).
Antimicrobial susceptibility testing and phenotypic assays
Initial antibiotic susceptibility was performed using the VITEK II system with AST GN09 cards (bioMérieux). MICs for 18 antibiotics were determined by the E-test (bioMérieux) according to the manufacturer's instructions. The tested antibiotics were amikacin and gentamicin (aminoglycosides); ampicillin, amoxicillin–clavulanic acid, and piperacillin (β-lactam); aztreonam (monobactam); cefalothin, cefepime, cefotaxime, cefoxitin, ceftazidime, and cefuroxime (cephalosporins); ciprofloxacin (quinolone); colistin (polymyxin); ertapenem, imipenem, and meropenem (carbapenems); and tigecycline (glycylcycline). Susceptibility testing was interpreted according to the CLSI recommendations, 3 except for tigecycline and colistin. For tigecycline, we used the breakpoints recommended by the Food and Drug Administration, USA, that is, susceptible if MIC of ≤2 mg/L and resistant if MIC of ≥8 mg/L. For colistin, the breakpoints recommended for Acinetobacter spp. were used (i.e., MIC of ≤2 mg/L for susceptible and MIC of ≥4 mg/L for resistant). 3 Escherichia coli ATCC 25922 and E. coli ATCC 35218 strains were used as controls. Preliminary screening for the presence of carbapenemase was done by the modified Hodge test (MHT) 3 and E-test according to the manufacturer's instructions (bioMérieux). K. pneumoniae ATCC BAA-1705 and ATCC BAA-1706 were used as positive and negative controls, respectively.
PCR amplifications and sequencing
PCR assays were used to amplify the extended-spectrum β-lactamases (ESBLs) genes blaCTX-M, blaSHV, and blaTEM, 26 and the carbapenemase genes blaOXA-48, blaVIM, blaNDM, blaIMP, blaGIM, and blaKPC. 24 Sequencing was performed using a GenAmp PCR system 9700 by cycle sequencing with BigDye termination (AB Applied Biosystem, Carlsbad, CA).
Pulsed-field gel electrophoresis
Pulsed-field gel electrophoresis (PFGE) was performed with endonuclease XbaI (New England BioLabs, Ipswich, MA) to restrict genomic DNA of OXA-48-positive isolates, and electrophoresis was performed with the CHEF-DR III system (Bio-Rad, Hemel Hempstead, United Kingdom). Electrophoresis conditions were pulse times ranging from 5 to 45 sec for 20 hr at 6 V/cm at 14°C. Restriction patterns were analyzed according to previously described criteria. 30
Multilocus sequence typing
Multilocus sequence typing (MLST) was used to assess the relatedness of E. coli and K. pneumoniae isolates using standard primers and protocols. 6 Allele sequences and sequence types (STs) were defined with reference to the Pasteur scheme (www.pasteur.fr/recherche/genopole/PF8/mlst) for K. pneumoniae, and the University College Cork (UCC), Ireland scheme for E. coli (www.mlst.ucc.ie/mlst/dbs). A novel allelic profile and novel allele patterns were sent to the curators of the Pasteur scheme to assign novel ST designations. MLST was not done for species belonging to other genera.
Results
Bacterial isolates
Of the 66 CRE isolates, 11 were positive for blaOXA-48. The clinical features and patient characteristics are shown in Table 1. The ages ranged from 2 months to 90 years (mean=49.8 years). All were long-term residents in Kuwait. The gender ratio was similar. Treatment modalities varied from monotherapy to treatment with as many as five antibiotics. Nine of 11 patients survived with a mortality rate of 18.1%. One patient died due to sepsis and another due to meningitis.
BP, hypertension; DVT, deep venous thrombosis; IHD, ischemic heart disease; CVA, cerebrovascular accident; DM, diabetes mellitus; UTI, urinary tract infection; BPD, bronchopulmonary dysplasia; IVH, intraventricular hemorrhage; EVD, external ventricular drain; RTA, road traffic accident; NK, non-Kuwaiti with unknown nationality; AK, amikacin; PM, cefepime; CO, colistin; CTX, cefotaxime; CRO, ceftriaxone; AMP, ampicillin; VAN, vancomycin; TZ, ceftazidime; CI, ciprofloxacin; CLAR, clarithromycin; MP, meropenem; TAZ, piperacillin–tazobactam.
Table 2 shows the different sources of the isolates—six from urinary tract infection (UTI), three from skin and soft tissue infections (gastrostomy wound and infected umbilicus of a cancer patient), one from endotracheal secretion of a patient with pneumonia, and one from the cerebrospinal fluid of a patient with meningitis. They were the following: K. pneumoniae (n=7), E. coli (n=2), Morganella morganii (n=1), and Enterobacter cloacae (n=1). All the Egyptians and the Indian had a recent history of travel to their native countries within the previous 1–3 months before admission to hospital. The Kuwaiti patients did not have a history of recent travel overseas.
CSF, cerebrospinal fluid; WS, wound swab.
Susceptibility testing
The results of susceptibility testing are shown in Table 3. According to CLSI criteria, 3 all isolates showed a high-level resistance (MIC >256 mg/L) to ampicillin, amoxicillin–clavulanic acid, cefalothin, cefuroxime, and piperacillin (data not shown in Table). Eight, six, and five isolates were resistant to ertapenem, imipenem, and meropenem, respectively; six isolates were resistant to cefepime (MICs 12- >256 mg/L), seven to cefoxitin (MICs 12- >256 mg/L), eight to ceftazidime (MICs 6- >256 mg/L), and nine to cefotaxime (MICs 3- >256 mg/L); five isolates were resistant to aztreonam and gentamicin, but only a single isolate (K. pneumoniae) showed resistance to amikacin; six isolates were resistant to ciprofloxacin and cefepime. All except the M. morganii isolate were susceptible to colistin and only three isolates (M. morganii, K. pneumoniae, and E. cloacae) were susceptible to tigecycline. All isolates were positive for carbapenemase with the modified Hodge test, but all gave negative results with the metallo-β-lactamase (MBL) E test.
The values in parentheses in the first row are the recommended breakpoints for resistance according to Clinical Laboratory and Standards Institute. 3
AT, aztreonam; PM, cefepime; FX, cefoxitin; ETP, ertapenem; GM, gentamicin; IP, imipenem; MIC, minimum inhibitory concentration; MP, meropenem; TG, tigecycline.
Detection of ESBL and carbapenemase
The blaOXA-48-positive isolates were negative for blaNDM-1, blaVIM, blaKPC, blaGIM, and blaIMP genes. Among these 11 isolates, nine coproduced ESBLs (Table 2); blaCTX-M was detected in six of these isolates and blaSHV gene was detected in five. Among the different CTX-M variants, those belonging to CTX-M-15 and CTX-M-14 groups accounted for 66.6% (n=4; 3 K. pneumoniae and 1 E. coli) and 33.3% (n=2; K. pneumoniae), respectively. The other ESBL determinant, SHV-11 was detected in two K. pneumoniae, while SHV-1 production was detected in three K. pneumoniae isolates. In addition, two isolates harbored both the blaCTX-M and blaSHV genes. Three ESBL-producing isolates (2 K. pneumoniae and 1 E. coli) were susceptible to ceftazidime and two to cefotaxime. However, one K. pneumoniae and one E. coli were ESBL negative.
Clonal relationship
PFGE analysis showed that the seven K. pneumoniae and the two E. coli isolates had distinct patterns and therefore were not clonally related to one another (Fig. 1).
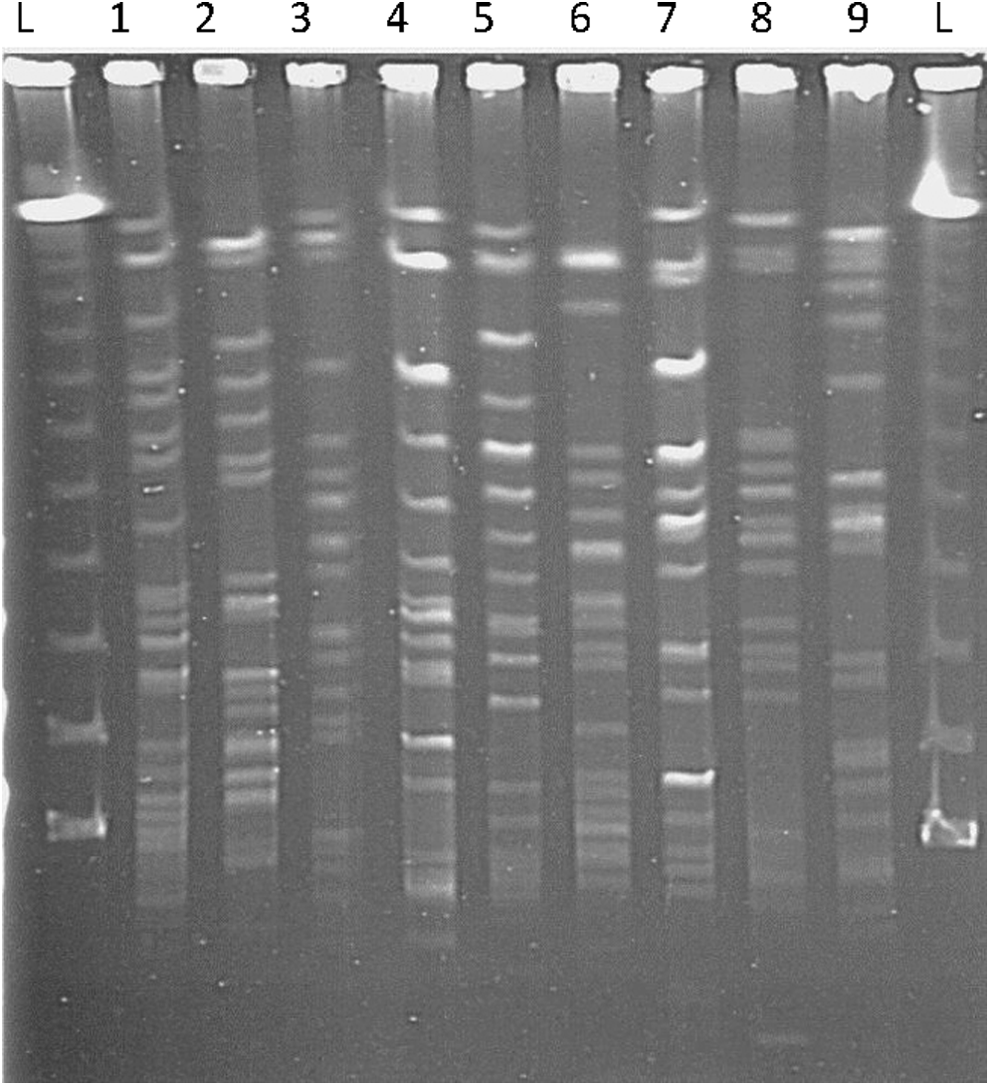
PFGE pattern of OXA-48 positive of Klebsiella pneumoniae and E. coli after digestion with XbaI. Lane L=λ ladder (Bio-Rad); lane 2=KEC3=Escherichia coli strain 3; lane 3=KEC69=E. coli strain 69; lane 4=KKP156=K. pneumoniae strain 156; lane 5=KKP33=K. pneumoniae strain 33; lane 6=KKP83=K. pneumoniae strain 83; lane 7=KKP38=K. pneumoniae strain 38; lane 8=KKP68; K. pneumoniae strain 68; lane 9=KKP55=K. pneumoniae strain 55. PFGE, pulsed-field gel electrophoresis.
Determination of the STs
MLST analysis performed on all the E. coli and K. pneumoniae isolates revealed that the K. pneumoniae isolates belonged to seven different ST types, namely ST677, ST16, ST107, and ST485, while three ST types were new and were not listed in the Pasteur Institute MLST scheme (Table 4). They were given new designations as ST1593, ST1592, and ST1594 by the Pasteur Institute. The E. coli isolates belonged to ST405 and ST38.
gapA, glyceraldehyde 3-phosphate dehydrogenase; infB, translation initiation factor 2; mdh, malate dehydrogenase; pgi, phosphoglucose isomerase; phoE, phosphorin E; rpoB, beta subunit of RNA polymerase; tonB, periplasmic energy transducer; *, new allele.
Discussion
The emergence of CRE is an important public health problem as this phenomenon may lead to untreatable infections. 17 Reports of OXA-48 carbapenemases have been published worldwide, including the GCC countries, for example, Saudi Arabia, Sultanate of Oman, Qatar, and UAE,4,7,33 and the West Asian countries, for example, Turkey, Egypt, Tunisia, Morocco, Libya, Lebanon, and Israel.1,23 In our study, 9/11 isolates coexpressed ESBLs as reported previously.7,31,33
In this current report, about 55% and 46% of our isolates were susceptible to meropenem and imipenem, respectively (with MIC <1 mg/L), according to the CLSI guidelines. 3 Therefore, it is difficult to suspect OXA-48 production in isolates exhibiting only a slight increase in carbapenem MICs. A similar observation has been made previously. 7 By contrast, only 27.3% of the OXA-48-positive isolates remained susceptible to ertapenem, which therefore appears to be a better indicator compared to imipenem or meropenem susceptibility. Noteworthy that Huang et al., 2014, recently highlighted this observation. 10 Therefore, screening for ertapenem resistance has been proposed as the most sensitive marker for detection of CRE. 5
Eight and nine of our OXA-48-producing stains were resistant to ceftazidime and cefotaxime, respectively. This may be explained by the coexistence of ESBLs in the majority of our isolates, which coproduced either CTX-M or SHV enzymes. This may reflect the variable hydrolysis of ESBL in OXA-48-producing K. pneumoniae.2,21 Therefore, their use for empirical treatment of infected patients should not be encouraged. In a routine clinical microbiology laboratory, cefotaxime and ceftazidime should be tested regularly as the guidelines emphasize their use as first-line therapy and not carbapenems. However, experimental peritonitis in mice due to K. pneumoniae-producing OXA-48 carbapenemase has been treated successfully with ceftazidime with a good outcome provided that the strain does not produce ESBLs or AmpC cephalosporinase. 14 In addition, ceftazidime has been found to be effective in a murine infected model with OXA-48-producing K. pneumoniae. 32
In our study, ST analysis was performed only on E. coli and K. pneumoniae isolates. Among the K. pneumoniae isolates, seven different STs were identified from nine different Kuwaiti hospitals. Four STs have been previously identified in other countries such as Sweden, France, and Poland. However, three isolates could not be assigned to any known STs and these represented novel STs. One isolate, K. pneumoniae ST16, was similar to the K. pneumoniae found in Turkey. 23 It is interesting to note that these STs are different from the ones circulating in the nearby GCC countries (K. pneumoniae ST753, ST754; E. coli ST138, ST648 circulate in these countries) and the rectally colonized isolate from a Kuwaiti patient treated in France (K. pneumoniae ST743).7,19 The two carbapenemase-producing E. coli in our study belonged to ST38 or ST 405. It is noteworthy that OXA-48-producing ST38 E. coli that emerged in France 22 and subsequently reported from numerous other countries, 25 appears to be a successful clone. Also, an OXA-48-producing E. coli from a patient in Egypt belonged to ST38, 23 similar to one of the isolates in our study.
The occurrence of OXA-48-producing Enterobacteriaceae in the nine major hospitals in Kuwait is of great concern. The use of the SUPERCARBA selective medium 16 and rapid identification of carbapenemase production by using the Carba NP test are highly recommended for rapid detection of OXA-48-producing strains. 18
In conclusion, we showed the epidemiology of OXA-48 in Kuwait. We believe that our findings are just the tip of the iceberg and we recommend strict implementation of infection control policies in hospitals to prevent the spread of these strains.
Footnotes
Acknowledgments
Disclosure Statement
No competing financial interests exist.