
Abstract
Introduction
T
Case Report
In this study, we describe the case of a 24-year-old female who presented to the Walk-In/Urgent Care department of Urban Health Plan (Fig. 1) with folliculitis of both buttocks and furuncles on the left hip and right lateral thigh. She denied history of fever, malaise, nausea, vomiting, or fatigue. She had no comorbid conditions, did not take medications, and had no history of food or environmental allergies. She had no recollection of previous SSTIs or recent trauma to the lower extremities. She reported living in an apartment with a male partner, two school-aged children, and her sister. There were no pets in the home. The patient originally came to New York from Puerto Rico but had not recently traveled out of the New York metropolitan area.

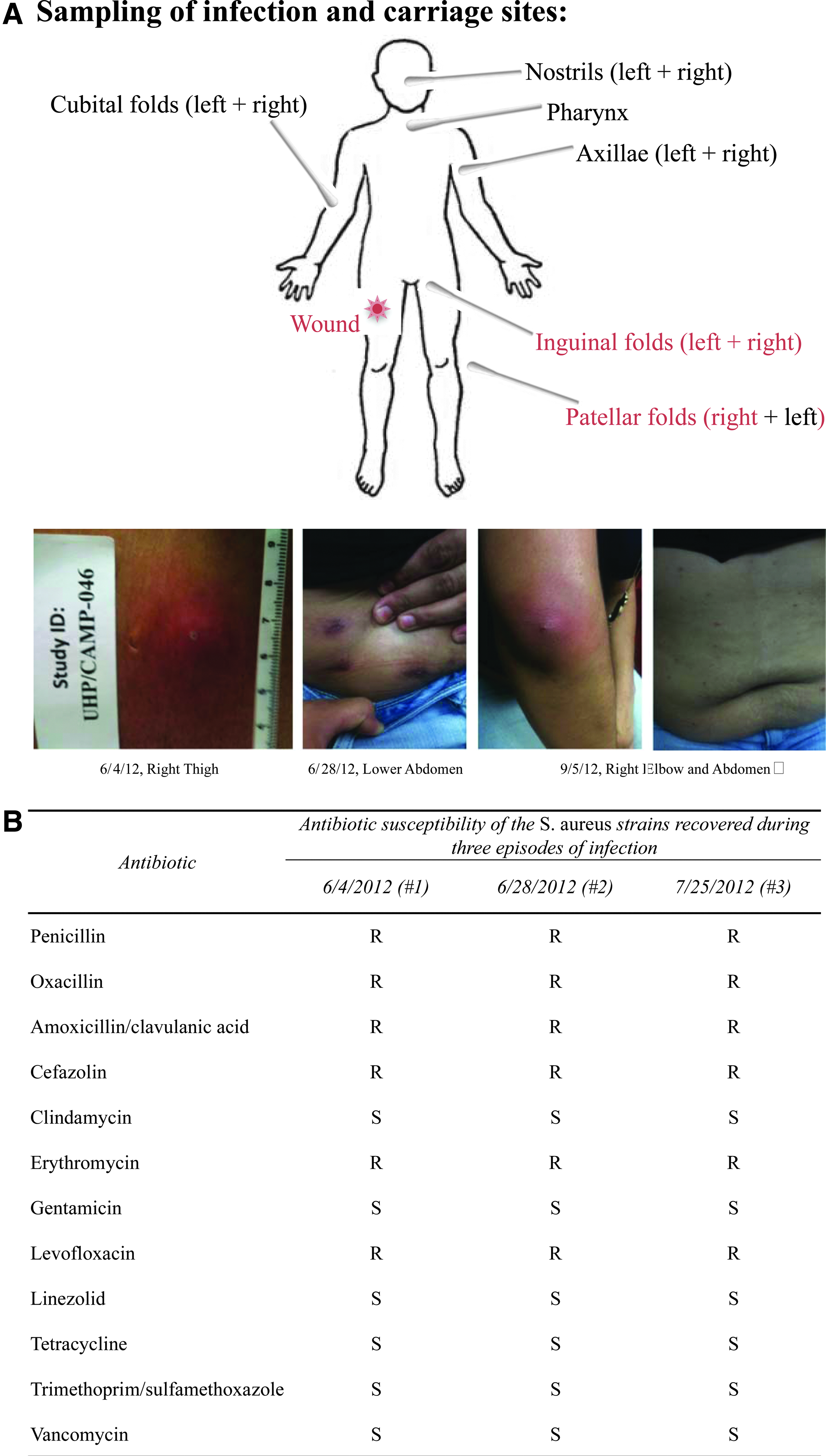
History of recurrent skin infections caused by a methicillin-resistant Staphylococcus aureus (MRSA) strain belonging to the USA300 clone. TMP/SMX, trimethoprim/sulfamethoxazole.
The furuncles were incised, drained, and cultured. Surveillance cultures were obtained from the following sites: nostrils, pharynx, axillae, and cubital, inguinal, and patellar folds (Fig. 2A). Specimens from the right lateral thigh furuncle and left and right inguinal folds were positive for MRSA; sensitivity testing revealed that all strains were susceptible to trimethoprim/sulfamethoxazole (TMP-SMX), and the patient was prescribed oral TMP-SMX (Fig. 2B).
Two days later, the patient returned with complaints of worsening pain and swelling at the incision sites, generalized malaise, and chills, and reported antibiotic compliance. Physical examination revealed cellulitis at the left hip incision site, and two new furuncles at the right posterior thigh and hip. She was transferred to a local hospital, where she received intravenous vancomycin and underwent two additional incision and drainage (I&D) procedures. During her hospital stay, she had negative blood cultures and an urticarial reaction presumed to be secondary to the administration of vancomycin. She was discharged after 48 hours and returned to the CHC 2 days later, where she was directed to complete a 10-day course of oral TMP-SMX. The patient was seen for follow-up 1 week after hospital discharge and the physical examination revealed resolution of lesions and symptoms.
Twenty-two days after the initial visit, the patient returned with furuncles on the lower abdomen and folliculitis on the posterior thighs. The furuncle, nostrils, pharynx, axillae, and the cubital, inguinal, and patellar folds were cultured. MRSA was again detected in the wound, groin area, and now also in the right patellar fold, but not in the nares.
Over the next 3 months, the patient presented with three additional episodes of SSTIs (Fig. 1). Each time she was treated with the I&D procedure and a 7–10-day course of TMP-SMX, and treatment resulted in clinical resolution. The patient was instructed to bathe daily with chlorhexidine soap. The MRSA strain responsible for the recurrent infections appears to be identical, as judged by the antibiotype and similar clinical presentation.
Three months after the initial presentation (Fig. 1), the patient returned with folliculitis of the abdomen and an abscess proximal to her right elbow. The patient refused another I&D procedure and requested a different antibiotic regimen. She received a 30-day supply of doxycycline based on prior antibiograms and was instructed to apply warm compresses to promote drainage. She returned 3 weeks later and was reportedly symptom free and satisfied with her clinical outcome.
Upon further examination, the patient reported that the sister who had been residing with her had developed an SSTI, for which she underwent I&D and received antibiotics at a local emergency department around the same time as the patient's initial presentation. The sister subsequently moved out of the patient's apartment and according to our patient, she did not experience any recurrence. The patient's children and partner did not develop SSTIs at any time.
Materials and Methods
Sampling
The three I&D samples were sent to a clinical laboratory (Bio-Reference Laboratories, Inc., Elmwood Park, NJ) for identification, speciation, and antibiograms by MICROSCAN.
Samples from the wound and 11 body sites were collected with sterile swabs at the first presentation and again during follow-up consultation 1 month later and were transported to the Laboratory of Microbiology and Infectious Diseases at The Rockefeller University for molecular characterization.
Molecular typing
The samples were grown in Triptic Soy Broth at 37°C overnight and plated on Mannitol Salt Agar for 48 hours at 37°C. Yellow colonies were selected to perform the coagulase test. Positive isolates to both the mannitol and coagulase tests were further characterized by molecular typing. Pulsed-field gel electrophoresis (PFGE) was performed on all S. aureus isolates 2 and the resulting SmaI restriction band profiles were analyzed by visual inspection 15 ; spa types were assigned through the Ridom webserver (http://spaserver.ridom.de). 1 Multilocus sequence typing was conducted.8,3 PCRs were performed to detect pvl, 31 arginine catabolic mobile element (ACME), 6 and to type the SCCmec cassette.17,18
Results
S. aureus was identified in the two wounds and groin area, as well as in the right patellar fold during the second SSTI episode. Isolates were resistant to beta-lactams, erythromycin, and levofloxacin, and susceptible to clindamycin, gentamicin, tetracycline, vancomycin, linezolid, and trimethoprim/sulfamethoxazole (Fig. 2B). Each of the isolates was susceptible to mupirocin, although scattered colonies were found on the inhibition halo of the groin samples from the second visit.
Molecular typing showed that the strain belonged to the USA300 clone with its characteristic PFGE profile, spa-type t008, and ST8. The strain carried the SCCmecIVa cassette, the pvl gene encoding for the Panton-Valentine leukocidin (PVL), and the ACME complex characteristic of this clone—ACME-I (Fig. 3).
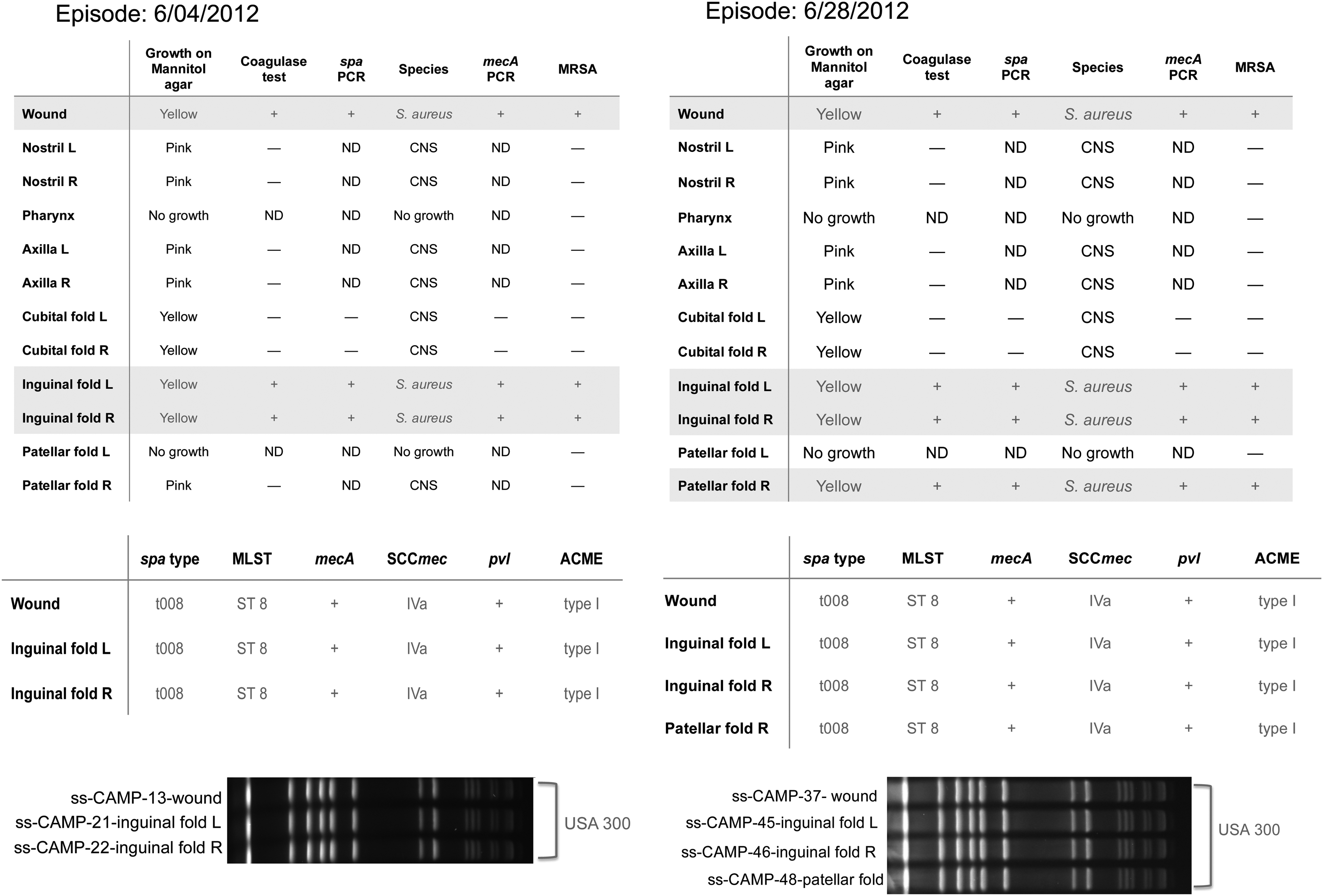
Sampling of different body sites for bacterial growth and identification of the MRSA strain by molecular typing. MLST, multilocus sequence typing.
Discussion
During the past decade, CA-MRSA has become an increasingly dominant source of SSTIs across North America,10,13,22 and USA300 is the predominant clone in the United States.23,27 The spread of USA300 has become global, is frequently associated with severe SSTIs, and is often involved with necrotizing pneumonia. 24 S. aureus colonization of the skin and nares is common, and the asymptomatic CA-MRSA nasal carriage is a strong predictor of subsequent SSTIs,7,33 however, extranasal colonization has also been documented, particularly in the perirectal and inguinal regions. 34 Among SSTIs, CA-MRSA is most commonly associated with folliculitis and furunculosis. 5 There is no accepted standard for the treatment and prevention of recurrent SSTIs caused by CA-MRSA beyond the CDC-IDSA guidelines, 14 although a recent study demonstrated positive results with a combined regimen of systemic antibiotics and nasal decolonization with topical mupirocin. 21
The nares are the primary site for screening asymptomatic carriers of S. aureus, however, the lower body is the most common location of CA-MRSA infections due to USA300. Analysis limited to the nasal flora may miss extranasal colonization,26,28,32 and some authors suggest screening the oropharynx, perirectal area, and groin.26,34 During this patient's first SSTI episode, a MRSA strain with the same clonal type as the one recovered from the skin wound was also recovered from the left and right inguinal folds. During the second episode, MRSA was recovered from the left and right inguinal folds and the right patellar fold, and all isolates were identified as USA300. Groin colonization by USA300 presents a higher risk for SSTI than colonization of the nares by the same strain or colonization of the groin by other PFGE profiles such as the closely related USA500. 15 SSTI recurrence is frequent when USA300 is the infective agent; some studies point to the ACME as a significant virulence factor.5,29
During each episode of infection, the bacteria recovered from the wound retained full susceptibility to TMP-SMX, and antibiotic treatment, in conjunction with I&D where feasible, resulted in clinical cure,9,16 yet the patient continued to return with infection recurrences apparently caused by the same MRSA strain. During the final episode, the patient received a 30-day course of doxycycline, which again resulted in clinical cure, and the patient has not since presented with an additional episode. Although the optimal regimen is unknown, both TMP-SMX and doxycycline are suggested for recurrent MRSA SSTIs by IDSA, 14 and doxycycline has been shown to be effective in the treatment of CA-MRSA SSTIs. 25
While the patient sustained clinical cure following doxycycline treatment, we hypothesize that the true interruption of the cycle of recurrent infection may be related to the elimination of an environmental source of the pathogen. Of note, the sister did not have any recurrent SSTIs after she left the patient's home. Decolonization protocols may be coupled with or follow treatment protocols for MRSA when infections are recurrent.11,14
Study limitations
One limitation of the present study was that the protocol was designed to develop an infrastructure and to detect and identify MRSA in our target population, but was not designed to track recurrences; therefore, isolates from the subsequent recurrences were not systematically collected for characterization. Another limitation was that we did not confirm MRSA eradication in the inguinal folds after antimicrobial therapy nor did we look for a potential reservoir, either in the household members or the environment. Current standard of care guidelines for treating MRSA in the outpatient setting suggest that there is not enough evidence to routinely recommend decolonization of the patient or household members or decontamination of household surfaces. 12 These approaches, which are effective in the intensive care unit setting, 11 are now being tested in a newly funded randomized clinical trial (PCORI, Grant # CER-1402-10800, PI: Jonathan N. Tobin) that will develop and evaluate a home-based intervention using promotoras to prevent reinfection and transmission of CA-MRSA.
Conclusion
The clinical history of this recurrent CA-MRSA infection demonstrates the need to identify whether clinical cure occurs due to the course of treatment (I&D and antibiotics) or due to the disappearance of the source, as well as to identify potential persistent biological (patient, household member, pet) and/or environmental (surfaces, fomites) reservoirs.4,19,20,30 Identification of chronic exposure source(s) is critical for implementing effective eradication strategies, including topical decolonization and surface decontamination.11,14 Future studies should examine how to implement evidence-based strategies to decontaminate environmental reservoirs and decolonize carriers to reduce recurrence and household transmission11,21 and test these strategies in household settings. Future studies should also examine whole-genome sequencing of the pathogen to determine whether particular genetic sequences are associated with a recurrent phenotype.
Summary
We present the clinical history of a patient with recurrent skin infections caused by a strain of CA-MRSA belonging to the USA300 clone. The strain was recovered repeatedly from wounds and lower body sites but never from the nares. The clinical history of recurrence strongly suggests the existence of a common environmental source of the MRSA strain.
Footnotes
Acknowledgments
Supported, in part, by a NIH-NCATS Grant #8 UL1 TR000043 (PI: Barry Coller, MD) and by a 2011 CTSA Community Engagement Administrative Supplement Award (PI: Jonathan N. Tobin, PhD). Funding was also obtained from the AHRQ Grant # 1 P30-HS-021667 (PI: Jonathan N. Tobin, PhD) and the NIH-NCATS Grant # UL1 TR000043-07S1. Also supported by PCORI Grant # CER-1402-10800 (PI: Jonathan N. Tobin, PhD).
Disclosure Statement
The authors do not have financial or other relationships with the manufacturer(s) of any commercial product(s) or provider(s) of any commercial service(s) discussed in this case report.